
Abstract
Venetoclax in combination with hypomethylating agents (HMAs) or low-dose cytarabine (LDAC) has demonstrated exceptional activity in elderly and unfit patients with newly diagnosed acute myeloid leukemia (AML). Notably, the safety profile of venetoclax-based induction regimens was favorable, with a low rate of early treatment-related mortality, even in frail study participants. Thus, the introduction of venetoclax has transformed the landscape of AML therapy in elderly patients. Given these promising results, venetoclax in combination with other agents is now being studied as a frontline therapy in younger patients with AML, as well as in relapsed/refractory AML patients. Here, we review clinical data for venetoclax-based therapy in AML, both from prospective as well as retrospective studies, and highlight ongoing novel studies of venetoclax-containing regimens and discuss future research directions.
Introduction
The incidence of acute myeloid leukemia (AML) increases with age, with a median age of 68 years at the time of diagnosis. There is a correlation between increased age and inferior outcomes in AML. The 5-year overall survival (OS) for patients >55 years diagnosed with AML is in the range of ~10%, and long-term survival has only modestly improved in the past several decades, despite the progress in supportive care and the application of allogeneic hematopoietic cell transplantation (alloHCT) to older patients.1,2
The poor survival of elderly patients is partially due to age-related factors such as frailty and pre-existing co-morbidities that accompany older age, and this situation creates obstacles towards administering standard intensive induction regimens [such as idarubicin + cytarabine (7+3)]. In addition, AML diagnosed at an advanced age frequently harbors high-risk clinico-pathogenetic features including an origin from antecedent hematological disorders as well as the presence of adverse risk mutations and cytogenetic abnormalities, both of which confer resistance to conventional chemotherapies. 3 Therefore, what are considered standard induction regimens for AML are only beneficial in fewer than half of all newly diagnosed patients as a result of their poor tolerability as well as low response rate, particularly in patients with an adverse genetic risk. As a consequence, frail and elderly patients with newly diagnosed AML were historically offered low intensity treatments, such as single-agent hypomethylating agents (HMAs) or low-dose cytarabine (LDAC) which have a very low likelihood of inducing response or prolonging survival.
B cell lymphoma-2 (BCL-2) family proteins are key regulators of intrinsic apoptosis pathways, and the BCL2 family of genes encode related proteins that mediate either pro-apoptotic or anti-apoptotic activity, with the balance between these proteins determining either survival or apoptosis. Venetoclax, previously known as ABT-199, is a selective, potent BCL-2 inhibitor that leads to apoptosis by binding directly to BCL-2, displacing pro-apoptotic proteins and thereby triggering mitochondrial outer membrane permeabilization and activation of caspases. 4 Venetoclax has shown significant activity across various subtypes of leukemias, including chronic lymphocytic leukemia, AML, and acute lymphoblastic leukemia (ALL).5–8
BCL-2 expression is high in AML, including in leukemia stem cells (LSCs), 9 which justified targeting BCL-2 in this setting. Clinical studies have proved the effectiveness of this approach. The introduction of venetoclax-based therapies in untreated, unfit patients with AML has transformed the frontline therapy of AML in elderly patients, and the remarkable activity of these combinations is re-shaping the landscape of frontline therapy in AML across all ages as well as in advanced AML.
Venetoclax-based induction therapy in AML patients unfit for intensive chemotherapy
Venetoclax-based combinations, either with HMAs or LDAC, are now approved for newly diagnosed unfit or elderly patients with AML. The approval of venetoclax was based on two separate phase II clinical studies that enrolled older and unfit patients who were considered ineligible for intensive regimens, either because of advanced age or co-morbidities.6,10 Subsequently, a phase III randomized study has confirmed efficacy by demonstrating improved response rates and overall survival compared to standard of care. 11
Two venetoclax (VEN) combination studies, one with HMAs and one with LDAC, shared similar inclusion criteria, with the exception that the HMA study did not allow enrollment of patients who were previously treated with HMAs for antecedent myelodysplastic syndrome, whereas the LDAC study did not restrict enrollment on the basis of prior exposure to HMAs, and patients with this exposure comprised 29% of the study group. 10 Both studies excluded patients with favorable risk cytogenetics, and the study populations were enriched with high-risk patients either because of older age, secondary or therapy-related leukemia, or high-risk genetic profile.
