
Abstract
Renin–angiotensin system (RAS) blockade by angiotensin-converting enzyme inhibitors (ACEis) or angiotensin-receptor blockers (ARBs) has been related to anemia in various situations. We aimed to investigate whether discontinuation of RAS inhibitors improves erythropoiesis in patients with lower-risk myelodysplastic syndromes (LR-MDSs). Seventy-four patients with LR-MDS were divided into three groups matched for gender and age. Group A consisted of 20 hypertensive patients who discontinued RAS inhibitors and received alternative medications. Group B consisted of 26 patients who continued to receive ACEi/ARB and Group C included 28 patients (50% hypertensive) never exposed to ACEi/ARB. Half of the patients in each group were under treatment with recombinant human erythropoietin (rHuEPO). Data were collected at baseline and after 3, 6 and 12 months. Group A showed a significant increase in hemoglobin from 10.4 ± 1g/dL at baseline to 12.6 ± 1.2 g/dL after 12 months (p = 0.035) and in hematocrit (31.4 ± 3% versus 37.9 ± 4%, p = 0.002). Incident anemia decreased from 100% at baseline to 60% at 12 months (p = 0.043) despite a concomitant dose reduction in rHuEPO by 18% (p = 0.035). No changes in hemoglobin and hematocrit were observed in both Group B and Group C. In the subset of patients not treated with rHuEPO, improvement of erythropoiesis was found only in Group A, as measured by changes in hemoglobin (11.5 ± 1 g/dL versus 12.4 ± 1.3 g/dL, p = 0.041) and hematocrit (34.5 ± 3% versus 37.1 ± 4%, p = 0.038) after 12 months. In contrast, Group B and Group C decreased hemoglobin and hematocrit after 12 months (p < 0.05). In conclusion, discontinuation of ACEi/ARB in LR-MDS patients is followed by a significant recovery of erythropoiesis after 12 months.
Keywords
Introduction
Myelodysplastic syndromes (MDSs) represent a heterogeneous group of clonal hematopoietic stem cell disorders which are characterized by ineffective hematopoiesis and represent one of the most challenging health-related problems in the elderly.1,2 Every case is classified according to the World Health Organization (WHO) 2016 criteria 3 and prognosis is based on International Prognosis Scoring System (IPSS) 4 and revised IPSS (IPSS-R). 5 Patients with lower-risk MDS (LR-MDS) (low and intermediate-1 according to IPSS and very low, low and intermediate according to IPSS-R) present with peripheral blood cytopenias. Anemia represents the most common cytopenia6,7 and recombinant human erythropoietin (rHuEPO) or darbepoetin is the first-line treatment of anemia in most LR-MDSS without del(5q) abnormality. 1 Various pathogenetic causes can lead to these disorders, including genetic abnormalities within myeloid progenitors, epigenetics alterations and changes in the bone marrow microenvironment.8,9 Thus, MDSs constitute several distinct entities that share common changes in blood and bone marrow.
Many experimental and clinical studies have revealed that the renin–angiotensin system (RAS) is significantly involved with the regulation of red blood cell mass. As a consequence, RAS blockade by angiotensin-converting enzyme inhibitors (ACEis) and angiotensin receptor blockers (ARBs) has been associated with a hemoglobin-lowering effect and/or anemia in various clinical situations. In otherwise uncomplicated patients, RAS blockade can cause statistically, but not clinically, important decrease in hematocrit values (~1%) and hemoglobin concentrations (~0.3 g/dL). 10 However, when bone marrow has need of every possible stimulus to enhance erythropoiesis, RAS blockade can increase the risk of de novo anemia, such as in chronic kidney disease (CKD), in renal transplant recipients and in patients with non-proliferative glomerulonephritis.11–14 In patients with heart failure, the prevalence of anemia has increased by an estimated 16%, from prior to the discovery of RAS blockers to the modern era, when RAS blockade is considered the basic treatment modality. 15 In addition, RAS blockade has been used to lower and normalize the hematocrit values in polycythemic patients.16–18
Although anemia is the most common cytopenia affecting patients with MDS, the role of RAS in such patients has not yet been addressed. Therefore, our goal was to investigate whether discontinuation of ACEi/ARB for 1 year in patients with LR-MDS could have any favorable effect in hemoglobin concentration, hematocrit values or dosage of rHuEPO used, in comparison with age and gender matched counterparts that either maintained a regimen based on RAS inhibitors or never administered RAS inhibitors.
