
Abstract
Objective
To compare the potential beneficial effects of the angiotensin converting enzyme inhibitor (ACEI) benazepril and the angiotensin II receptor 1 blocker (ARB) irbesartan on vaginal vascular remodeling and fibrosis in female spontaneously hypertensive rats (SHRs).
Methods
Twelve-week-old female SHRs were treated with irbesartan or benazepril for 12 weeks. Vaginal renin angiotensin system (RAS) components were detected by polymerase chain reaction and western blot and vaginal α-smooth muscle actin (α-SMA), endothelial nitric oxide synthase (eNOS), and collagen III (Col III) were analyzed by western blot. Vaginal tissue sections were examined by hematoxylin and eosin staining, Masson trichrome staining, and immunohistochemical analysis of α-SMA and Col III.
Results
Irbesartan and benazepril had different impacts on vaginal RAS components. Both agents decreased vaginal α-SMA and Col III and increased eNOS expression in SHR. The wall/lumen thickness ratio of vaginal arterioles was similarly decreased following irbesartan and benazepril treatment. Both drugs also decreased collagen deposition in SHRs. There was no difference in vaginal vascular remodeling or fibrosis between the two groups.
Conclusions
Irbesartan and benazepril have different effects on vaginal RAS expression but similar positive effects against vaginal vascular remodeling and fibrosis.
Keywords
Introduction
Available data indicate that female sexual dysfunction (FSD) is more frequent in hypertensive compared with normotensive individuals.1–4 Sexual dysfunction was experienced by 42.1% of hypertensive women, compared with 19.4% of normotensive women in one previous study, 1 while our earlier clinical study showed that FSD occurred in 60.4% of hypertensive women but only 26% of normotensive women. 5 Despite large discrepancies in reported incidences among studies, related to differences in study populations and methods, FSD has consistently been found to be more common among women with hypertension. Hypertension was associated with diminished sexual desire and increased vaginal dryness. 3 Although the mechanism of FSD is still poorly understood, vaginal vascular function is known to play a significant role in female sexual function, and increased blood flow to the vagina, clitoris, and labia is responsible for the vasocongestion, engorgement, and lubrication involved in the sexual arousal response. 6 Endothelial dysfunction in the female lower genital organs 7 and fibrosis might thus be the important mechanisms of FSD in women with hypertension.
Hypertension-related erectile dysfunction and the impact of antihypertensive pharmacotherapies on sexual function in men have received significant attention; however, fewer studies have examined the effects of hypertension on FSD. Some classes of antihypertensive drugs have been shown to cause sexual dysfunction in hypertensive women, including thiazide diuretics and non-selective beta blockers.1,2,5,8,9 In contrast, angiotensin II receptor 1 blockers (ARBs), as renin angiotensin system (RAS) inhibitors, could protect and possibly improve sexual function.5,9 A randomized controlled trial conducted by Fogari et al. 9 showed that valsartan improved sexual function in women in terms of sexual desire, sexual activity, and sexual fantasies. In a previous randomized controlled study, 5 we showed that irbesartan improved certain aspects of sexual function in women with hypertension, such as sexual desire. However, there is currently little evidence to support an effect of other RAS inhibitors, angiotensin converting enzyme inhibitors (ACEIs), on sexual function. 10 Sexual dysfunction has important effects on quality of life, and although women are less likely to talk about this issue, clinicians should pay attention to this problem when prescribing medications, to minimize sexual side effects and maximize the quality of life and compliance with therapy.
RAS components have been identified in the female reproductive organs, including the ovaries. 11 Angiotensin II regulates the function of these organs via angiotensin II receptors, including AT1R and AT2R. Excessive angiotensin II in hypertensive patients could induce vascular and smooth muscle contraction, exacerbate inflammation and oxidative stress through AT1R, and enhance proliferation, hypotrophy, and fibrosis in the heart, liver and kidney. AT2R is thought to have opposing properties to AT1R, with peripheral vasodilatory, anti-growth, and anti-inflammatory benefits. Angiotensin-(1-7) is a natural agonist of angiotensin II that acts via the Mas receptor (MasR) to induce anti-proliferative effects (Figure 1).