The rates of complete remission (CR) and CR with incomplete hematological recovery (CRi) were 73% and 54% in the VEN-HMA and VEN-LDAC studies, respectively.6,10 The time to CR/CRi was short, at 1.2–1.4 months. Minimal residual disease (MRD) less than 10–3 was achieved in 29% of evaluable patients who achieved CR/CRi with VEN-HMA. 6 The median OS and duration of response were 17.5 and 11.3 months in the VEN-HMA study and 10.1 and 8.1 months in the VEN-LDAC study, respectively.6,10 A comparably high response rate (CR/CRh = 63%) with VEN-HMA was also reported from real-world experience published by researchers at the University of Colorado. 12
A phase III randomized study (VIALE-A) comparing azacitidine alone or in combination with venetoclax in patients with newly diagnosed AML who were ⩾75 years or <75 years and had co-morbidities, has met the primary endpoints of OS (Hazard ratio [HR] = 0.66; 95% confidence interval [CI]: 0.52–0.85; p < 0.001) (14.7 versus 9.6 months) and composite CR rate (66% versus 28%, p < 0.001) at the first interim analysis, favoring the combination regimen. 11 A phase III randomized study (VIALE-C) of LDAC with or without venetoclax in unfit newly diagnosed AML patients was reported recently, and in contrast, it did not meet the primary endpoint of OS (7.2 months versus 4.1 months, p = 0.11); however, post-hoc analysis after an additional 6 months follow up showed significant improvement in median OS in the venetoclax arm compared to placebo (8.4 versus 4.1 months, p = 0.04). Nonetheless, composite CR rate was higher in the venetoclax + LDAC arm compared to placebo + LDAC (48% versus 13%, p < 0.001). 13 Refer to Table 1 for venetoclax based studies in newly diagnosed AML.
Studies for venetoclax-based therapy in newly diagnosed AML.
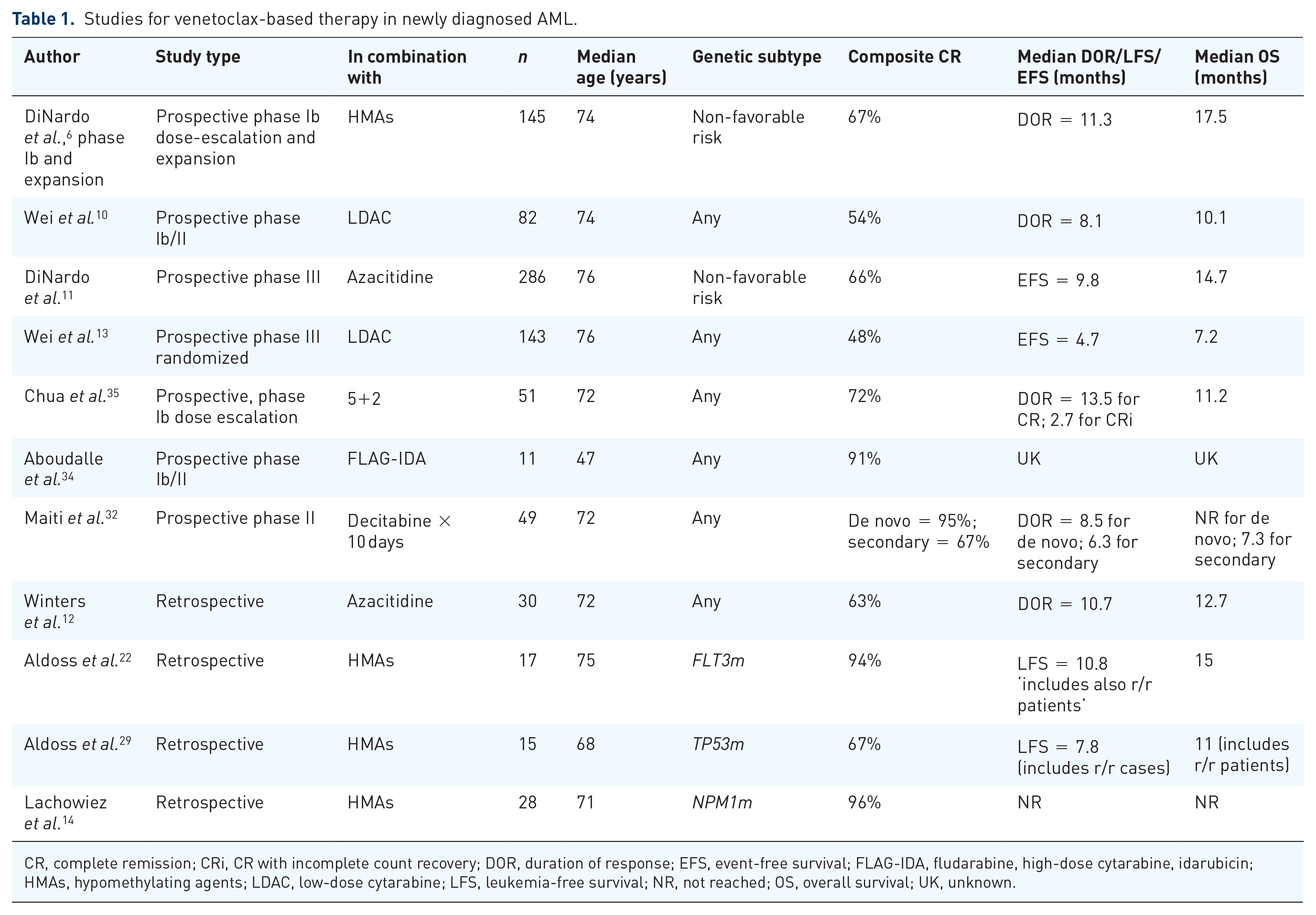
CR, complete remission; CRi, CR with incomplete count recovery; DOR, duration of response; EFS, event-free survival; FLAG-IDA, fludarabine, high-dose cytarabine, idarubicin; HMAs, hypomethylating agents; LDAC, low-dose cytarabine; LFS, leukemia-free survival; NR, not reached; OS, overall survival; UK, unknown.