Methods
Study design
In this single-center prospective study, a total of 74 elderly stable patients on antihypertensive medications with LR-MDS and anemia, half on rHuEPO treatment, were recruited consecutively from the Hematology Unit outpatient clinic of the University General Hospital “Attikon” between March 2018 and June 2019. Bone marrow aspiration, biopsy and cytogenetic analysis had been performed in all patients. The diagnosis of MDS was based on the WHO 2016 criteria 3 and the risk stratification was made according to the IPSS 4 and IPSS-R scoring systems. 5 Anemia was defined according to the WHO criteria as a hemoglobin <12 g/dL for female and <13 g/dL for male patients. 3 Patients with malignancies, chronic inflammatory disease, chronic obstructive pulmonary disease, moderate or severe CKD [estimated glomerular filtration rate (eGFR) ⩽45 ml/min per 1.73 m2], liver failure, iron, vitamin B12 or folate deficiencies, history of alcohol abuse, hemolytic anemia, blood loss and bleeding disorders were excluded.
To investigate the role of RAS in erythropoiesis of patients with LR-MDS, three groups of patients were followed for 1 year. Group A consisted of 20 patients who were evaluated by their physician and found capable to safely discontinue RAS inhibitors and receive therapy with a different class of antihypertensive medications. In particular, 13 patients received calcium channel blockers, five patients received diuretics and two patients were treated with β-blockers. Group B consisted of 26 patients who continued to receive ACEi/ARB because their physician felt uncomfortable to discontinue them. Finally, Group C included 28 patients. Of those, 14 were hypertensive subjects who had never been treated with ACEi/ARB, whereas the remaining 14 patients did not have hypertension. This group served as control group. Data were collected at baseline and patients were re-evaluated as outpatients after 3, 6 and 12 months. At baseline and at each follow-up visit we measured hematocrit values, hemoglobin concentrations, mean corpuscular volume (MCV) of the red blood cells, blood urea nitrogen and creatinine. We calculated eGFR using the Cockcroft–Gault formula as follows: [(140 – age in years) × body weight in kg/(72 – serum creatinine in mg/dL)]( × 0.85 if female). In addition, we recorded the dosage of rHuEPO in the subset of patients treated with exogenous erythropoietin. Two sequential measurements of the brachial blood pressure in the right arm separated by a 2 min interval were obtained and the mean was used for statistical analysis.
The current study conforms to the principles outlined in the Declaration of Helsinki and ethical approval was obtained from the Ethics Committee of University General Hospital “Attikon” (Approval number: 166/05-03-2018). All participants provided written informed consent.
Statistical analysis
The Statistical Package for Social Sciences 21.0 for Windows (SPSS Inc., Chicago, Illinois, United States) was used for analysis. Data are reported as mean ± standard deviation or median with interquartile range (first quartile–third quartile). Analysis of variance (ANOVA) was applied for paired comparisons (3 or 6 or 12 months versus baseline) using post-hoc analysis with Bonferroni correction. The F and p values of the factorial ANOVA for the comparison between groups were calculated. Categorical data were analyzed using the chi-square test. A p-value of less than 0.05 (p < 0.05) was considered statistically significant for all tests.