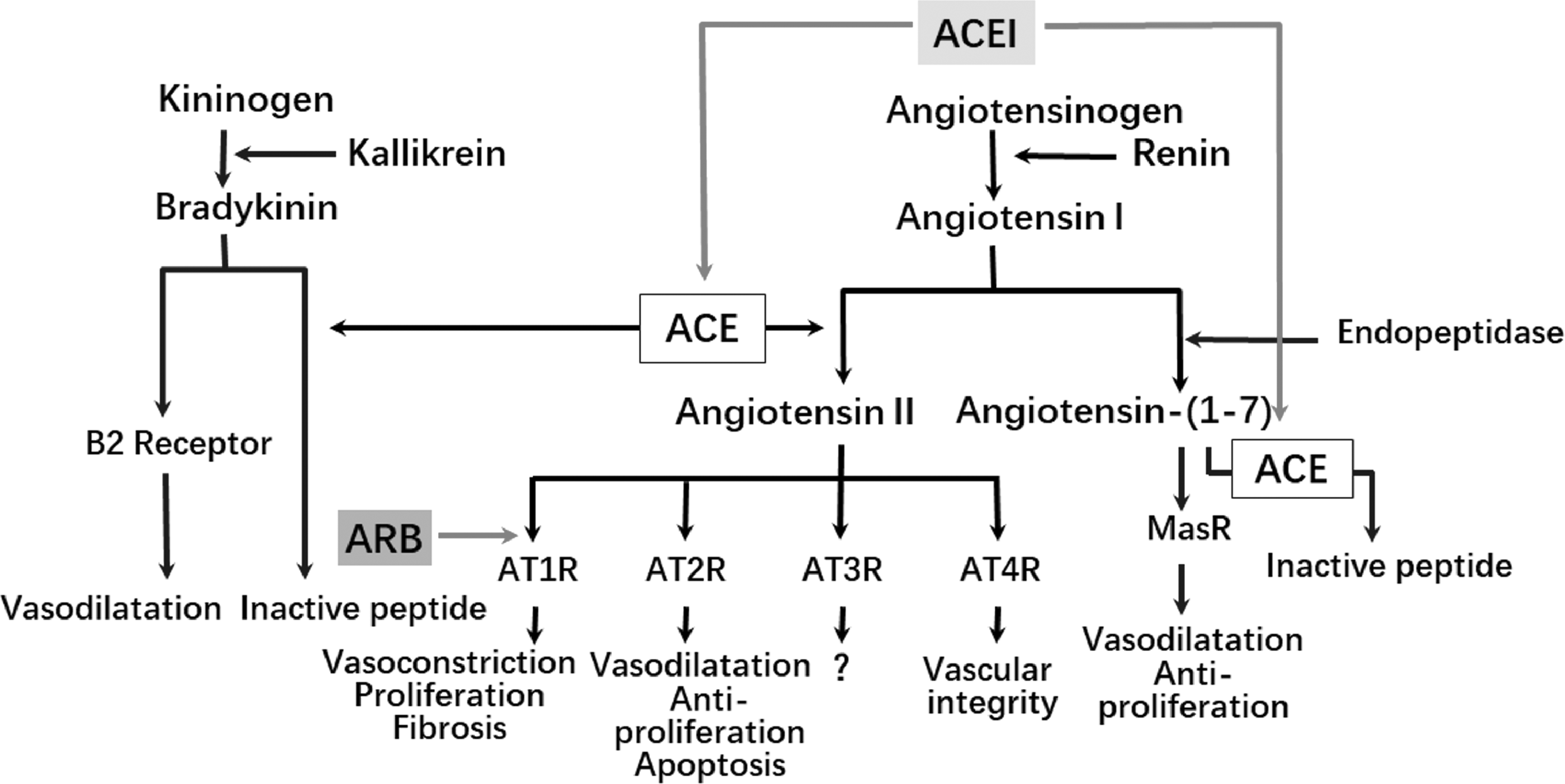
Schematic diagram of renin angiotensin system and the effects of angiotensin II receptor 1 blockers and angiotensin converting enzyme inhibitors.
