
Abstract
With survival expectation that of age-matched controls and given excellent response and worldwide access to tyrosine kinase inhibitors (TKI), family planning is increasingly important for a considerable fraction of patients with chronic myeloid leukemia (CML). The potential for therapy discontinuation (“treatment free remission”) can afford the opportunity for a CML patient in deep response to plan and carry a pregnancy to full term without any therapeutic interventions. However, the reality of pregnancy desired or occurring when patients are not eligible for treatment-free remission raises the discussion of therapy choices during pregnancy. To date there are no official guidelines available to assist patients and clinicians with these decisions. This first position paper aims to analyze information published and presented surrounding this challenging area, with focus on different scenarios of disease burden and time from CML diagnosis, including CML discovered during pregnancy and pregnancy during CML treatment. An updated review, supported by data and presented together with authors’ joint recommendations, is aimed to counsel the practical management of CML patients and pregnancy.
Introduction
In the current era, a diagnosis of chronic myeloid leukemia (CML) and pregnancy should not be mutually exclusive. CML survival has vastly improved and approaches that of non-leukemia age-matched controls. Worldwide, the age at diagnosis varies from the “adult-advanced” age of 55–65 years in industrialized countries to a median 10–15 years younger, notably in developing countries with the greatest population growth. 1 Thus, with a substantial CML population of reproductive age worldwide, the possibility of pregnancy and the need to manage pregnancy are increasingly important. With the ability and knowledge to utilize both old and new treatment options such as interferon (IFN) and tyrosine kinase inhibitors (TKIs) and increasing confidence in “treatment free remission” (TFR)—a planned therapy discontinuation—it is possible for physicians and patients to design and orchestrate a successful approach to pregnancy.
There are currently, however, no established guidelines for pregnancy in CML; expert recommendations have been published 2 and recently updated.3–5
Fertility and pregnancy issues should ideally be discussed at diagnosis. Counseling about the possible risk and benefit of stopping or delaying treatment to conceive, where appropriate, should be given to the patient and partner. Specific to male patients, TKIs have little effect on fertility and progeny with the caveat that little is known about more recently available (ponatinib) and novel (asciminib) agents. Therefore, for men, first- and second-generation drugs do not need to be discontinued if pregnancy is planned. Specific to women, TKIs are teratogenic and use should be limited or excluded during pregnancy, especially during the early period of organogenesis (5–13 weeks of pregnancy). 6 Conception in female patients with continuous active treatment is questioned and strongly discouraged due to the risk of fetal abnormalities. 7 Depending on individual circumstances, ovarian, oocyte or embryo cryopreservation can be considered and requires active collaboration between obstetricians and hematologists. 8
Given this framework, how can we start to ‘plan’ a pregnancy given that TKI during pregnancy is contraindicated? The first thing to consider, if the patient is already on treatment, is response to therapy. CML response landmarks are well defined (Table 1) and include established milestones: complete hematologic response (CHR), complete cytogenetic response (CCyR), major molecular response (MMR; or MR3), and deep molecular response (DMR; MR4 or better). At present many consider, irrespective of pregnancy considerations, that TFR is the goal of therapy and operates on the principle that planned cessation of TKIs can be suggested and planned “safely” in patients with at least 1–2 years of DMR. Many TFR studies have proved that, independently of TKI used, 40–50% of such patients can remain free of treatment with ongoing follow-up, while the remaining 50–60% will lose MMR within 12 months and require re-treatment. 9 MMR is considered a “safe haven” and thus the recommendation is to resume treatment if MMR is lost, maximizing likelihood of regaining response and minimizing any risk of disease progression.
Criteria of hematologic, cytogenetic, and molecular responses in chronic myeloid leukemia.

PCR, polymerase chain reaction.
When a female patient satisfies guideline-derived (NCCN, ESMO) “eligibility criteria” for TKI discontinuation and wishes to become pregnant, it is entirely reasonable to follow the standard practice for TFR.10,11 However, not all pregnancies are planned, not all patients are eligible for safe discontinuation, and MMR may not be sustained throughout conception attempts and/or pregnancy, necessitating contingency planning and guidance. Possible scenarios suggesting the need for management plans include:
CML diagnosed during pregnancy;
Pregnancy during CML treatment, specifically:
(a) Pregnancy early in CML treatment;
(b) Pregnancy late in CML treatment and not TFR candidate;
(c) Pregnancy late in CML treatment and TFR candidate.
CML diagnosed during pregnancy
CML may be diagnosed at any time during gestation and raises issues relating to: (1) consideration of termination; (2) timing of therapy initiation; and (3) the choice of therapy during pregnancy, considering the balance of safety and efficacy versus risks to both mother and child.