Results
Baseline demographic, clinical and laboratory data
Table 1 summarizes the demographic, clinical and laboratory data in the three groups at baseline. Seventy-four patients (45 men and 29 women) with LR-MDS were included in this study, with a median age of 78 years (interquartile range: 72–82 years). Based on the WHO 2016 classification, 31 (42%) patients were diagnosed with MDS with single lineage dysplasia (MDS-SLD), two (3%) with MDS with ring sideroblasts and single lineage dysplasia, 37 (50%) with MDS with multilineage dysplasia (MDS-MLD), one (1%) with MDS with excess blasts, type I , two (3%) with MDS with isolated deletion of chromosome 5q [MDS with del(5q)] and one (1%) patient with chronic myelomonocytic leukemia – 0. According to the IPSS, 69 (93%) patients were classified in the low-risk group and five (7%) patients in the intermediate-1 group. In addition, according to IPSS-R, 14 (19%) patients were categorized in the very low-risk group, 57 (77%) patients in the low-risk group and three (4%) in the intermediate-risk group.
Baseline demographic, clinical characteristics and laboratory data.
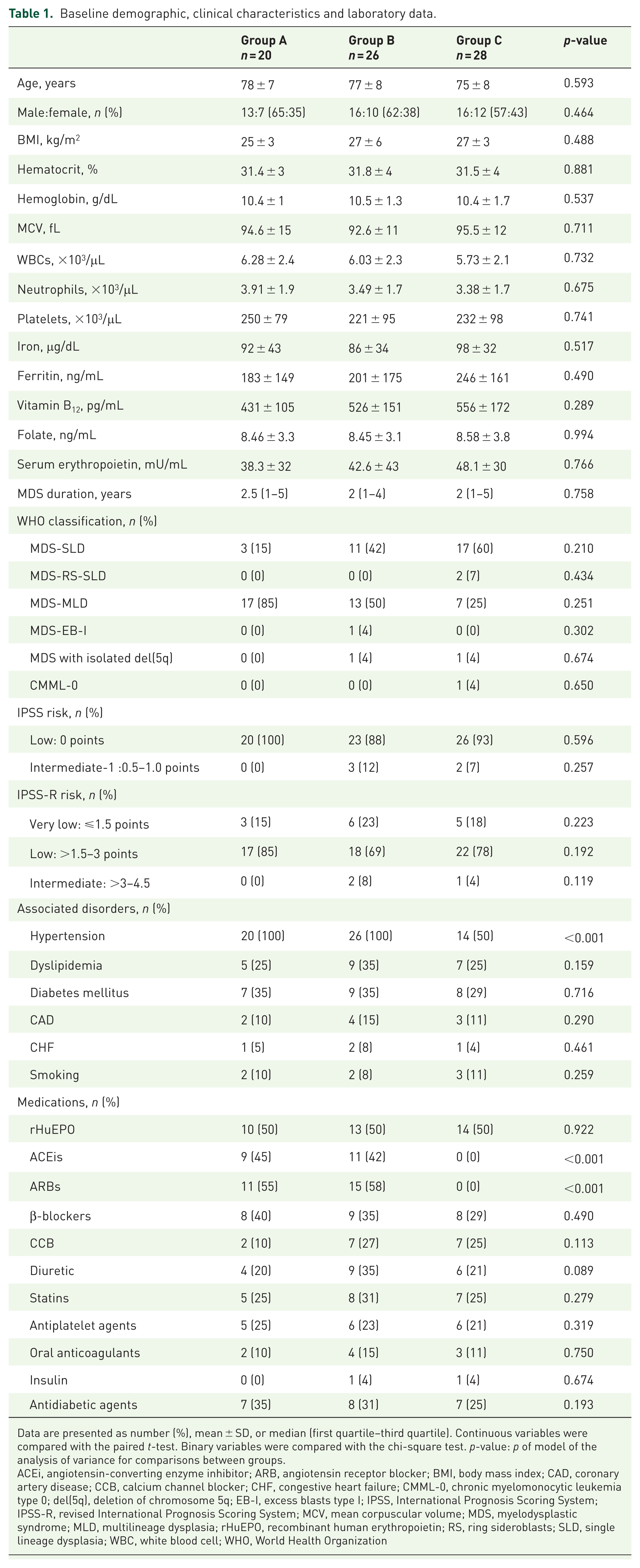
Data are presented as number (%), mean ± SD, or median (first quartile–third quartile). Continuous variables were compared with the paired t-test. Binary variables were compared with the chi-square test. p-value: p of model of the analysis of variance for comparisons between groups.
