
Abstract
Background:
COVID-19 patients present with both elevated D-dimer and a higher incidence of pulmonary embolism (PE). This single-centre retrospective observational study investigated the prevalence of early PE in COVID-19 patients and its relation to D-dimer at presentation.
Methods:
The study included 1038 COVID-19-positive patients, with 1222 emergency department (ED) attendances over 11 weeks (16 March to 31 May 2020). Computed tomography pulmonary angiogram (CTPA) for PE was performed in 123 patients within 48 h of ED presentation, of whom 118 had D-dimer results. The remaining 875 attendances had D-dimer performed.
Results:
CTPA performed in 11.8% of patients within 48 h of ED presentation confirmed PE in 37.4% (46/123). Thrombosis was observed at all levels of pulmonary vasculature with and without right ventricular strain. In the CTPA cohort, patients with PE had significantly higher D-dimer, prothrombin time, C-reactive protein, troponin, total bilirubin, neutrophils, white cell count and lower albumin compared with non-PE patients. However, there was no difference in the median duration of inpatient stay or mortality. A receiver operator curve analysis demonstrated that D-dimer could discriminate between PE and non-PE COVID-19 patients (area under the curve of 0.79, p < 0.0001). Furthermore, 43% (n = 62/145) of patients with D-dimer >5000 ng/ml had CTPA with PE confirmed in 61% (n = 38/62), that is, 26% of >5000 ng/ml cohort. The sensitivity and specificity were related to D-dimer level; cutoffs of 2000, 3000, 4000, and 5000 ng/ml, respectively, had a sensitivity of 93%, 90%, 90% and 86%, and a specificity of 38%, 54%, 59% and 68%, and if implemented, an additional 229, 141, 106 and 83 CTPAs would be required.
Conclusion:
Our data suggested an increased PE prevalence in COVID-19 patients attending ED with an elevated D-dimer, and patients with levels >5000 ng/ml might benefit from CTPA to exclude concomitant PE.
Keywords
Strengths and limitations of this study
All patients over 11-week period were included.
In all, 81% of patients at emergency department presentation had results of D-dimer.
Addition of D-dimer increased the uptake of computed tomography pulmonary angiogram (CTPA).
Criteria for requesting CTPA were not evident in the notes.
Selection bias with overestimation of pulmonary embolism at presentation is a possibility.
Introduction
SARS-CoV-2 results in COVID-19 pneumonia and is responsible for the 2020/2021 pandemic, and in the majority, it is a self-limiting illness. However, in a considerable proportion of the population, particularly the elderly and those with significant comorbidities, acute respiratory distress syndrome, multi-organ failure and death are common1,2
Elevated D-dimer is a common finding in COVID-19 patients, and significantly elevated D-dimer at admission and in hospitalised patients, including intensive care, has been associated with poor prognosis and higher mortality.3–6 Several groups have now reported clinically significant thrombosis in pulmonary arteries on imaging in COVID-19 patients who are hospitalised as inpatients on wards and intensive care, with rates between 11% and 31%.7–10 Similar findings, including small vessel thrombosis, have been reported in autopsy studies.11,12 It has been proposed that the pulmonary emboli in COVID-19 represent de novo thrombus formation, secondary to local inflammation as opposed to being embolic in origin.13–15
In patients with COVID-19, D-dimer has been suggested as a biomarker for disease severity, representing coagulation activation secondary to ongoing inflammation and potentially thrombosis. The International Society on Thrombosis and Haemostasis guidance suggests that the degree of D-dimer increases may help identify patients who might benefit from admission 16 and pharmacological thromboprophylaxis. Updated guidance from the same organisation does not comment on screening for venous thromboembolic disease in the context of elevated D-dimer and reiterates the need for further studies. 17