These previously mentioned studies universally included patients who were ineligible for intensive induction therapy either because of older age (⩾75 years) or the presence of co-morbidities such as congestive heart failure, chronic stable angina, impaired lung function, moderate hepatic or renal impairment, prior exposure to anthracyclines, or poor performance status. Almost half of all included patients in these studies were <75 years and had pre-existing co-morbidities, and many of these patients had more than one factor rendering them ineligible for an intensive induction regimen.6,13,14
Figure 1 shows the dosing schema and timing of bone marrow biopsy of four lower-intensity venetoclax-based regimens.

Four low-intensity, venetoclax-containing regimens.
Venetoclax-based therapy for relapsed/refractory AML
Single-agent venetoclax was administered at a 800 mg daily dose in relapsed/refractory (r/r) AML patients in a phase II study, and this trial showed only a modest activity (CR/CRi = 19%). 5 Therefore, venetoclax as a monotherapy did not generate considerable interest in the advanced AML setting. In contrast, the high activity of venetoclax in combination with HMAs in the frontline setting led to extending the use of the combination regimen to r/r AML patients, and several prospective and retrospective studies were reported on its activity.
At City of Hope (COH), we have reported a CR/CRi rate of 46% in 90 patients with r/r AML treated with VEN-HMA, with a median time to achieve CR/CRi of 1 month. Among responders who had MRD testing performed, 64% achieved a MRD negative (MRD–) response. The cohort included high-risk patients, among whom 32 (35%) had therapy-related/secondary AML, 46 (51%) had prior HMA therapy and 26 (29%) had failed prior alloHCT. The median OS was 7.8 months for all patients and 16.6 months for patients achieving CR/CRi. 15 In contrast, investigators at MD Anderson Cancer Center (MDACC) reported a CR/CRi/morphological leukemia-free state (MLFS) rate of 21% in 43 consecutive patients with various myeloid malignancies (including myelodysplastic syndrome and blastic plasmacytoid dendritic cell neoplasm) who were treated with venetoclax in combination with HMAs, LDAC or chemotherapy. 16 The MDACC study population and treatments were different from those in the COH experience, which may explain to some extent the disparity in results. In another report from Taiwan comprising 40 patients with r/r AML who received venetoclax-based therapies (including single-agent venetoclax or with HMAs, LDAC, or chemotherapy), the CR/CRi rate was 22.5%, with an additional five patients achieving MLFS and another six attaining partial response. 17
Among 23 AML patients who either relapsed or were refractory to HMAs, a venetoclax combination regimen [with HMAs (87%) or LDAC (13%)] led to a 43% CR/CRi rate, as reported by Ram et al. 18 In another cohort restricted to patients with relapsed AML post alloHCT (n = 21), eight (38%) patients achieved CR/CRi with venetoclax-based regimens. 19 In our experience, neither prior HMA treatment nor failing alloHCT resulted in an inferior response to VEN-HMA in the r/r AML setting. 15
In a noteworthy small cohort study of patients with AML who carried the NPM1 mutation (n = 12) and had either relapsed or remained with persistent molecular MRD, 92% achieved MRD negativity after one or two cycles of venetoclax with HMAs or LDAC. 20
In a prospective study combining venetoclax with 10 days of decitabine in different AML settings, 83 patients were treated for r/r disease. The CR/CRi rate was 39% and 42% in secondary and de novo r/r AML, in addition to an MLFS rate of 21% and 18%, respectively. 21
These results, although mostly retrospective in nature, provide evidence of the encouraging activity of venetoclax-based therapy in r/r AML including in patients who have relapsed after alloHCT. See Table 2 for venetoclax-based studies in r/r AML.
Studies for venetoclax based therapy in r/r AML.