ACEi, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; BMI, body mass index; CAD, coronary artery disease; CCB, calcium channel blocker; CHF, congestive heart failure; CMML-0, chronic myelomonocytic leukemia type 0; del(5q), deletion of chromosome 5q; EB-I, excess blasts type I; IPSS, International Prognosis Scoring System; IPSS-R, revised International Prognosis Scoring System; MCV, mean corpuscular volume; MDS, myelodysplastic syndrome; MLD, multilineage dysplasia; rHuEPO, recombinant human erythropoietin; RS, ring sideroblasts; SLD, single lineage dysplasia; WBC, white blood cell; WHO, World Health Organization
Patients in the three groups were comparable in baseline demographic and clinical characteristics, such as age, gender, body mass index, blood pressure, the duration of MDS and its classification according to WHO 2016. It is worth mentioning that in Group A there was an increased number of patients with MDS-MLD compared with Group B and Group C, but this difference was not statistically significant (Table 1). None of the patients needed blood or platelets transfusions. Furthermore, none of our patients were on treatment with granulocyte-colony stimulating factor at inclusion or during the study period. The traditional cardiovascular risk factors, including dyslipidemia, diabetes mellitus, coronary artery disease, heart failure, cigarette smoking and anemia, were similar among the groups. All patients in Groups A and B were hypertensive on ACEi/ARB, but only half of patients in Group C were hypertensive on antihypertensive medications other than RAS inhibitors, as per study protocol.
Baseline hematocrit values and hemoglobin concentrations, white blood cell and platelet counts were comparable among the groups. All patients had normal levels of iron, ferritin, vitamin B12, folate and serum erythropoietin concentration. Half of the patients in each group were administered rHuEPO (epoetin alfa) as a subcutaneous injection. The median weekly rHuEPO dose was 40,000 units (interquartile range: 20,000–40,000 units) and was titrated according to the standard clinical practice. 19 Renal function, as measured by eGFR, was comparable in all patients (Table 2).