Guidelines recommend a Bayesian approach to evaluate patients presenting with suspected venous thromboembolism (VTE), using clinical decision rules for estimating pretest probability based on a combination of predisposing conditions (malignancy, immobility, previous VTE, contraceptive use) and presenting symptoms (elevated heart rate, haemoptysis and low oxygen saturation). This is followed by D-dimer testing to increase the yield of a pulmonary embolism (PE) diagnosis by imaging.18–20 Current rules were validated before the COVID-19 pandemic, based on the estimated PE prevalence of the population studied. 19 Presently, although studies suggest an excess of VTE, there is no consensus on the clinical or laboratory criteria for identifying patients for diagnostic imaging although COVID-19 symptoms are indistinguishable from PE. Shortness of breath and chest pain are reported in around 60% and 20% of COVID-19 patients, respectively, and similarly, haemoptysis is reported in around 5%. 21
Patient selection for definitive imaging for PE diagnosis based on clinical parameters alone is challenging, and the use of clinical decision rules reflects this in routine clinical practice. 19 Individual clinicians in the context of COVID-19 have undertaken imaging based on their personal experience or local guidelines. While excess thrombosis has been documented in COVID-19, no studies have attempted to identify the highest risk period for developing PE. In our single-centre retrospective observational study, our primary objective was to establish the co-presentation of early PE with COVID-19. We defined early PE by the demonstration of thrombosis within 48 h of emergency department (ED) presentation, which potentially represents disease-related thrombus formation rather than uncomplicated embolisation from deep veins associated with hospitalisation. Our secondary objectives were the characterisation of the early PE patient cohort, including distribution of D-dimer at presentation, and investigation of the utility of D-dimer for distinguishing patients for computed tomography pulmonary angiogram (CTPA) for the diagnosis of PE.
Methods
Patients
Our hospital had more than 1500 COVID-19 attendances during the first peak between March 2020 and July 2020. The study period covered ED attendances over 11 weeks between 16 March and 31 May 2020. During this period, clinicians were guided by a COVID-19 Clinical Care Bundle to manage suspected and confirmed COVID-19 patients. This bundle was updated monthly and earlier as needed to reflect new local, national and international guidance, aiming to provide support to the clinician amid rapid changes in science and recommendations.
A dataset was created to record the basic clinical and demographic parameters of patients with COVID-19 presenting to the ED. Details collected included patient demographics, number of comorbidities, initial observations at triage, chest X-ray at presentation and CTPA, and routine laboratory results. Data were collected from the ED electronic medical record, CERNER Millennium (Cerner Corp., Kansas City, MO), and data for missing fields were identified from the scanned handwritten ED notes.
A patient was considered to have COVID-19 for this analysis if they were positive by real-time reverse transcriptase polymerase chain reaction (RT-PCR) for SARS-CoV-2 RNA (n = 700) or had findings on chest X-ray or CT scan consistent with COVID-19. For analysis of early PE, patients with a CTPA undertaken within 48 h were included; anticipated due to significant workflow demands, failure to respond to initial therapy and clinical instability, this was decided a priori. National research ethics committee does not require patient consent for data review to facilitate audit or service development. Further more, health research authority UK has waived the consent for research based on COVID-19 data. 22 There was no involvement of patients or the public in the design of this study.
Investigations
SARS-CoV-2 RNA was detected by real-time RT-PCR on a nasopharyngeal or throat swab. All patients had chest X-ray. The CTPA was conducted on a Toshiba Aquilion Prime (Canon Medical Systems, USA) 80-MDCT scanner within 48 h of admission. Images acquired following administration of 50 ml of intravenous contrast at 4 ml/s through an 18–20G cannula in an upper limb vein were reviewed on a PACS workstation (Carestream). The images were evaluated for thrombus from the main pulmonary artery down to the subsegmental level.
D-dimer was analysed using the Innovance® D-dimer assay (Siemens Healthcare Diagnostics Products GmbH, Marburg, Germany) on a CS5100 coagulometer (Sysmex, Kobe, Japan) according to the manufacturer’s instructions, and results were reported in ng/ml fibrinogen-equivalent units (FEU). The upper limit of normal in the hospital was 400 ng/ml.