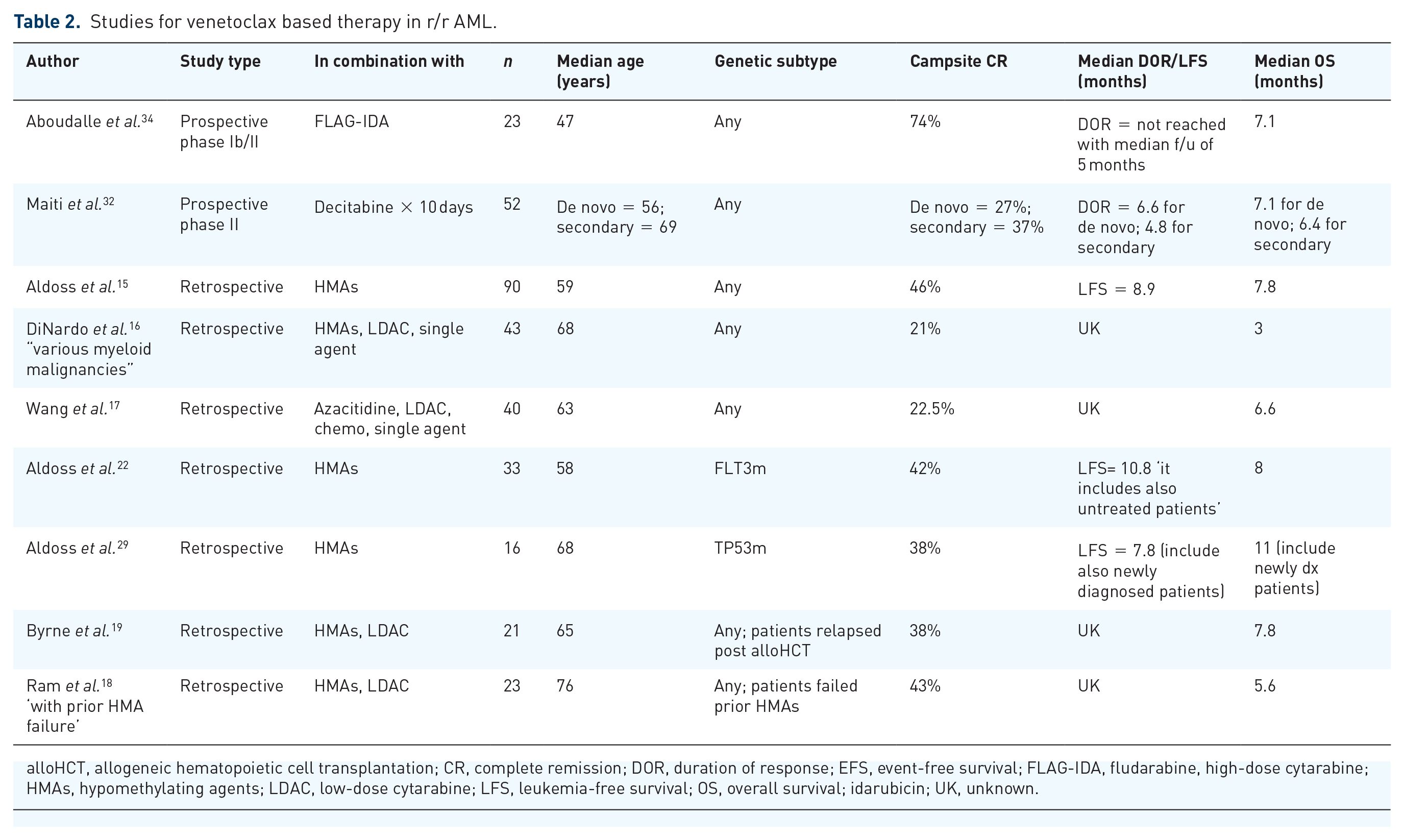
alloHCT, allogeneic hematopoietic cell transplantation; CR, complete remission; DOR, duration of response; EFS, event-free survival; FLAG-IDA, fludarabine, high-dose cytarabine; HMAs, hypomethylating agents; LDAC, low-dose cytarabine; LFS, leukemia-free survival; OS, overall survival; idarubicin; UK, unknown.