ARBs and ACEIs both attenuate the effects of angiotensin II, albeit by different mechanisms. ARBs prevent the AT1R-mediated effects of angiotensin II by binding to AT1R (Figure 1), while ACEIs reduce the generation of angiotensin II by inhibiting angiotensin converting enzyme (ACE), which catalyzes angiotensin II production (Figure 1). ARBs and ACEIs thus both ameliorate oxidative stress and fibrosis by inhibiting RAS via different mechanisms. We hypothesized that both ACEIs and ARBs may have beneficial effects on indicators of vascular remodeling and fibrosis in the vagina.
This study aimed to compare the effects of an ARB and an ACEI on RAS components in vaginal tissue in hypertensive rats. We also compared α-smooth muscle actin (α-SMA) expression and the thickness of the arteriole vascular wall, as indicators of vascular remodeling, endothelial nitric oxide synthase (eNOS) expression, as an indicator of oxidative stress, and collagen III (Col III) expression and collagen deposition, as indicators of fibrosis in vaginal tissues from hypertensive rats treated with these two types of drugs.
Materials and methods
Animals and treatments
Thirty-nine 12-week-old female spontaneously hypertensive rats (SHRs) and thirteen 12-week-old female Wistar–Kyoto (WKY) rats (Vital River Laboratory Inc., Beijing, China) were included in this study. All the animals were housed in individual cages on a 12-h light–dark cycle in a room with controlled temperature (21±1°C) and humidity (50% to 60%) and allowed access to standard rodent chow and distilled water ad libitum. Vaginal smears and cytology were performed for 2 weeks to confirm a continuous estrous cycle prior to grouping. SHRs were then randomly allocated to three groups (n=13 each): SHR rats treated with vehicle; SHR + Irb rats treated with 30 mg/kg per day irbesartan (Sanofi-Aventis, France); and SHR + Ben treated with 8 mg/kg per day benazepril (Novartis, Switzerland). Thirteen WKY rats received vehicle. The stochastic sequence was generated using a computer. Irbesartan and benazepril were dissolved in 1 mL normal saline and administered orally once daily to rats in the SHR + Irb and SHR + Ben groups, respectively, via a gastric tube. The SHR and WKY groups received 1 mL saline via a gastric tube daily. The rats were treated for 12 weeks and vaginal smears and cytology were then performed for up to 4 consecutive days after which the rats were sacrificed. The animal protocol was approved by Lanzhou University Second Hospital Ethics Committee and followed the Regulations of Experimental Animals in China (National Scientific and Technological Commission, revised in 2013).
Blood pressure measurement
Systolic and diastolic blood pressure were measured at the beginning of the treatment and every 2 weeks thereafter using tail-cuff plethysmography (Alcott Biotech, China). The rats were kept calm in animal holders and then placed in a restrainer for 15 minutes, the cuff was attached to their tail, and the blood pressure was then recorded. Three readings were taken for each rat and averaged. The blood pressure values at the beginning of the treatment and at week 12 were included in the analysis.
Vaginal cytology
Vaginal cytology is a non-invasive method used to determine the stage of the estrous cycle, based on the presence or absence of specific cell types and associated characteristics. 12 In this study, vaginal lavage fluid was collected daily between 8 and 10 a.m., as described previously. 13 Vaginal cells were flushed by introducing 50 μL of sterile saline (NaCl 0.9%) through a pipette and the collected fluid was then put on a glass slide and evaluated immediately, fresh and unstained. Slides were observed using a ×10 objective light microscope (DP72, Olympus Corporation, Japan). The estrous stage was classified as described previously. 14
Blood and tissue sample collection
After 12 weeks of treatment, all rats were anesthetized with 10% chloral hydrate (300 mg/kg, intraperitoneal). The adequacy of the anesthesia was verified based on a lack of response to a nociceptive stimulus. Heart rate was measured using an animal electrocardiograph monitor (SurgiVet V3404, Smiths Medical PM, Inc., MA, USA). Blood samples for estradiol determination were collected from the abdominal aorta via an abdominal incision. The lower third of the vagina was excised and harvested for real-time polymerase chain reaction (PCR) (n = 5), western blot analyses (n = 5), and histology (n = 3). The vaginal tissue samples were fixed in 10% formaldehyde neutral buffer solution and frozen in liquid nitrogen immediately after harvesting. The rats were then sacrificed by anesthesia with 10% chloral hydrate (1000 mg/kg, intraperitoneal). Death was verified by the termination of electrocardiograph signals, and the heart was then quickly excised and weighed to confirm the blood pressure data.