Statistical analysis
Descriptive statistics were used to describe the cohorts with and without CTPA and the presence of PE. Baseline characteristics of patients with and without PE were compared using the Mann–Whitney test, and significance was set at p < 0.05. R software was used for this statistical analysis. In the CTPA cohort, a receiver operating characteristic (ROC) analysis was undertaken to investigate the potential for D-dimer and other significant variables identified in the between-group analysis to predict the presence of PE. The ROC analysis provided sensitivity and specificity values for different D-dimer cutoff values for diagnosing PE by CTPA, in patients with COVID-19. This was performed using MedCalc version 19.2.3 (MedCalc Software Ltd, Ostend, Belgium) to calculate the standard error of the area under the curve (AUC). We also modelled the requirement of additional CTPAs for different cutoffs in the cohort of patients with D-dimer results but no CTPA within 48 h of presentation.
Results
Baseline characteristics
The retrospective data review identified 1038 patients with 1222 patient attendances with a confirmed diagnosis of COVID-19. The number of COVID-19 patient attendances across 11 weeks, along with the number with D-dimer and CTPA results, are presented in Figure 1. It is evident from the graph that the number of CTPAs increased with the introduction of D-dimer into the care bundle.

Patient attendances secondary to COVID-19 over 11 weeks.
Over the 11 weeks, some patients were seen on more than one occasion. Of the total 1222 attendances, 1038 attendances represented a patient’s first visit, 149 attendances were a second visit and 35 attendances represented the third to fifth visit. When the attendances were analysed for the duration of symptoms before presentation to the ED, 692 attendances were seen within 7 days of symptom onset, 361 attendances were seen between 8 and 14 days, and 169 attendances were seen 15 days or more. In the last group, 73 attendances were documented as first visit, with 67 representing second visit and 29 third visit or more.
Early PE was considered to be present if a thrombus was identified within the first 48 h of attendance, as this is likely to represent thrombosis that had developed preadmission. Of the 1038 unique patients, a total of 277 (26.7%) patients underwent CTPA in the 11 weeks, of which 123 patients underwent CTPA within 48 h of ED presentation (11.8%), and 107 scanned within 24 h.
In the 1222 COVID-19-positive attendances, D-dimer results were available for 81.3% (n = 993). Common reasons for the lack of D-dimer results included request not made, haemolysed samples and repeat collection failure.
Baseline clinical and laboratory characteristics of the COVID-19-positive cohort, categorised by use of CTPA and the detection of PE, are described in Tables 1 and 2, respectively. The non-CTPA cohort includes 753 unique patients with D-dimer results.
Baseline clinical characteristics of patients with and without CTPA.

CTPA, computed tomography pulmonary angiogram; IP, inpatient; IQR, interquartile range; PE, pulmonary embolism.
Data are presented as n (%) unless otherwise indicated; ***p < 0.001; **p < 0.01; and between-group comparison was done for patients with and without PE by Mann–Whitney test.
Baseline routine blood tests at emergency department presentation.

ALT, alanine aminotransferase; APTT, activated partial thromboplastin time; AST, aspartate aminotransferase; CK, creatine kinase; CTPA, computed tomography pulmonary angiogram; HCT, haematocrit; INR, international normalised ratio; IQR, interquartile range; PE, pulmonary embolism; RBC, red blood cells; WBC, white blood cells.
Mann–Whitney test between-group comparison was done for patients with and without PE; ***p < 0.001; **p < 0.01; *p < 0.05.
Median (IQR) provided by more than 50% of the cohort had data for the variable, and no data are denoted by NA.
Outliers with values greater than 2.0 were removed from the analysis.
Pulmonary embolism/thrombosis on CPTA
Of the 123 patients who had CTPA within 48 h of arrival in the hospital, PE was identified in 46 patients (37.4%), and 77 patients had no demonstrable thrombus (62.6%). In this group of 123 patients, 118 had D-dimer results. The median duration of symptoms before imaging was 7 days at the first visit (n = 94) and 20 days for the second (n = 20) and third visit or greater (n = 6), which are 9%, 15% and 17% of the respective visits. Between-group comparison of patients with positive and negative CTPA shows that patients with PE had significantly higher C-reactive protein(CRP), troponin and total bilirubin, with lower albumin suggesting greater disease severity (Tables 1 and 2). The group also had a significantly higher total white blood cell (WBC) count, which was predominantly a neutrophilia. The coagulation screen shows higher prothrombin time (PT) with higher D-dimer. There was no difference in the presence of comorbidities or ethnicity of the patients. Notably, there was no difference in the median duration of inpatient stay or mortality following diagnosis and treatment. A binomial logistic regression was performed to ascertain the effects of continuous variables D-dimer, PT, CRP, troponin, albumin, total bilirubin, WBC and neutrophils on the dependent variable of the identified PE. Of the eight predictor variables, only D-dimer was found to be statistically significant, with increasing D-dimer being associated with an increased likelihood of PE.