The impact of leukemia genetics on outcome of venetoclax-based therapy in AML
Venetoclax-based regimens have proved to be efficacious in AML with adverse risk cytogenetics, although response appears to be lower and short-lived compared to cases with intermediate risk cytogenetics. DiNardo et al. reported CR/CRi rates of 60% and 74% for VEN-HMA in patients with unfavorable and intermediate risk cytogenetics, respectively. 6 In a phase II study, 10 Wei et al. showed that, when combined with LDAC, venetoclax produced CR/CRi rates of 42% and 63% in unfavorable and intermediate risk cytogenetics, respectively. In the randomized VIALE-C study, CR/CRi rates among patients with unfavorable risk AML were 28% with VEN-LDAC and were 10% with LDAC and placebo. 13 In the r/r AML setting, adverse risk genetics according to the 2017 European LeukemiaNet (ELN) classification also influenced the CR/CRi rate to VEN-HMA adversely compared to intermediate risk genetics (34% versus 65%). In contrast, the response rate was impressive in r/r AML patients harboring favorable risk genetics (75%) thereby further validating the utility of genetic risk stratification of AML as a predictor of response to VEN-based combination therapy. 15
Remarkably, venetoclax-containing regimens were associated with impressive response rates across high-risk molecular mutations in AML, especially when HMAs were included in the combination. In the frontline setting, venetoclax with either HMAs or LDAC produced CR/CRi rates of 47% and 18–30%, respectively, in AML with TP53m.6,10,13 In a retrospective analysis from COH that was restricted to TP53m AML patients (n = 31) treated with VEN/HMA, we showed a CR/CRi rate of 67% and 38% in newly diagnosed and r/r patients, respectively. Likewise, in untreated patients, venetoclax with either HMAs or LDAC produced CR/CRi rates of 72% and 45% in FLT3m AML, respectively.6,10,13 In a retrospective analysis limited to FLT3m AML patients treated with VEN-HMA (n = 50) from our institution, CR/CRi rates were 94% and 42% in newly diagnosed and r/r patients, respectively. 22 We have observed no difference in response to VEN-HMA with regard to the type of FLT3 mutation (ITD versus TKD) or the allelic ratio of the FLT3-ITD mutation. 22 Interestingly, acquired TP53 and FLT3 mutations were observed at the time when AML became resistant to VEN-HMA. 23 There is a suggestion that mutations in PTPN11 can potentially confer resistance to venetoclax therapy in AML by enhancing the expression of other anti-apoptotic genes such as BCL-XL and MCL-1. 24 In the r/r AML setting, we have observed a superior response in AML carrying TET2 and ASXL1 mutations, and a trend towards inferior response in patients harboring the U2AF1 mutation. 15
Consistently among several reports, IDHm AML was associated with a high response rate and durability of remissions with venetoclax-based therapies.5,6,10,23 This sensitivity of IDHm AML to venetoclax seems related to decreased cytochrome c oxidase activity in the mitochondria that makes these cells more susceptible to apoptosis on BCL2 inhibition. 25 Similarly, VEN-HMA therapy was associated with a very favorable composite CR rate in older (>65 years) AML patients with the NPM1 mutation (96%), and the response rate as well as OS were superior with VEN-HMA compared to intensive induction regimens in a paired-matched historical cohort of NPM1m AML patients.23,26
Although the CR/CRi rate following VEN-HMA treatment appears favorable among AML with high-risk genetics, responses seem short-lived. In the frontline setting, the median duration of response (DOR) [6.7 (4.1–9.4) versus 12.9 (11–not reached) months] and OS [9.6 (7.2–12.4) versus not reached (17.5–not reached) months] were lower in poor-risk cytogenetics compared to the intermediate risk group. Similarly, patients with TP53m AML treated with VEN-HMA had a median DOR and OS of 5.6 and 7.2 months, respectively. In NPM1m, the median DOR and OS were not reached, and in IDHm, the median DOR and OS were not reached and 24.4 months, respectively. 6
The choice between HMAs and LDAC, and the type and duration of HMAs in combination with venetoclax
Although the response rate appears higher with venetoclax when combined with HMAs compared to LDAC on the basis of published single-arm phase II/III studies, these combinations have never been compared head to head in a randomized fashion, and individual studies enrolled different patient populations. One key distinction between these studies is the allowance of prior HMAs in the VEN-LDAC studies but not in the VEN-HMA studies, as mentioned before. Prior exposure to HMAs predicts a lower response rate across various induction regimens in AML,27,28 including VEN-LDAC. 10 In fact, the CR/CRi rate to VEN-LDAC was as high as 62% when analysis was restricted to HMA-naïve patients with AML, 10 a rate approaching what was observed with VEN-HMA in this setting. 6
Nonetheless, it is noteworthy to mention that the efficacy of VEN-HMA combinations has been reported after prior exposure to HMAs in retrospective studies. In r/r AML, prior HMA treatment did not predict response (41% versus 50%, p = 0.53) to VEN-HMA in our experience. 15 However, we have observed lower responses to VEN-HMA in AML patients carrying TP53m and who had prior treatment with HMAs, compared to those naïve to HMAs (14% versus 63%, p = 0.025). 29 This result could be due to the known sensitivity of TP53m AML to HMAs, particularly with a prolonged course of decitabine. 30
Therefore, both HMAs and LDAC are reasonable options to combine with venetoclax in untreated unfit patients with AML; however, only the VEN-HMA combination has demonstrated OS benefit in a phase III randomized study. Nonetheless, for AML patients with prior HMA treatment, especially if HMA administration was recent, it is reasonable to choose VEN-LDAC over VEN-HMA given the lack of prospective data supporting the true benefit of VEN-HMA in this setting. However, for patients who had a remote history of treatment with HMAs, we believe that VEN-HMA represents a reasonable choice based on retrospective data.