In most patients CML is diagnosed in chronic phase (CP). Initial blood counts may vary from a moderate increase in leukocyte count to marked hyperleukocytosis coupled with thrombocytosis. Due to lack of evidence, it is difficult to predict whether a delay in TKI initiation might impact prognosis or permit disease progression; offsetting this concern is the fact that CML at onset is characterized by 2–3 years of CP before evolving if untreated 12 and many patients present with symptoms and blood count changes of several months’ duration. Persistence of abnormally high blood counts increases the chance of obstetric complications including thrombosis, bleeding, placental insufficiency, and intrauterine growth retardation; in order to diminish these possibilities it becomes reasonable to pursue cytoreduction during pregnancy to benefit both mother and child.
Historically, the treatment options in CML diagnosed during pregnancy included leukapheresis and IFN. However, leukapheresis is a temporizing procedure with no curative potential or lasting effect, and availability of this procedure is limited. IFN is generally considered safe for the fetus, with minor concern over the vehicle polyethylene glycol (PEG) present in long acting interferons, which in practice has shown no harmful impact, possibly due to limited exposure to small amounts of PEG. IFN has a slower and less certain ability compared with TKI to induce control of abnormal blood counts and therefore may not be a sufficient treatment for high leukemic burden at CML onset.
Hydroxycarbamide (HC) may provide a rapid cytoreduction but its use during pregnancy is restricted due to recognized teratogenicity in preclinical studies. There are a limited number of case reports describing the use of HC in pregnancy without harmful effects but the data are insufficient to recommend its general use.13–15
Potential teratogenicity of TKI is clearly a matter of concern, and conclusions regarding the balance of risk and benefit for every TKI are different. As reported by Pye et al. congenital abnormalities on imatinib were mostly observed when it was used during organonenesis. 7 No preclinical teratogenicity and no increased rate of birth abnormalities have been described in the full prescribing information for nilotinib. In contrast, dasatinib has been noted to be harmful to the fetus in both early (first) and late (second/third trimester) gestation. 16 Knowledge about the limited placental transfer of imatinib and nilotinib17–19 and emerging data from observational multicenter CML registries 20 reporting uneventful use of these drugs late in pregnancy may warrant their cautious introduction after placental formation (15th–16th week) if treatment is needed urgently. However, dasatinib cannot be recommended for use at any time during pregnancy even after placental formation, based on available data and knowledge that it passes through placenta. A recent report of 16 cases from Pfizer’s bosutinib safety database of women receiving bosutinib and pregnancy noted six live births, three abortions (two by choice and one for a molar degeneration), one miscarriage, unrelated to bosutinib, and six outcomes unknown. The mothers had all stopped taking bosutinib, two at 5 weeks of pregnancy and the other at unknown time. The babies were reported healthy at birth. 21 The paucity of information regarding bosutinib as well as ponatinb and emerging novel agents such as asciminib discourages their use even after placental and organ formation.
According to recent data from the ELN CML Pregnancy Registry, 21% of cases were diagnosed during pregnancy; 22 about 70 cases of CML diagnosed during pregnancy in the TKI era have been reported to date. Delivery of normal healthy children has been reported in several case series incorporating different treatment strategies. Data from MD Anderson Center (USA) were presented at the American Society of Hematology 2017 meeting; 23 reported outcomes of 13 patients with CML onset during pregnancy were as follows: healthy deliveries (n = 12, including two twins), spontaneous miscarriages (n = 2; at weeks 4 and 27 of gestation), and one elective abortion. TKI therapy was postponed in all patients until after the end of the pregnancy. One patient received IFN, one patient underwent leukapheresis, and five patients received short courses of HC. Second generation TKIs (nilotinib, dasatinib, or bosutinib) and imatinib were started after delivery in 11 and two patients, respectively. MMR and DMR were achieved in seven and five patients respectively (3–68 months); one patient had a progression from CP to blast crisis (BC).
The experience of the Hammersmith Hospital (London, UK) for CML diagnosed at pregnancy in the TKI era included eight cases: seven pregnancies resulted in childbirth with one spontaneous abortion (unpublished data). Three patients received IFN during pregnancy, while four patients had no drug therapy until delivery. Four patients underwent leukapheresis, repeated from two to 17 times. Five patients received imatinib and two patients were given second generation TKIs after childbirth. Two patients had resistance to first line TKI and were switched to alternative TKIs. All patients were alive with the median follow-up of 58 (14–195) months; one patient had achieved MMR and the remaining seven achieved MR4–MR5 at the time of reporting. Two cases of CML diagnosed during pregnancy came from the Lyon Hospital, France. 24 Both pregnancies ended in normal childbirth. Both patients received IFN and one HC during pregnancy. Imatinib and nilotinib were started after delivery and optimal disease response was achieved.