The thrombus location was reviewed in relation to the pulmonary vasculature and right ventricular (RV) strain. Four patients had a thrombus in the main pulmonary artery without RV strain, and nine patients had a thrombus in the main pulmonary artery with RV strain. Thrombus limited to lobar vessels was seen in six patients, segmental vessels in eight patients and subsegmental branches in five patients. Extensive thrombus across more than one type of vessel with RV strain was seen in 10 patients, and similarly extensive thrombus without RV strain was seen in four patients.
D-dimer ROC analysis for the detection of a PE on CTPA
An ROC analysis evaluated the ability of D-dimer and other significant variables to discriminate patients with and without PE by CTPA. The ROC analysis results are provided in Table 3, which details the variable, associated AUC, p-value, optimal cutoff, and linked specificity and specificity. D-dimer had the highest AUC, and a comparison of ROC curves demonstrated D-dimer had a higher AUC compared with PT, neutrophils, CRP, troponin, albumin and total bilirubin. There is no significant difference between D-dimer and WBC. The ROC of D-dimer for the diagnosis of PE in the ED is presented in Figure 2. The cohort for this analysis included 118 COVID-19-positive patients who had results of both CTPA and D-dimer. The ROC curve demonstrated an AUC of 0.799 with a p-value of <0.0001, demonstrating that D-dimer is good to excellent in discriminating between patients with and without PE by CTPA, in patients with COVID-19.
ROC analysis of significant laboratory variables for prediction of PE present on CTPA.

AUC, area under the curve; CRP, C-reactive protein; CTPA, computed tomography pulmonary angiogram; PE, pulmonary embolism; PT, prothrombin time; ROC, receiver operating characteristic; WBC, white blood cells.

The solid blue line represents the ROC curve, AUC = 0.799, with a 95% confidence interval of 0.716–0.868 and a p-value of <0.0001. D-dimer is the predictor variable, and the presence and absence of PE by CTPA are the classifier variable. Data correspond to all samples with CTPA and D-dimer (N = 118).
Stratified D-dimer results and modelling of different D-dimer cutoffs for imaging
Table 3 provides D-dimer results for all patients stratified by the absolute increase. Normal levels were seen in 17% of the attendances, an elevation of <2000 ng/ml was seen in half of the patients (52%) and 32% had D-dimer >2000 ng/ml and 15% >5000 ng/ml.
A CTPA was performed in 43% (n = 62/145) of patients with D-dimer >5000 ng/ml, and within the scanned group, 61% (n = 38/62) had a detectable thrombus. The 5000 ng/ml threshold is 10 times the conventional threshold of 500 ng/ml, used during VTE evaluation. The results suggest an association between increasing D-dimer levels and presence of thrombosis.
Table 4 presents the sensitivity and specificity of some chosen D-dimer cutoffs. A cutoff of 2000, 3000, 4000, and 5000 ng/ml, respectively, had a sensitivity of 93%, 90%, 90% and 86% and a specificity of 38%, 54%, 59% and 68%. At these cutoffs, 27% (229), 17% (141), 13% (106), and 10% (83) of the non-CTPA, D-dimer attendances would have required a CTPA.
D-dimer results at presentation stratified.

CTPA, Computed tomography pulmonary angiogram; PE, pulmonary embolism.
Discussion
In this single-centre retrospective observational study, we report the presence of early PE on CTPA in a subgroup of patients with COVID-19 within 48 h of presentation to the ED. A CTPA undertaken in 11.8% (n = 123) of the patients demonstrated PE in 37.4%. All of these patients had elevated D-dimer, and in the group with D-dimer >5000 ng/ml, 42% had a CTPA, of which PE was observed in 61% of patients.