Serum estradiol detection
Serum estradiol was analyzed using a CCA461Ge pan-species chemiluminescent immunoassay kit for estradiol (Cloud-Clone Corp., TX, USA), according to the manufacturers’ protocol.
Real-time (RT)-PCR
mRNA levels of RAS components including ACE, ACE2, AT1R, AT2R, and MasR were measured in vaginal tissue samples by RT-PCR. Total RNA was extracted using TRizol® reagent according to the manufacturer’s instructions (Invitrogen Life Technologies, CA, USA) and measured using a Quawell UV-Vis Spectrophotometer Q5000 (Quawell Technology, Inc., CA, USA). Following cDNA synthesis, 2 µL of cDNA was mixed with 18 µL of Master Mix and PCR was performed using a QuantStudio 5 Real-Time PCR system (Thermo Fisher Scientific, Waltham, MA, USA) under the following conditions: 15 minutes at 94°C followed by 40 cycles of 94°C for 30 s, 60°C for 90 s, and 72°C for 90 s; and a final single incubation at 72°C for 10 minutes.15,16 The primers were as follows: ACE (sense 5′-ATTGCAGCCGGGCAACTTTT-3′; antisense 5′-CGCATTCTCCTCCGTGATGT-3′); ACE2 (sense 5-CGCTGTCACCAGACAAGAA-3′; antisense 5-CGTCCAATCCTGGTTCAAG-3′); AT1R (sense 5′-CACACAACCCTCCCAGAAAG-3′; antisense 5-TTGGGGCAGTCATCTTGG-3′); AT2R (sense 5′-TCATFGACCTGGCACTTCC-3′; antisense 5′-AACCCTAAACACACTGCGG-3′); MasR (sense 5′-CCTGCATACTGGGAAGACCA-3′; antisense 5′-TCCCTTCCTGTTTCTCATGG-3′) and β-actin (sense 5-CACACAACCCTCCCAGAAAG-3′; antisense 5′-TTGGGGCAGTCATCTTGG-3′). Expression of each gene was normalized to the housekeeping β-actin gene as a control. Relative gene expression levels were quantified using the 2−ΔΔCt method. 17
Western blot analysis
Tissue samples (n = 5) were homogenized and centrifuged at 12,000 × g for 5 minutes (4°C). After centrifugation, the supernatant was collected and the protein lysate was measured with a bicinchoninic acid protein assay kit (Cat. no. 23225; Pierce, Rockford, IL, USA) according to the manufacturer’s instructions. Equal amounts of protein lysates (15 µg) were separated by sodium dodecyl sulfate-polyacrylamide gel electrophoresis and transferred onto nitrocellulose membranes (Cat. no. ab133413; Abcam, Cambridge, UK). The blots were blocked with 5% (w/v) nonfat milk for 2 hours and incubated overnight at room temperature with the following rabbit polyclonal antibodies (1:500; Abcam, Cambridge, UK) against ACE (Cat. no. ab28311), ACE2 (Cat. no. ab65863), AT1R (Cat. no. ab124505), AT2R (Cat. no. ab92445), MasR (Cat. no. ab200685), α-SMA (Cat. no. ab5694), eNOS (Cat. no. ab5589), Coll III (Cat. no. ab7778), and β-actin (Cat. no. ab8227). After washing, the blots were further incubated with goat anti-rabbit secondary antibody (1:3000; Cat. no. ab7090; Abcam) for 1 hour at room temperature. Immunoreactive bands were visualized by chemiluminescence and exposed to the Gel Doc™ XR+ system (Bio-Rad, Hercules, CA, USA) for densitometric analysis. The optical density of the blots was analyzed using Image Lab software (Bio-Rad). 16 and the expression of each protein was normalized to β-actin as a control.