Additional reports in the literature highlight management challenges. A case of CML diagnosis during pregnancy was reported 25 with 20 leukapheresis procedures performed and ultimately premature labor induction. An optimal treatment response was achieved one year post-partum on TKI therapy. In another case CML in pregnancy with hyperleukocytosis was treated with IFN only until delivery; 26 initial CP progressed to BC with 32% peripheral blood blasts shortly after labor. The woman was not able to achieve a response after 9 months of therapy (details not provided) and was referred to hospice care. The child had respiratory distress at birth, but further development was reported normal.
Incomplete or insufficient management of blood counts with IFN or leukapheresis likely drives physician consideration of imatinib in patients diagnosed during pregnancy. Several case reports have described effectiveness and safety using imatinib in late pregnancy. Ali et al. reported the use of imatinib from the 21st week of gestation until delivery in a woman diagnosed with CML during the second trimester 27 resulting in a normal childbirth without congenital defects or side effects. Limited imatinib placental transfer was demonstrated. The authors summarized information from 26 cases of imatinib use during pregnancy and noted no fetal abnormalities when the drug was started beyond the second trimester. A subsequent report by Burwick et al. 28 described the use of imatinib at 28 weeks’ gestation for CML diagnosis in pregnancy, after failure of leukapheresis and IFN; complete hematologic response was achieved within 4 weeks. Normal childbirth was observed despite detection of residual levels of imatinib in placental tissue and amniotic fluid. Yadav et al. reported a case of imatinib and HC use for CML diagnosed in the third trimester; imatinib was introduced at 32 weeks, with delivery at week 37; no subsequent follow-up was reported. 29
The outcome and therapy of 48 patients from six countries with CML diagnosed at pregnancy were summarized and presented at the 2018 meeting of the American Society of Hematology. 30 The majority of patients (70%; 33 patients) delivered children, 14 patients had elective abortions, and one had a spontaneous abortion. Imatinib was used in 13 patients in either the second or third trimester. Other therapy included IFN (five patients) and HC (one patient) while 14 patients were observed without therapy until delivery. Pregnancy outcome was unremarkable (no fetal abnormalities). Imatinib and second generation TKI (dasatinib and nilotinib) were introduced in 30 and three patients, respectively, after delivery; 23 (67%) patients achieved optimal treatment response. One patient received IFN for 4.5 months during pregnancy and imatinib after week 31 for CHR lost. She regained CHR, delivered a healthy child at term but 2 months after progressed to BC and died after subsequent failure of allogeneic stem cell transplant.
In summary, delivery of normal healthy children with different treatment strategies has been reported in several case series of CML diagnosed during pregnancy. In general, adverse impact of treatment delay after CML diagnosis in pregnant women is uncertain. However, the two reported cases of disease progression to BC in women for whom TKI administration was postponed are disturbing. Although both cases deal with the progression to BC after labor, and detailed information concerning the biological presentation or progression of the CML is lacking, they highlight the issue of starting treatment with TKI as a more effective therapy option.
Recommendations for CML diagnosed during pregnancy
Given the variety of different scenarios, weighting treatment start or delay depends on initial blood counts and expected time to labor. As the chance of progression without TKI treatment should be taken into consideration, most cases may warrant therapy when CML is diagnosed at early pregnancy with delivery expected after several months. The control of white blood cell and platelet counts are also important to avoid obstetric and delivery complications.
Overall, for CML diagnosed during pregnancy, such decisions, including choosing termination or continuation of pregnancy, should be judged individually.
The nature of the treatment used should take into consideration the gestational stage. For patients in the first trimester, ideally all cytoreductive medication should be avoided, and a treatment-free first trimester would be ideal. If the white cell count is >100 × 109/L, leukapheresis may be useful to immediately reduce the white cell count and allow the pregnancy to proceed without other intervention. It is not effective in inducing sustained reductions in the platelet count; aspirin or low molecular weight heparin may be necessary if the platelet count is very high, for instance >600 × 109/L. Interferon can be used, but may provide a slow kinetic of tumor burden reduction.
For patients presenting in the second and third trimesters, the advice is similar although the risk of congenital abnormalities is much lower since organogenesis is well established. Treatment may not be necessary if the counts remain low. There is rarely an indication for HC and, if used, it should only be given for a short period of time to reduce leukocyte or platelet counts. IFN can be used safely. In theory imatinib can be introduced after 15 weeks (point of placental maturation and critical organ formation) because of limited placental transfer but is not recommended by the manufacturer. Although nilotinib can be considered, second generation TKIs should be avoided until after delivery. Care should be taken not to induce cytopenias, particularly around the time of delivery.