A recent systematic review of 86 studies has given a VTE prevalence of 7.9% [95% confidence interval (CI), 5.1–11.2] in non–intensive care unit (ICU), and 22.7% (95% CI, 18.1–27.6) in ICU patients, although individual studies vary widely in VTE prevalence. 23 Although it has been postulated that the pulmonary thrombus represents de novo thrombus formation, the CTPA appearances do not distinguish de novo thrombus from one that is embolic in origin. In a cohort of 388 COVID-19 hospitalised patients, no symptomatic deep vein thrombosis (DVT) was seen. Furthermore, 64 patients in the same cohort underwent a Doppler ultrasound of the lower limbs with no identifiable thrombus. 15 However, a multicentre study that assessed pretest probability in the ED with a revised Geneva score demonstrated a similar VTE prevalence of 15% in patients with and without COVID-19, suggesting the current clinical decision rules may not aid to identify COVID-19 patients with PE. 24
Patients with PE had significantly higher CRP, troponin, total bilirubin and neutrophils with lower albumin, suggesting severe disease. Indeed, CRP is a recognised marker of prognosis and disease activity.1,25,26 Interestingly, our data demonstrate that the addition of D-dimer to the care bundle order set increased the number of CTPA requests over time. Furthermore, elevated D-dimer was markedly different between the groups with a p-value of <0.001. Studies of COVID-19 patients have also suggested a potential correlation between D-dimer and the severity of the disease.27,28
The ROC also confirmed that D-dimer was the most useful variable in discriminating patients with and without PE by CTPA (AUC of 0.79, p < 0.0001). In an ROC analysis of 81 ICU COVID-19 patients with 20 patients demonstrating VTE, a D-dimer cutoff of 1500 ng/ml was reported to have a sensitivity of 85.0% and a specificity 88.5%. 5 In another cohort, a D-dimer of 2660 ng/ml was detected in all the positive patients. 9 In our cohort, D-dimer of >5000 ng/ml had a specificity of 88.0% with a sensitivity of 84.0%, with lower values having a marked impact on the specificity with increased sensitivity. Higher cutoffs, age-adjusted in the older population 29 and cancer inpatients, 30 have previously been noted to have better predictive value. A recent study of 242 COVID-19 patients suggested the elevated D-dimer was predictive of PE on CTPA during hospitalisation, and ROC analysis had an AUC of 0.79, with a sensitivity of 81% and a specificity of 59% for a cutoff of 2903 ng/ml. 31
There are several limitations to this study, all which may have resulted in a selection bias. First, there was no clinical guideline or decisions rules associated with selecting patients for CTPA with COVID-19, which was done on clinician gestalt in the initial stages. Furthermore, the lack of detailed information about medical comorbidities might limit the value of the observations. The introduction of a COVID-19 order-set on 22 March alongside a ‘Clinical Bundle of Care’ that included the D-dimer saw a rise in the number of CTPA request. Early in the pandemic, most patients were advised to self-isolate, and potentially, the development of PE might have precipitated an ED visit due to an increase in the severity of symptoms. In our clinical practice, worsening hypoxaemia on ICU has become an indication for CTPA, and treatment appeared to be associated with symptomatic improvement. (Table 5)
ROC analysis: sensitivity and specificity of different cutoffs.