Histological procedures and immunohistochemical analysis
Lower vaginal tissues were prepared for microscopic examination (n = 3). Tissues were fixed with 10% formalin for 24 hours at room temperature, embedded in paraffin blocks, and then sectioned at 4 µm, starting from the lateral end of the vagina, and then stained with hematoxylin and eosin. The thickness of the arterioles in the vaginal walls and the wall/lumen thickness ratio were evaluated. Paraffin-embedded tissues were also stained with Masson trichrome to assess collagen deposition.
For immunohistochemical analysis, paraffin sections were deparaffinized and dehydrated, and then blocked with 3% H2O2 and 2% bovine serum albumin to remove endogenous peroxidase activity and to avoid nonspecific protein binding sites, respectively. The sections were then incubated overnight at 4°C with rabbit polyclonal first antibody against α-SMA (Cat. no. ab32575; Abcam) or Col III (Cat. no. ab32575; Abcam) at a dilution of 1:200 to evaluate vascular smooth muscle remodeling of arterioles in the vaginal walls and the process of fibrosis in the vaginal tissues, respectively. The sections were washed again and incubated overnight at 4°C with goat anti-rabbit IgG H&L (Biotin, TX, USA) secondary antibody (1:10,000; Cat. no. ab5694; Abcam) and goat anti-rat IgG at room temperature for 2 hours. Finally, the sections were counterstained with hematoxylin, dehydrated, mounted and examined under a light microscope (DP72, Olympus) using a ×10 eyepiece lens and a ×20 objective lens. The images were analyzed with Image-Lab Plus Software, version 6.0 (Media Cybernetics, Inc., Silver Spring, MA, USA) and expression levels were estimated by integrated optical density/area, as the average cumulative optical density of the positive staining area for each group.
Statistical analysis
The results are presented as mean ± standard deviation. The data were analyzed statistically using SPSS Statistics for Windows, version 22.0 (SPSS Inc., Chicago, IL, USA). Differences among groups were compared by analysis of variance (ANOVA) followed by the Student–Newman–Keuls test. A value of P < 0.05 was considered statistically significant.
Results
General features of rats
The body weights of the rats immediately before sacrifice were comparable among the groups. Heart weight was significantly higher in SHR compared with WKY rats (P < 0.05). There was no significant difference in body weight or heart weight between the SHR + Irb and SHR + Ben groups (P>0.05). Systolic and diastolic blood pressure were significantly higher in the SHR group compared with the WKY group (P < 0.01). Irbesartan and benazepril both significantly decreased systolic and diastolic blood pressure in SHRs compared with vehicle-treated SHRs (P < 0.01). There was no significant difference in systolic or diastolic blood pressure after treatment between the SHR + Irb and SHR + Ben groups (Table 1).
General features and serum estradiol level of the rat groups at baseline and at the 12th week.
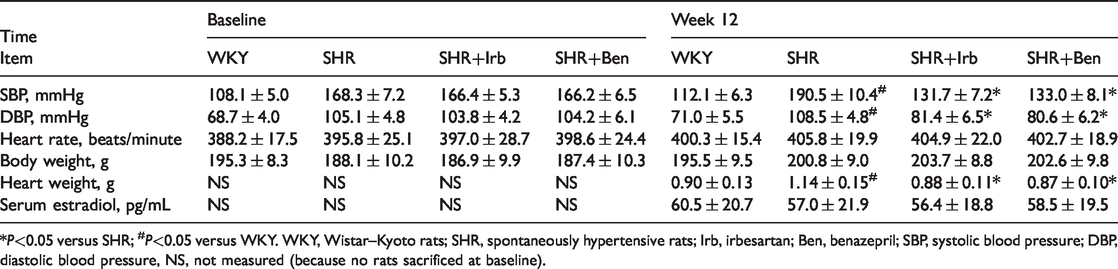
*P<0.05 versus SHR; #P<0.05 versus WKY. WKY, Wistar–Kyoto rats; SHR, spontaneously hypertensive rats; Irb, irbesartan; Ben, benazepril; SBP, systolic blood pressure; DBP, diastolic blood pressure, NS, not measured (because no rats sacrificed at baseline).
Serum estradiol concentration
There was no significant difference in estradiol concentrations among the four groups after 12 weeks of intervention (Table 1).