For patients presenting in accelerated phase (AP) or BC, the risk to the mother in delaying treatment is higher. Consideration must be given to terminating the pregnancy, especially if advanced phase CML is diagnosed in the first trimester, and immediate treatment is warranted. Imatinib or second generation TKI can be used in AP after pregnancy termination; acute leukemia like chemotherapy with or without TKI should be used in BC; steroid/TKI combinations may be feasible and safer in lymphoid BC. There may be rare exceptions of advanced disease presenting in later stages of pregnancy where it may be possible to deliver the baby earlier. Sensitive and compassionate counseling of the parents, and careful examination of all possibilities, is mandatory.
Careful follow-up of the patients during pregnancy is needed. Regular complete blood counts (CBCs) can be performed every 7–14 days. If a complete hematologic response is achieved, CBC can be evaluated less often until closer to delivery. In cases where a TKI is administered, response expectations should mirror those in the non-pregnant state (molecular response evaluation after 3 and 6 months recommended). Optimal obstetrical follow-up and monitoring is necessary, and maximal use of available prenatal testing is recommended. Delivery timing and method may be defined considering both the obstetric and hematologic status. After delivery the patients should be treated according to the established guidelines with timely switch of TKI in cases of treatment failure or intolerance.
Pregnancy during CML treatment
If pregnancy is suspected or confirmed a female CML patient should interrupt TKI treatment.
Given that time from diagnosis, treatment initiation and depth of molecular response are key factors, management of pregnancy occurring during CML treatment could be divided into three circumstances: (1) pregnancy early in CML treatment; (2) pregnancy late in CML treatment, not TFR eligible; and (3) pregnancy late in CML treatment, TFR eligible. Interesting, published case reports do not always distinguish between early and late CML treatment.
Clinical data in non-pregnant CML confirm that TKI treatment duration may influence TFR rate.31,32 It is conceivable that late into CML treatment, in DMR, where biologic sensitivity to TKIs is clear, such patients are candidates for TFR independent from pregnancy and quite naturally the agendas of TFR and pregnancy intersect. ‘TFR eligibility’ of a pregnancy case thus can serve as a good framework for advice, risk assessment and risk management.
In contrast, patients in stable MMR, not DMR, have less chance to maintain the achieved molecular response when therapy is discontinued. However, based on our experience and that of others, women with optimal treatment response who are in an MMR sustained for >12 months have demonstrated ability to safely stop their TKI without pregnancy complications related to their underlying CML. The resumption of TKI treatment in compliant patients resulted in restoration of excellent disease control, with no post-partum progression to advanced phase as detailed later.
Lasica et al. described 12 patients with ⩾MMR response (but not TFR candidates), in whom TKI was replaced with IFN during pregnancy. All patients retained or re-established MMR or better with subsequent resumption of TKI therapy. 33 In another report from the American Society of Hematology 2018 meeting, 34 representing data from five clinics, it was shown that loss of initial MMR when TKI was interrupted for pregnancy was reversible, and that MMR could be recovered within 1–2 years after TKI restart despite additional loss of cytogenetic response or MR2. A recent study by Dou et al. showed that MMR duration ⩾3.5 years was significantly associated with MMR-failure-free survival during pregnancy. 35 Thus, similar to TKI cessation predictors in the non-pregnant state, initial TKI sensitivity, time on therapy and longer MMR duration are relevant determinants of safe TKI interruption for pregnancy.
Pregnancy early in CML treatment (<3 years of TKI therapy)
Although not optimal, it is possible that a patient less than 3 years on TKI therapy, who is less likely to have achieved a sustained MMR or deeper response, will either become or wish to become pregnant. In such cases the residual leukemia burden and the response to therapy to date should be taken into careful consideration. For a patient with a high residual leukemia burden (⩽MR2) resulting from either short (<3–6 months) TKI exposure or longer exposure and suboptimal response to therapy, we suggest managing such cases akin to CML diagnosed during pregnancy.