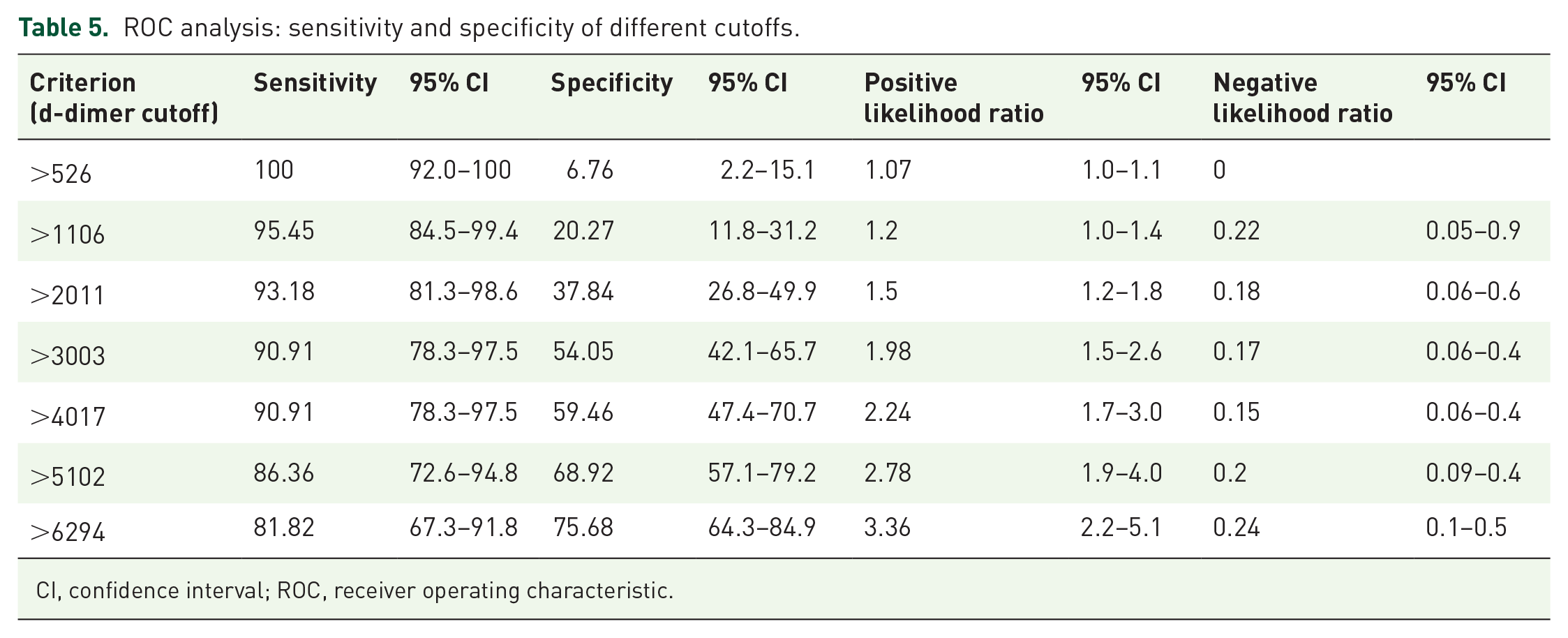
CI, confidence interval; ROC, receiver operating characteristic.
Our data raise several important questions. Current treatment strategies focus on anti-viral or anti-inflammatory medications and do not require any screening for pulmonary thrombosis. In our opinion, the control of infection and limitation of inflammation may prevent further progression, but clot resolution is hastened by full anticoagulation, and it is plausible this would be similarly relevant in this cohort of patients. Indeed, the median duration of inpatient stay and mortality was similar between the groups despite the suggestion of more severe disease in patients with PE, which may be related to treatment.
Small randomised control trials of anticoagulation of different intensity in COVID-19 without screening for PE have suggested a potential benefit of enhanced anticoagulation in patients with a non-severe disease requiring supplemental oxygen but not severe disease requiring ventilatory support, invasive and non-invasive. A strategy of early diagnosis and treatment may have more gains. Prospective cohort studies of PE prevalence and relationship to D-dimer and currently used clinical decision rules are required as this diagnosis would result in patient anticoagulation post-discharge, unlike prophylactic anticoagulation strategy.
In summary, our study confirms the findings of previous studies of an excess of thrombosis in pulmonary arteries in patients with COVID-19. We have demonstrated PE early in the disease and association with elevated D-dimer, particularly at levels >5000 ng/ml. Furthermore, as PE symptoms are indistinguishable from those of COVID-19 pneumonia, D-dimer could potentially identify patients for further imaging, pending the development of clinical decision rules. It is crucial that we continue to diagnose complications of COVID-19 that might impact the mortality and morbidity of patients.
Footnotes
Acknowledgements
We thank Adrian Fogarty for copywriting and editing the document.
Author contributions
TS proposed the study. AP, TS and JJ established the RFLCOVID-19 dataset and collected the data. AP and PC contributed to the data analysis. All authors contributed to the review of data interpretation, writing of the manuscript, and critically reviewed and approved the final version of the manuscript.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Data sharing
No additional data available.