ACE, ACE2, AT1R, AT2R, and MasR mRNA expression levels in vaginal tissue
mRNA levels of vaginal RAS components differed between the SHR and WKY groups (Figure 2). Baseline mRNA expression levels of AT1R, MasR, ACE, and ACE2 were significantly lower and AT2R mRNA expression was significantly higher in the SHR group compared with the WKY group (all P < 0.05). Irbesartan and benazepril both significantly reduced AT1R mRNA expression levels in vaginal tissues in SHRs (both P < 0.05); however, the two drugs had significantly different effects on the other RAS components. Irbesartan upregulated mRNA expression levels of AT2R, MasR, and ACE (P < 0.05) and highly significantly increased mRNA expression of ACE2 (P < 0.01). In contrast, benazepril significantly downregulated mRNA expression levels of AT2R, MasR, and ACE compared with the control SHR group (P < 0.05) (Figure 2). ARBs and ACEIs thus had different influences on the RAS and the Mas axis at the mRNA level in the female lower genital tract.

Real-time polymerase chain reaction analysis of the mRNA expression levels of renin angiotensin system components in vaginal tissues from the WKY and SHR rats. mRNA levels of (a) Angiotensin converting enzyme, (b) angiotensin converting enzyme 2, (c) angiotensin II receptor 1, (d) angiotensin II receptor 2, and (e) Mas receptor. Graphs based on densitometric analysis of mRNA levels normalized to the expression of β-actin.
ACE, ACE2, AT1R, AT2R, and MasR protein expression levels in vaginal tissue
Protein levels of vaginal RAS components differed between the SHR and WKY groups (Figure 3). Baseline expression levels of ACE, ACE2, AT1R, and MasR were significantly decreased while AT2R expression was significantly increased in the SHR compared with the WKY group (all P < 0.05). Benazepril, but not irbesartan, significantly decreased the expression of ACE (P < 0.05). ACE2 expression was significantly increased in both the SHR + Irb and SHR + Ben groups (P < 0.01, P < 0.05, respectively) and was significantly higher in the SHR + Irb compared with the SHR + Ben group (P < 0.05). Similar reductions in AT1R expression occurred in the SHR + Irb and SHR + Ben groups (both P < 0.05). AT2R expression was significantly increased in the SHR + Irb group (P < 0.05) but significantly decreased in the SHR + Ben group (P < 0.05). There was no significant difference in MasR expression among the SHR, SHR + Irb, and SHR + Ben groups (Figure 3). These results indicate that irbesartan and benazepril had different impacts on protein levels of RAS components, including ACE, ACE2, and AT1R, in vaginal tissue in SHRs.

Western blot analysis of the protein expression levels of renin angiotensin system components in vaginal tissues from WKY and SHR rats. (a) Western blot. Graphs based on densitometric analysis normalized to the expression of β-actin for (b) angiotensin converting enzyme, (c) angiotensin converting enzyme 2, (d) angiotensin II receptor 1, (e) angiotensin II receptor 2, and (f) Mas receptor angiotensin converting enzyme 2.
α-SMA, eNOS, and Col III expression in vaginal tissue determined by western blot
α-SMA expression was significantly increased in vaginal tissue from SHR compared with WKY rats (P < 0.05). Both irbesartan and benazepril elicited significant decreases in vaginal α-SMA expression compared with the SHR control group (p < 0.01 for all), but α-SMA expression levels were comparable between the SHR + Irb and SHR + Ben groups (Figure 4).

Western blot analysis of α-smooth muscle actin (α-SMA), collagen III (Col III), and endothelial nitric oxide synthase (eNOS) in vaginal tissues from WKY and SHR rats. (a) Western blot. Graphs based on densitometric analysis of (b) α-SMA, (c) Col III, and (d) eNOS normalized to the expression of β-actin. *P<0.05 vs. SHR, #P<0.05 vs. WKY.
eNOS expression levels in vaginal tissue were significantly lower in SHR compared with WKY rats (P < 0.05). Both irbesartan and benazepril significantly augmented eNOS expression (both P < 0.05), with no significant difference between the SHR + Irb and SHR + Ben groups (Figure 4).