TKI therapy should be stopped promptly when pregnancy is discovered, during the first trimester based on fetal risk. After an individual discussion, if pregnancy is continued, hematologic or cytogenetic relapse may be expected and primary consideration should be given to IFN in order to control the disease without jeopardizing organ development in the fetus.36,37 After placental formation and crucial fetal organ development are complete (15–16 weeks), consideration can be given to introduction or re-introduction of select TKI therapy (imatinib or nilotinib) where indicated and after clear discussion regarding risk/benefit and some degree of uncertainty, highlighting that TKIs are contraindicated by labeling and health authority precaution during pregnancy. Dasatinib should not be used at any time during pregnancy. In the largest series of dasatinib-treated pregnancy cases reported by Cortes et al., of three women treated with dasatinib during pregnancy, only one delivered a normal infant (dasatinib initiated at week 17). Both remaining fetuses developed hydrops fetalis, one terminated at week 17 (treated during weeks 6–17), the other delivered prematurely at week 28 (treated week 17–24) and survived <24 h. 16
Patients in MMR at time of pregnancy with a short exposure to TKI or those with less than deep molecular response despite longer time on therapy present a substantial risk of loss of molecular response. Similar to the aforementioned suggestions, interferon can be added in such cases, or imatinib or nilotinib can be considered if BCR-ABL transcript level rises above 1–10% after 15–16 weeks.
Pregnancy late in CML treatment (>3 years of TKI therapy), not TFR candidate
Patients with more than 3 years of therapy may also present with differing scenarios, ranging from the ‘ideal candidate’ to plan and carry a pregnancy, or perhaps not the ‘worst candidate’, but notably unable to achieve DMR despite prolonged TKI exposure. The latter cases may be somewhat indolent clinically on therapy but with interruption may face loss of molecular, cytogenetic or hematologic remission. Suggestions for these patients in principle are similar to those stated previously: in cases of unplanned pregnancy, the TKI should be stopped as soon as the pregnancy is suspected; consideration should be given to replacing TKI with IFN, and additional consideration for use of imatinib or nilotinib in the later stages of pregnancy, if necessary, where it is agreed that risk is acceptable. In the case of a patient who has failed to achieve sustained MMR or deeper response, but wishes to become pregnant, consideration can be given to changing the TKI to try to obtain deeper response and defer immediate pregnancy planning until a later date. Interventions such as embryo or oocyte cryopreservation may be suggested or indicated if there is concern regarding older age and loss of fertility while trying to establish a deeper response.
For patients in sustained MMR but not in DMR it is not unreasonable to stop treatment to attempt conception. The time for natural conception after stopping treatment varies, depending on age (with advanced age reducing the probability of conception), between 2 and 56 weeks, as reported by Lasica et al., 33 or conventionally at ~15 weeks for the non-CML population. Thus those 3–4 months needed for conception should be added to the first trimester time period, bringing the time advised to be ‘treatment free’ surrounding pregnancy initiation to an average of 6 months. Based on highly variable lead-in time required to avoid treatment, the alternative to stopping for conception is the strategy of stopping treatment at first positive pregnancy test (typically 4–5 weeks), at implant, before organogenesis. Such a strategy requires a well-informed patient, knowledge of menstrual cycle patterns and indicators of ovulation/fertility as well as ready access to sensitive pregnancy testing. According to present data of the GIMEMA and the ELN database, such an approach seems rather safe as about 70% of all successful childbirth cases described in those registries occurred in women who stopped treatment immediately after pregnancy confirmation and no abnormalities were observed in the offspring.
Patients who have been in DMR (MR4 or better) for >12–24 months can be managed exactly as a patient eligible for a trial of discontinuation and TFR. The recently suggested criteria for safe TKI discontinuation and observation in TFR include TKI duration for >3–4 years for second generation TKIs or >5 years for imatinib; the recommended DMR duration is at least 1–2 years.5,32 These patients have a ~50% chance of being able to remain off drug indefinitely. However, another 50% could lose response, the majority within 3–6 months, 38 and thus potentially before the end of first trimester, warranting caution when stopping treatment prior to conception. Stop at first positive pregnancy test, as above, can be considered. Lastly, consideration of sequential TFR attempt without pregnancy, at least past 6 months where relapse risk is greatest, followed by conception attempt, may offer lower risk of molecular relapse during pregnancy when treatment options are more limited.
For those patients who experience molecular relapse (MMR loss) when trying to conceive but are not yet pregnant, treatment should be re-started. If a sustained DMR is re-established, subsequent conception attempts and stop at first positive pregnancy test during continuous TKI treatment can be suggested to minimize the need to retreat in the first trimester.
For pregnant patients in molecular relapse, management will depend on their clinical situation. Observation of relapse kinetics during pregnancy may suggest that patients who have had very deep response prior to conception may be less likely to experience rapid increases in their leukemic burden and thus may be able to defer treatment until after delivery. If they do experience loss of CCyR or CHR, they can be managed as the aforementioned pregnant CML patient.