Changes in hematologic parameters, markers of renal function and blood pressure by the study groups during the follow-up period.
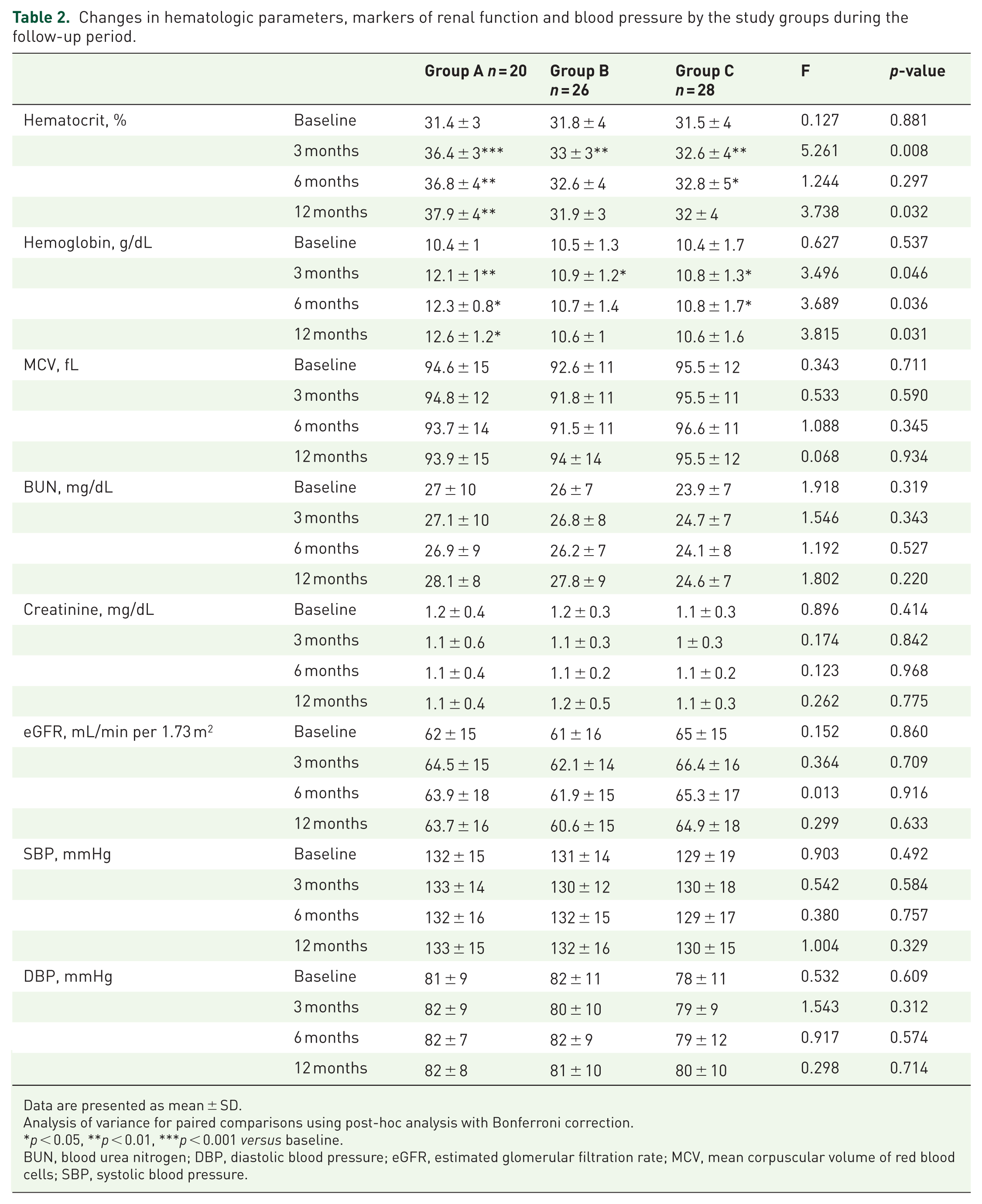
Data are presented as mean ± SD.
Analysis of variance for paired comparisons using post-hoc analysis with Bonferroni correction.
p < 0.05, **p < 0.01, ***p < 0.001 versus baseline.
BUN, blood urea nitrogen; DBP, diastolic blood pressure; eGFR, estimated glomerular filtration rate; MCV, mean corpuscular volume of red blood cells; SBP, systolic blood pressure.
Study outcomes
The hematocrit values and hemoglobin concentrations at baseline and at 3, 6 and 12 months of observation are summarized in Table 2 and Figure 1. Patients in Group A showed a significant improvement in erythropoiesis after discontinuation of RAS inhibition, as evidenced by increase in hemoglobin concentration from 10.4 ± 1 g/dL at baseline to 12.6 ± 1.2 g/dL after 12 months (p = 0.035) and in hematocrit values from 31.4 ± 3% at baseline to 37.9 ± 4% after 12 months (p = 0.002). Incident anemia decreased from 100% at baseline to 60% at 12 months (p = 0.043) despite a concomitant dose reduction in rHuEPO by 18% (p = 0.035; Figure 2). In line with these findings, two patients (10%) of Group A discontinued rHuEPO owing to adequate hematologic response at 3 and 12 months respectively. Both patients were on treatment with 40,000 units per week subcutaneously. The increase in hemoglobin concentrations and hematocrit values seen in Group A after discontinuation of RAS inhibition were similar between those under ACEi and those under ARB (data not shown). In sharp contrast, no changes in hemoglobin concentrations and hematocrit values from baseline were observed in both Group B and Group C. Moreover, no significant changes in MCV of red blood cells and markers of renal function, such as serum creatinine and eGFR, were revealed throughout the follow-up period compared with baseline values among the study groups (Table 2).

The changes in hemoglobin concentrations in the three study groups during the follow-up period. Data are presented as mean ± SD.

Change in recombinant human erythropoietin dose per week after 12 months follow-up. The Τ lines on the bars of the figure indicate standard deviation of the mean value.