If the decision is made to combine VEN with HMAs, outcomes appear comparable using either a 5-day course of decitabine or a 7-day course of azacitidine, as was administered in the phase I/II studies, in which the choice of HMA was left to the treating institution to decide between both options. 6 However, preclinical experiments showed the potential ability of azacitidine in combination with VEN for eradicating LSCs. 31 Such activity on LSCs with decitabine, although possibly similar, it is not known at this time. The phase III randomized study used only azacitidine in combination with venetoclax or placebo, which may lead to increasing use of this combination in the community.
With the excellent tolerability of standard VEN-HMA regimens in published studies, intensifying decitabine by prolonged administration over 10 days was attempted to enhance the efficacy further. In a single-center prospective study from MDACC utilizing a 10-day schedule of decitabine in the first cycle, together with VEN, in 101 newly diagnosed and r/r AML patients, CR/CRi rates were 95% in de novo untreated AML, 67% in untreated secondary AML, 37% in r/r secondary AML, and 27% in de novo r/r AML. 32 Data from other retrospective studies showed no significant differences in outcomes, including in AML with TP53m.15,29 This finding is not surprising, as a recent randomized study failed to showed superiority of 10 over 5 days decitabine administered to newly diagnosed AML patients. 33 Therefore, there is no demonstrated benefit at this time of administering 10 courses of decitabine versus the standard 5-day regimen.
Venetoclax in combination with conventional chemotherapy regimens in AML
Given the promising activity of venetoclax in AML and the non-overlapping toxicity profile with conventional cytotoxic chemotherapeutic agents, with the exception of myelosuppression, venetoclax has been tested in combination with intensive salvage regimens in fit patients with AML.
Investigators at MDACC administered venetoclax in combination with fludarabine, high-dose cytarabine and idarubicin (FLAG-IDA) in newly diagnosed and r/r AML in an ongoing phase Ib/II study [ClinicalTrials.gov identifier: NCT03214562]. 34 Of 23 patients with r/r AML, the composite CR rate was 74%, while 91% (10 out of 11) of untreated AML patients achieved composite CR. The early treatment mortality rate was low (13% in r/r and 0% in newly diagnosed), and among the three early deaths in r/r AML, two were attributed to disease progression and one to fungal pneumonia.
In a phase Ib study (CAVEAT) that enrolled fit, older patients (median 73 years) with newly diagnosed AML, 51 were treated with venetoclax in combination with a 2-day idarubicin and 5-day cytarabine (5+2) regimen. The CR/CRi rate was 72%, and it was 97% and 43% in de novo and secondary AML patients, respectively. The median OS for the whole population was 11 months, and early death occurred in four patients. 35
There are ongoing clinical studies combining venetoclax with other chemotherapeutics, such as VEN in combination with liposomal daunorubicin and cytarabine (CPX 351, Vyxeos) in newly diagnosed fit AML patients lacking targetable mutations [ClinicalTrials.gov identifier: NCT04075747] as well as in older and unfit newly diagnosed AML patients [ClinicalTrials.gov identifier: NCT04038437].
Although combining VEN with standard intensive chemotherapy is intriguing, this approach should be compared head to head with VEN in combination with HMAs or LDAC, as toxicities are expected to be increased with these intensive regimens, especially the periods of cytopenia and associated complications.
Adverse event profile and supportive care
When VEN is combined with HMAs or LDAC, the induction mortality is low even in frail and elderly patients with AML. The 30-day induction death raye was 3% in the phase I/II study of VEN-HMA, and 6% in the phase I/II study of VEN-LDAC, which is remarkable for this patient population.6,10
Myelosuppression is the predominant toxicity encountered during venetoclax-based therapy, and this intensifies in severity and duration after several cycles of therapy. This situation is very relevant, because these regimens are given indefinitely as long as toxicities are manageable and there is no relapse.