Col III protein expression levels in vaginal tissue were significantly higher in the SHR compared with the WKY group (P < 0.01). Col III expression was significantly reduced in both the SHR + Irb and SHR + Ben groups (both P < 0.05 ), with no significant difference between the two groups (Figure 4).
Histology and immunohistochemical analysis of vaginal tissue
The wall/lumen thickness ratio of the vaginal arterioles was significantly increased in the SHR compared with the WKY group (P < 0.05), and was significantly decreased in both the SHR + Irb and SHR + Ben groups (both P < 0.05), with no significant difference between these two groups (Figure 5).
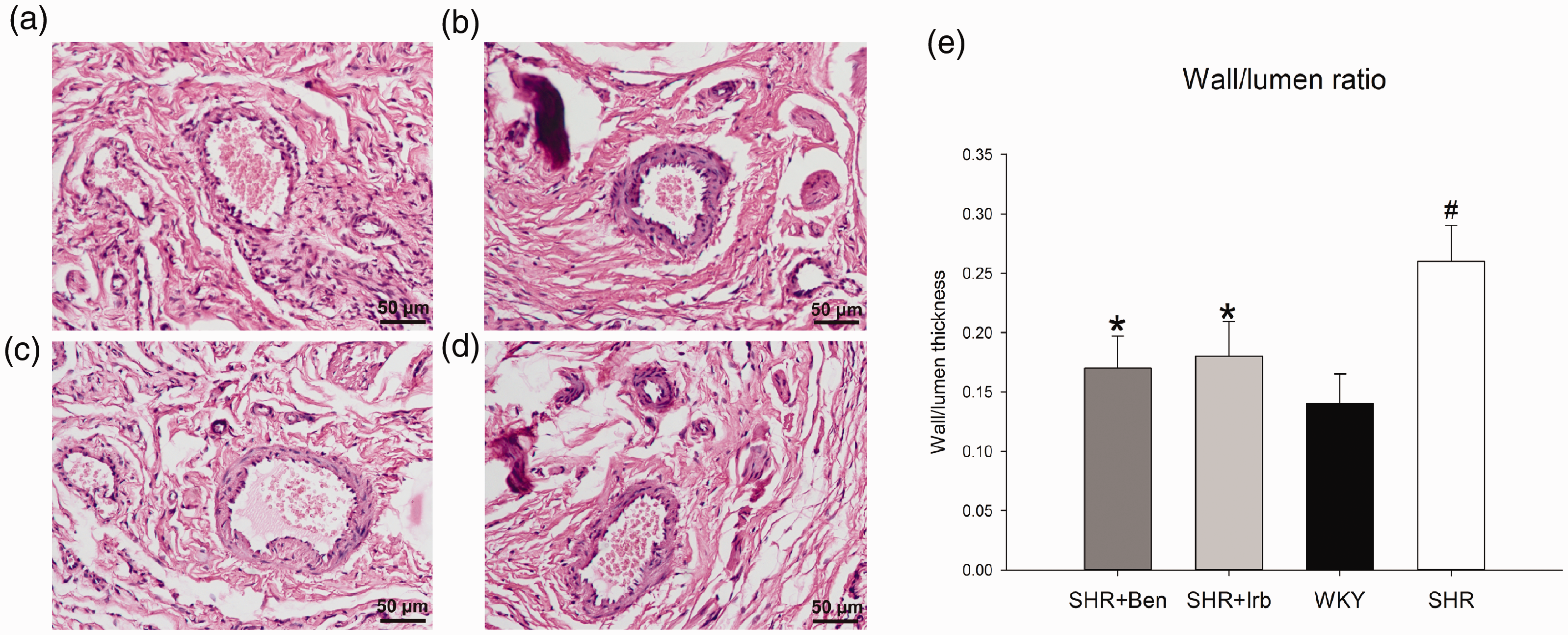
Coronal sections of lower vaginal tissues stained with hematoxylin and eosin (×200). (a) WKY, (b) SHR, (c) SHR + Irb, and (d) SHR + Ben groups. (e) Wall/lumen thickness ratio of arterioles in the vaginal wall
Immunohistochemical analysis showed that α-SMA expression in vaginal arterioles was significantly higher in the SHR compared with the WKY group (P < 0.01). α-SMA expression levels were significantly reduced in the SHR + Irb and SHR + Ben groups compared with the SHR control group (both P < 0.05). There was no significant difference in α-SMA expression in vaginal arterioles between the SHR + Irb and SHR + Ben groups (Figure 6).