Table 3 shows the changes in hemoglobin concentration and hematocrit values in relation to the use of rHuEPO at 3, 6 and 12 months. The discontinuation of ACEi/ARB in Group A patients increased the response to rHuEPO administration compared with Group B and Group C patients. Thus, in Group A, Group B and Group C at 3 months hemoglobin concentration increased by +3 ± 1.2 versus +0.5 ± 0.3 and +1.3 ± 0.7 g/dL, respectively, (p = 0.007) and hematocrit values increased by +8.7 ± 2.5 versus +2.1 ± 0.8 and +2.9 ± 1, respectively, (p = 0.015). These differences were maintained throughout the study. Of particular interest, the improved erythropoiesis in Group A patients on rHuEPO at 12 months was attained despite a greater reduction of rHuEPO dose compared with their counterparts in Group B and Group C (–18% versus –4% and –5%, respectively, p = 0.035; Figure 2).
Changes in hematocrit levels and hemoglobin concentration in relation to use of recombinant human erythropoietin (rHuEPO) by the study groups during the follow-up period.

Data are presented as mean ± SD or median (first quartile–third quartile).
p < 0.05, **p < 0.01, ***p < 0.001 for paired comparisons by analysis of variance (ANOVA) using post-hoc analysis with Bonferroni correction.
p < 0.05, ††p < 0.01 of the factorial ANOVA for comparisons between groups using post-hoc analysis with Bonferroni correction.
In the subset of patients not treated with rHuEPO, definite improvement of erythropoiesis was found in Group A after discontinuation of ACEi/ARB, as measured by hemoglobin concentrations, which increased from 11.5 ± 1 g/dL at baseline to 12.4 ± 1.3 g/dL after 12 months (p = 0.041), and by hematocrit values, which increased from 34.5 ± 3% at baseline to 37.1 ± 4% after 12 months (p = 0.038). In contrast, Group B patients decreased hemoglobin concentration from 11.6 ± 1.3 g/dL at baseline to 10.8 ± 1 g/dL after 12 months (p = 0.046) and hematocrit values from 34.9 ± 4% at baseline to 32.4 ± 3% after 12 months (p = 0.042). Similarly, in Group C patients, hemoglobin concentration decreased from 11.7 ± 1.6 g/dL at baseline to 10.3 ± 1.7 g/dL after 12 months (p = 0.033) and hematocrit values from 34.8 ± 4% at baseline to 32.2 ± 4% after 12 months (p = 0.045).
Discussion
This prospective observational study in elderly hypertensive patients with LR-MDS has demonstrated for the first time that discontinuation of ACEi/ARB and administration of antihypertensive medications of a different class resulted in improved erythropoiesis, as evidenced by statistically and clinically significant increase in hematocrit values and hemoglobin concentrations, a drop in incident anemia by 40%, despite reduced dosage of rHuEPO for those requiring exogenous erythropoietin administration. This improvement became apparent after 3 months and was sustained for at least the 1 year of observation. In contrast, worsening of anemia was witnessed during the same period of observation in those maintained on ACEi/ARB or in the control group with patients never treated with RAS blockade. These findings may have clinical and financial implications and deserve further study.
Our patients had no other specific etiology of anemia other than MDS. We had excluded patients with hemodilution, proinflammatory cytokines, loss of blood, malignancies, hepatic disease or uremia. Hematinic parameters, such as iron, ferritin, vitamin B12 and folate, were within normal limits. Anemia in MDS is due to ineffective erythropoiesis, and exogenous rHuEPO therapy may induce erythroid response rates in 40–50% of LR-MDS patients with a median duration of response of approximately 24 months.1,20 The clinical and biological factors that have been shown to be predictive of the response to erythropoietin therapy in patients with MDS have included short duration of disease, low (<2 units per month) or no blood transfusion requirement, baseline serum erythropoietin levels range from <100 to <500 U/L, bone marrow blasts <10%, IPSS low or intermediate-1, normal karyotype, no multi-lineage dysplasia and WHO subtypes MDS-SLD and MDS-RS.19–23 In the present study, the majority of patients met the previously mentioned criteria for a favorable response to rHuEPO.