One of the main concerns with the repeated occurrence of neutropenia is the risk of invasive fungal infections (IFIs) during AML therapy. Reassuringly, IFIs were reported infrequently during VEN treatment, notwithstanding the fact that broad-spectrum antifungal prophylaxis was not administered in the majority of treated patients because of the early concerns about drug–drug interactions. Phase I/II studies of VEN-HMA reported IFIs in the range of 8%. At COH, we analyzed the outcomes of 119 AML patients treated with VEN-HMA, and we reported an overall rate of 13% IFIs. As expected, IFIs were observed at a higher rate among non-responders compared to responders (22% versus 6%), and among patients treated with VEN-HMA in the r/r setting compared to newly diagnosed AML (19% versus 5%). 36
Given the concern of IFIs during neutropenic periods of VEN-HMA, one key question is the role of antifungal prophylaxis in this setting and the choice of agent. In our experience, we found that the use of antifungal prophylaxis was not consistent even within the same institution, as 21% of patients did not receive any, while 41% received azoles and 38% received echinocandins. We found no correlation between the use and the type of antifungal prophylaxis during VEN-HMA therapy and the risk of IFIs, and we concluded that the use of antifungal prophylaxis should be tailored towards the individual risk of IFIs during therapy, such as the AML setting (newly diagnosed versus r/r) among others. 36 In the phase I/II study of VEN-HMA, the low rate of IFIs was observed despite the prohibition of azoles, and only 46% of patients received echinocandins while the remainder did not receive any antifungal prophylaxis. 6
Tumor lysis syndrome (TLS) was found to be a serious side effect of venetoclax in Chronic lymphocytic leukemia (CLL). 8 Interestingly, clinical TLS was infrequently observed during AML treatment with venetoclax in combination with HMAs or LDAC.6,10 No clinical TLS was observed in phase I/II studies of VEN-HMA and VEN-LDAC; however, four cases of clinical TLS were reported in the phase III randomized study of VEN-LDAC. 13 Incorporation of a short, 3-day ramp-up of venetoclax dosing during the first cycle is still recommended, as was practised in the original studies. Furthermore, the pivotal studies required that the white blood cell count be lowered to <25 K/μL at the time of treatment initiation. Therefore, we recommend lowering the white blood cell count with cytoreduction prior to the initiation of a VEN-based combination, administering allopurinol and intravenous hydration, and closely monitoring TLS laboratory findings and manifestations.
Dosing of VEN, and managing dosing during prolonged use
No dose-limiting toxicities were observed for venetoclax during phase I studies when this agent was combined with HMAs and LDAC. Nonetheless, venetoclax at a daily dose of 400 mg and 600 mg was used in phase II/III efficacy studies when combined with HMAs or LDAC, respectively. These are the recommended doses of venetoclax when administered without the administration of concomitant moderate or strong CYP3A4 inhibitors. A ramp-up dosing is recommended in the first 3 days during the first cycle.
When combined with strong CYP3A4 inhibitors, such as posaconazole, the recommended venetoclax dose is 70 mg daily on the basis of pharmacokinetics data; 37 a dose of 100 mg is used when administered with other CYP3A4 inhibitors such as voriconazole. Comparative analysis showed no difference in efficacy when the dose of venetoclax was reduced because of concomitant CYP3A4 inhibitors. 38 For moderate CYP3A4 inhibitors such as isavuconazonium or fluconazole, the recommended dose is 200 mg daily.
As neutropenia is a predominant toxicity during venetoclax-based therapy in AML, treatment interruption and dose reduction may be required in subsequent cycles after patients have achieved complete remission. If the postinduction bone marrow blasts are >5% and absolute neutrophils count (ANC) is < 500 µ/L, we proceed with another cycle without interruption or venetoclax dose reduction. If the marrow blasts are <5% and ANC is < 500 µ/L, we delay cycle 2 up to 28 days until ANC recovery. If ANC requires more than 14 days to recover, then we shorten the venetoclax schedule to 21 rather 28 days on the subsequent cycle. If the postinduction marrow blasts are <5% and ANC is >500 µ/L, we proceed with the second cycle. A further reduction in venetoclax duration (i.e. 14 days) may be needed in subsequent cycles in patients with delayed count recovery, and in some cases, HMA dose reduction is required to improve prolonged cytopenias.
In patients who achieve remission with VEN-based therapy, we frequently administer granulocyte colony stimulating factors (G-CSFs) such as filgrastim to shorten periods of neutropenia to reduce the risk of infectious complications.
Duration of venetoclax-based therapy and alloHCT after VEN-HMA
Original studies of VEN-based therapies were designed for the combination to be given indefinitely in the absence of relapse or significant toxicities. In the phase II VEN-HMA studies, at the time of report, the median number of VEN-HMA cycles was five, but there were patients who received up to 25 cycles. 6 Some of the original patients on the study treated at COH remained on the combination long term, and one of our patients is currently receiving cycle number 39 as of the time of writing.
It is generally observed that the ability to deliver full doses on schedule becomes limited with prolonged administration of VEN-based regimens, and this circumstance often leads to lowering drug (HMA or LDAC) doses and prolonged durations of breaks between cycles.
Although preclinical studies support the potential of VEN-HMA in eradicating LSCs, 31 the majority of patients eventually relapse, especially if therapy is maintained. However, it is unknown how long to administer a VEN-based combination before the patient is deemed cured, if this is achievable at all in a subset of patients.
Our recommendations for newly diagnosed AML patients who achieve remission with VEN-HMA is to undergo alloHCT if they become fit after complete remission is achieved and a donor is identified. This approach is particularly critical in patients with high-risk genetics, those with persistent MRD after several cycles, and r/r patients, in whom durable remission is unlikely to be attained with just VEN-based therapy and relapse is imminent after the achievement of CR thereby providing only a short window of opportunity for potentially curative alloHCT. Reduced-intensity and non-myeloablative conditioning-based transplantations are well tolerated in elderly patients, and the graft versus leukemia effect may lead to eradicating residual leukemia and possibly cure.