The largest databases of CML outcome after TKI interruption in pregnancies are those of GIMEMA and the ELN and were presented at ASH 201820 and EHA 2019. 22 In the GIMEMA database, retrospective and prospective data of conception and pregnancies in male and female CML patients from Italian centers were collected; 56 female pregnancies with an established CML diagnosis under treatment were described. Of those with known molecular status at pregnancy onset, 27 were in DMR; 19 (70%) delivered without need for therapy, achieving a treatment free pregnancy (TFP ) status. Eleven were in MMR, with five (45%) TFP, while eight patients with high tumor burden (⩽MR2 at time of pregnancy) all required therapy during pregnancy. Treatment generally resumed with loss of MMR or CCyR; none of the patients lost CHR. All patients stopped TKI treatment when pregnancy was discovered (3–6 weeks’ gestation). Treatment information is available for 14 patients; 10 patients received IFN; TKIs were reintroduced in four patients, two with imatinib, and two nilotinib, after placental maturation (>20 weeks). No complications were noted in either the mothers or the developing children; post-natal follow-up noted normal child development and growth.
Interestingly, the kinetics of transcript rise was studied in 29 patients, and BCR-ABL doubling time (DT) during TKI cessation for pregnancy exhibited a bimodal trend, very short for some patients (mean 5.8 days) and much longer for others (mean 182 days), and did not seem to correlate with molecular status pre-cessation. These data are based on small numbers, but suggest a higher than expected rate of MMR retention and response stability, suggesting that kinetics of regrowth of residual CML during pregnancy in female patients may be different from that observed in non-pregnant TFR patients.
Similar results were found by Lee et al. (ASH 2018) with 19 patients starting pregnancy in MMR, subsequently lost in 12 (68%), but for 28 in ⩾MR4 markedly less loss of MMR (39%, 11 cases) was noted. BCR-ABL DT was also variable, with ~50% of cases demonstrating longer DT than non-pregnant TFR patients. Specifically, a significant portion (43%) of patients with loss of MMR during pregnancy TKI cessation retained MR2 (~CCyR) until delivery, with median time from MMR loss to delivery of 5.0 months, allowing such cases to deliver without therapy (TFP). 39
The ELN database is the largest archive of pregnancies in female CML patients established to date. It includes retrospective and prospective data from 13 countries with information on 305 pregnancies. In 249 of 305 cases, molecular response evaluations at start of pregnancy have been recorded. Eighty (32%) patients were in DMR and 31 (12%) in MMR; higher tumor burden was present in others with 32 (13%) in MR2 and 106 (43%) with BCR-ABL >1% international scale (IS). One hundred and eighty-two patients conceived while on TKI (71%, considering 257 pregnancies for which data are available). These included 141 (77%) patients treated with imatinib and 41 (23%) who received second or third generation TKIs. TKIs were usually stopped early in the first trimester when pregnancy was discovered (4th–5th week of gestation). In 82 pregnancies, patients were subsequently treated during the 2nd–3rd trimester, after placental formation. Treatment included imatinib in 33 (40%) of cases, nilotinib in seven (9%), IFN in 24 (28%), HC in six (7%) and in one case, pegylated IFN. Five of seven nilotinib treated patients received reduced dosage (400 mg daily), deemed sufficient to control the CML and preserve the complete hematologic remission. Imatinib was used throughout pregnancy in 13 (16%) cases. Congenital abnormalities were recorded in four (1.7%) cases as follows: polydactyly (1), hypospadias (1), and non-closed foramen ovale of interatrial septum (2). None of the abnormalities were severe or life threatening and their relationship to TKI use was deemed unrelated by physicians. Low birth weight was recorded in 13 children with imatinib or nilotinib exposure in late pregnancy. Regular follow-up of all children was recorded with a median age at follow-up of 5 years (range 2 months–17 years). The first analysis from this database focused on highlighting the feasibility and the “safety” for children. Information regarding CML status at delivery or after delivery was not noted, though the importance of adherence to treatment and strict follow-up was stressed in order to avoid progression of disease.
Pregnancy late in CML treatment (>3 years of TKI therapy) and TFR candidate
A patient planning a pregnancy or who conceives during CML therapy who has achieved and maintained a DMR is, by CML treatment guidelines and CML pregnancy recommendations, the best suited candidate for therapy interruption. At present it is not possible to precisely predict relapse amongst eligible TFR candidates; and approximately 40–60% of patients stopping TKIs will lose MMR and require retreatment, with >80% of molecular relapses occurring in the first 3–6 months. 38 Those patients who retained a DMR or have no MMR loss after the childbirth can continue treatment-free observation with appropriate molecular follow-up and expectation of retreatment in the case of potential late MMR loss, as recommended. 5
Even in this lower risk situation, extensive counseling and careful and personalized follow-up of patients during pregnancy is needed. Molecular testing should reflect the kinetics of BCR-ABL rise, following current TFR (i.e. monthly) guidelines and potentially more frequent for patients with higher transcript levels over time. Teamed obstetrical and hematological follow-up is advised as in other scenarios.