The RAS, and in particular angiotensin II, its active octapeptide, has been recognized as a regulator of erythropoiesis over the past 20 years. 24 Hematocrit values are higher in renovascular hypertension, the prototype of RAS activation and in transgenic mice carrying both the human renin and angiotensinogen genes.25,26 Hematocrit values remained normal when the two transgenes were introduced into the AT1-receptor knockout animals. 26 Knockout mice for the angiotensin-converting enzyme (ACE), angiotensinogen or angiotensin II genes develop significant anemia, which is successfully treated with angiotensin II infusion.27,28 The mechanism(s) by which RAS increases red blood cell mass has not yet been fully elucidated. Angiotensin II can augment erythropoietin (EPO) secretion by causing vasoconstriction of the efferent arteriole, ischemia of renal parenchyma and stimulation of hypoxia inducible-factor 1, the transcription factor regulating EPO production.24,29 Both serum EPO levels and kidney EPO messenger RNA expression significantly increased in the double-transgenic mice carrying both the human renin and angiotensinogen genes compared with the wild-type controls. 26 The effect of angiotensin II on EPO secretion seems to make use of the AT1 receptor, 30 since pretreatment with losartan could completely block EPO secretion induced by angiotensin II infusion in healthy individuals. 31 On the other hand, immunohistological studies showed expression of ACE protein in erythroid precursors of normal and myeloproliferative bone marrow. 32 Interestingly, ACE expression in erythropoietic cells was stronger in MDS samples than in normal bone marrow. 32 Indeed, angiotensin II is a direct growth factor of erythroid progenitors via specific AT1 receptors on their surface, 33 while at the same time it decreases hepcidin production and affects iron transporters to assist iron absorption and use. 34
If RAS activation augments erythropoiesis, RAS blockade should be expected to exert a hematocrit-lowering effect and/or anemia in a variety of clinical conditions. In the SOLVD study, including patients with congestive heart failure, new anemia developed in 11.3% of the study group treated with enalapril compared with 7.9% of the control group on placebo after 1 year of follow-up. 35 In a meta-analysis of seven studies with almost 30,000 patients, the risk of anemia increased by more than 50% in patients on RAS blockers compared with patients treated with other antihypertensive medications. 36 Of particular interest, the hematocrit values may rise gradually toward pretreatment levels within 3 months after discontinuation of RAS blockers.12,18 The involvement of RAS activation seems to be blown up when bone marrow has need of all available stimuli to augment erythropoiesis, as is the case of patients with MDS.
To the best of our knowledge, this is the first study to implicate RAS inhibition in the pathogenesis of anemia in MDS and to propose that discontinuation of ACEi/ARB may be a novel therapeutic modality that could decrease incident anemia and reduce dosage of rHuEPO, at least in those patients with LR-MDS. One limitation of our study was that it was a single-center prospective observational study without randomization, since we had to consult with patients’ primary physicians in order to obtain their consent to discontinue RAS blockade. Another limitation was the small sample size, which could prevent our findings from being extrapolated. However, to our advantage there was no heterogeneity among the groups at baseline. Although there were numerically more patients with MDS-MLD in Group A compared with Group B and Group C, this difference was not statistically and clinically significant so as to affect the erythropoiesis. Moreover, the period of observation was long enough to allow us to clearly demonstrate the effect of discontinuation of RAS inhibition on erythropoiesis in LR-MDS.
In conclusion, discontinuation of RAS blockade and use of antihypertensive medications of a different class when possible, in elderly hypertensive patients with LR-MDS, is associated with a significant recovery of erythropoiesis over 1 year of observation, as evidenced by lower incident anemia rates and increased hemoglobin and hematocrit levels despite a significant reduction in rHuEPO requirements in the subset of patients requiring exogenous erythropoietin. These beneficial effects were visible as early as the first trimester and lasted during 12 months of observation. Further prospective randomized clinical trials, with the appropriate laboratory surveillance, are required to test the safety and efficacy of discontinuation of RAS in patients with MDS for longer periods of time, especially in patients with cardiac and renal co-morbidities.