Of 32 patients with newly diagnosed and r/r AML who underwent alloHCT post VEN-HMA at COH, the majority were in remission (69%) and received reduced-intensity conditioning. One-year OS, disease-free survival, non-relapse mortality, relapse rate and grade II–IV acute graft versus host disease were 63%, 44%, 19%, 38%, and 44%, respectively. However, the one-year OS and relapse rate for patients who underwent alloHCT in remission were 77% and 9%, respectively. 39 A similar experience was reported by Pratz and colleagues in 31 patients with AML who underwent alloHCT after a VEN-based combination, including 16 in CR/CRi. 40 The 1-year OS was 68%, and 55% remained in remission. 40
However, for patients ineligible for alloHCT consolidation, we recommend the continuation of the VEN-based combination therapy as long as the patient is tolerating treatment and deriving clinical benefit. After patients attain remission with VEN-based therapy, we periodically monitor the ongoing response using bone marrow biopsies performed every 3–6 months, and we routinely test for MRD to identify early relapse. Patients relapsing after VEN-based therapy have a poor prognosis, as demonstrated by Maiti et al., 41 and such patients should be referred for clinical trials.
Future directions
The marked activity and favorable safety profile of venetoclax-based combinations in AML led to extending its investigation in a number of innovative combination studies, many involving combinations with novel agents in order to improve the results observed with the initially tested combinations further.
The response rate of VEN-HMA in unfit patients with untreated AML harboring non-favorable risk genetics is approaching what is observed with standard induction regimens; nonetheless, the safety profile is likely to be more favorable with VEN-HMA compared to 7+3 or equivalent regimens. This has led to investigating VEN-HMA as an induction regimen in younger and fit patients (>40 years) with newly diagnosed, non-favorable risk AML in a phase II multicenter randomized study. In that study (multicenter study including Massachusetts General Hospital, COH, and others), the efficacy of VEN-HMA will be compared to 7+3 or liposomal daunorubicin and cytarabine regimens in untreated AML (approved study in final stages of development). Another randomized study in development will compare venetoclax and Astx727 (oral azacitidine) combination with 7+3 in fit adults (>18 years) with adverse risk AML. Furthermore, a single-arm study at the University of Colorado is actively investigating the VEN-HMA regimen in untreated AML with adverse risk genetics, including younger fit adults [ClinicalTrials.gov identifier: NCT03573024]. Venetoclax is also being tested in the frontline setting with reduced and standard doses of CPX-351 in elderly and fit patients with AML, respectively [ClinicalTrials.gov identifiers: NCT04075747; NCT04038437], as mentioned previously.
As recurrent driver mutations are common in AML, and recently approved targeted agents have shown promise in these subtypes of leukemia, venetoclax is being actively investigated in combination with novel targeted agents in AML. For example, venetoclax is being studied with targeted agents in genetic subtypes such as FLT3 inhibitors [ClinicalTrials.gov identifiers: NCT04140487, NCT03625505, NCT03661307] in newly diagnosed and r/r AML with FLT3m, in combination with the TP53 activator APR-246 [ClinicalTrials.gov identifier: NCT04214860] in AML with TP53m, and with ivosidenib or enasidenib [ClinicalTrials.gov identifier: NCT03471260] in IDH1m or IDH2m AML, respectively. Interim analyses of ongoing prospective studies have shown the feasibility and promising activity of venetoclax in combination with the FLT3 inhibitors enasidenib or ivosidenib with or without HMAs in AML in patients with recurrent genetic alterations.14,21 A preclinical study has shown that venetoclax has synergistic anti-leukemia activity in combination with a BET inhibitor, 42 and a phase I study was completed showing safety and activity. The upregulation of MCL1 is an observed resistance mechanism to BCL2 inhibitors,5,43,44 and therefore venetoclax is being tested in combination with MCL1 inhibitors [ClinicalTrials.gov identifiers: NCT03797261, NCT03218683]. Venetoclax is also being studied in combination with CD123-targeted therapies such as SL-401 and IMGN632 [ClinicalTrials.gov identifiers: NCT03113643, NCT04086264]. VEN-HMA is planned to be investigated as maintenance therapy in high-risk AML patients undergoing allogeneic HCT, with an attempt to reduce disease recurrence post-transplantation.
Footnotes
Acknowledgements
The authors acknowledge James Sanchez for editorial support.
Conflict of interest
I.A. serves on an advisory board and receives research support from Abbvie. V.P. serves on an advisory board and is a consultant for Abbvie. A.S. receives research support from Abbvie.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.