Recommendations for pregnancy including breastfeeding in CML
As in the non-pregnant state and central to management, time from diagnosis and tumor burden can guide management and may predict outcome in pregnancy during CML. High tumor burden patients (⩽MR2) should be managed akin to new/recent CML diagnosis cases, may range from early to late (>3 years) into treatment, and IFN and appropriately timed TKI therapy is suggested. Patients with MMR, also potentially early or late after diagnosis and treatment initiation, are at higher risk of MMR loss during pregnancy TKI cessation, and IFN can replace TKI to maintain response. Kinetics of BCR-ABL rise should be considered as plateau and markedly slower relapse have been observed during pregnancy. Patients in DMR early in CML treatment (<3 years), based on favorable response, may stop TKI and adopt a “watch and wait” approach. Patients in DMR late into CML therapy (>3 years), typically candidates for non-pregnancy TFR, may pursue TKI stop for pregnancy including conception, often merging conventional TFR monitoring with the goal of achieving and carrying a pregnancy to term. Under the best circumstance (40–60% of those meeting criteria of TFR success), TFP success may follow.
An additional important consideration is breastfeeding. When possible for immunologic benefit to the newborn, colostrum and short-term breastfeeding can be offered even in women who need to restart TKI treatment. A woman with successful TFP can breastfeed the baby as long as response is maintained. A slower rise of BCR-ABL transcript and preserved response, such as fluctuations between MR2–MR3, may facilitate prolonged breastfeeding if consensus is not to mandate rush to restart TKI therapy. For women who are treated with IFN, lack of neonatal assimilation orally via breastmilk may obviate concern if a period of breastfeeding is desired and feasible prior to TKI restart. For women who restarted or who restart TKI, imatinib and nilotinib are demonstrated not to reach therapeutic concentrations in an infant’s blood during breastfeeding by a mother on these agents.40,41 However, lack of clinical evidence of use in children under one year of age and the excellent alternative of bottle feeding supports this strategy while a woman is receiving any TKI.
Conclusion
Planned and unplanned pregnancies coinciding with CML can indeed be managed. Strict collaboration between the key disciplines—hematologist, obstetrician-gynecologist, neonatologist, and others—is crucial. Also paramount is that the patient and those supporting them (partner, spouse, family, etc.) should be properly educated and aware of the pros and potential cons, risks involved, and contingency plans discussed. Stated simply, three factors must always be considered: the mother, the baby, the illness; all equally important and related. A summary of recommendations is presented in Table 2.
Therapy management during pregnancy in chronic myeloid leukemia patients, considering time from TKI therapy and tumor burden.
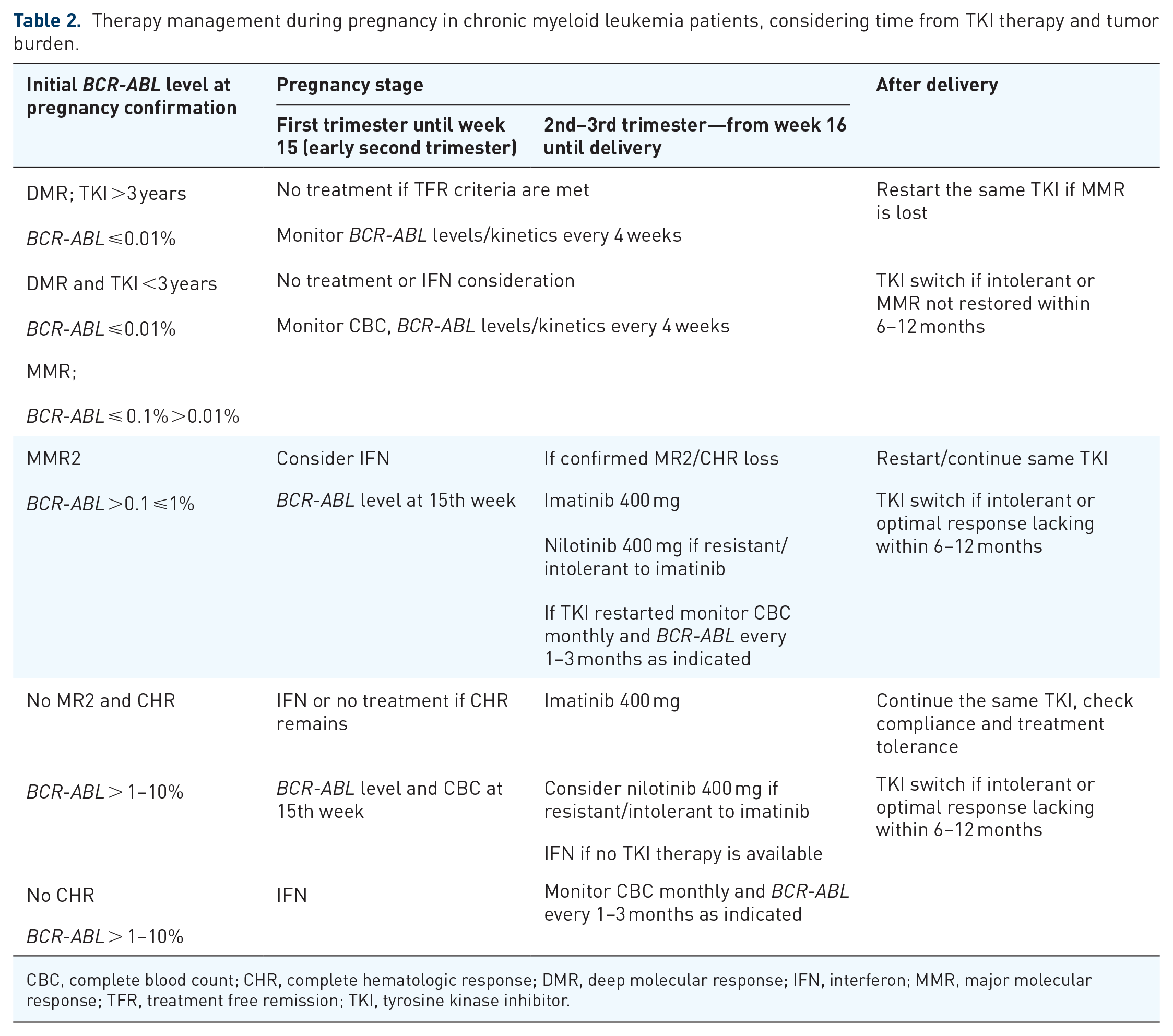
CBC, complete blood count; CHR, complete hematologic response; DMR, deep molecular response; IFN, interferon; MMR, major molecular response; TFR, treatment free remission; TKI, tyrosine kinase inhibitor.
It should be understood that CML patients should be encouraged to pursue a “normal life”, including planning a family, given advances in treatment and understanding of the natural history of CML in the era of TKI therapy. 42 Increasing numbers of pregnancy cases, as shown in Figure 1, are reported to result in normal childbirth. Despite the overarching principle of halting and avoiding TKIs during pregnancy, selected TKIs, specifically imatinib and nilotinib (given minimal placental transfer), may be started after organogenesis. Additional considerations, such as a reduced dosage of nilotinib, can be considered. Broadly applicable, the most recent update of 224 cases of pregnancy in female patients with CML within the ELN database 43 confirmed that based on the different situations examined, treatment with IFN is confirmed safe. If therapy during pregnancy is deemed necessary, IFN can be used at any time; if introduced earlier, IFN can offer greater chance of preserving molecular response after TKI interruption, whereas TKIs use can reduce high tumor burden.

Cumulative number of pregnancy outcomes in a National Research Center for Hematology, Moscow, Russia, from 2000 to 2019.
Caution should be taken when considering TKI cessation for the purpose of conception; this approach includes uncertainty regarding time needed for successful conception, and thus greater possibility of losing response; early stop (at first confirmation of pregnancy, or high suspicion) may be an overall safer approach. In synthesizing available knowledge regarding risks of TKI use during pregnancy with clearer understanding of TFR, it should be concluded that a planned pregnancy in stable DMR is the optimal intersection of minimal risk for triad of mother, baby, and CML.
We hope that these data and evidence presented may stand as provisional joint suggestions and may contribute to further clarification into the practical management of patients with CML during pregnancy.
Footnotes
Conflict of interest statement
EA has served on scientific advisory boards and consulted for Novartis, Bristol Myers Squibb, Pfizer and Incyte. JA has served on scientific advisory boards and consulted for Ariad, Novartis, Bristol Myers Squibb, Pfizer, and Incyte. MM has consulted for Novartis, Bristol Myers Squibb, Pfizer, Ariad, and Takeda. EC reports consultancy and lectures for Novartis, Bristol Myers Squibb, consultancy for Fusion Pharma.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.