Immunohistochemical analysis of α-smooth muscle actin (α-SMA) in vaginal arterioles (×200). (a) WKY, (b) SHR, (c) SHR + Irb, and (d) SHR + Ben groups. (e) α-SMA expression in the arterioles in the vaginal walls.
Col III expression levels in vaginal tissue were significantly higher in the SHR compared with the WKY group (P < 0.01), and were significantly decreased in the SHR + Irb and SHR + Ben groups compared with the control SHR group (both P < 0.05). There was no significant difference in Col III expression between the SHR + Irb and SHR + Ben groups (Figure 7).

Immunohistochemical analysis of collagen III (Col III) in vaginal tissue (×200). (a) WKY, (b) SHR, (c) SHR + Irb, and (d) SHR + Ben groups. (e) Col III expression in vaginal tissue.
Masson trichrome staining showed that collagen fibers in vaginal tissue were significantly increased in the SHR compared with the WKY group (Pp < 0.01), and were significantly decreased in the SHR + Irb and SHR + Ben groups compared with the control SHR group (both P < 0.05). There was no significant difference in collagen fibers between the SHR + Irb and SHR + Ben groups (Figure 8).

Masson trichrome staining of vaginal tissue (×200). (a) WKY, (b) SHR, (c) SHR + Irb, and (d) SHR + Ben groups. (e) Collagen deposition in vaginal tissue.
Discussion
The results of this study indicated that both irbesartan and benazepril had positive influences on vascular remodeling and fibrosis in vaginal tissue, despite having different impact on RAS expression. These results suggest that ACEIs, like ARBs, might help to prevent hypertension-related female genital vascular remodeling and fibrosis.
Sexual dysfunction affects 20% to 50% of women, and is more common in women than men; 18 however, sexual function in hypertensive women remains poorly studied. As in men with hypertension, women treated with some types of antihypertensive agents, including beta blockers or diuretics, commonly report sexual dysfunction as a possible medical adverse effects. ARBs seem to ameliorate sexual function,5,9but studies to establish the possible effects of antihypertensive agents on the pathophysiology of the female genital tract have been limited. The current experimental study thus provides important additional information in this field. A previous study reported that ramipril significantly reduced clitoral transforming growth factor-β expression and interstitial fibrosis in SHRs compared with metoprolol. 19 Although this supports the results of the current study, the previous study did not examine the effects of ARBs. Given that clinical evidence in both men and women with hypertension supports the beneficial effects of ARBs, but not ACEIs, on sexual function, 9 , 20 there is a need to compare these drug types to determine if ARBs are superior to ACEIs in terms of maintaining sexual function and protecting the female genital organs in women with hypertension. This is the first study to directly compare these two kinds of RAS inhibitors in relation to their protective roles in female genital organs.
It is still unclear if ARBs or ACEIs are superior for preventing target organ damage in hypertension. Although current guidelines recommend ACEIs and ARBs as first-line treatments for hypertension, these drugs are not interchangeable in all circumstances. ARBs are usually recommended for patients intolerant to ACEIs. 21 Many people also believe that ACEIs are inferior to ARBs in high-risk patients, such as those with diabetes mellitus.22,23 ARBs represent a valuable option to reduce cardiovascular mortality and morbidity in patients for whom ACEIs are unsuitable. 23 In this study, the two types of RAS inhibitors had similar effects in terms of increasing the vaginal expression of eNOS and decreasing the expression of α-SMA and Col III, decreasing the wall thickness of vaginal arterioles, and decreasing collagen fibers in vaginal tissue, suggesting that the beneficial effects of benazepril were not inferior to irbesartan. These results are consistent with clinical evidence.
To the best of our knowledge, the current study is the first to investigate the effects of ARBs and ACEIs on the expression of RAS components in female sexual organs. Angiotensin II is the main effector of the RAS, which is a complex hormonal system responsible for controlling vital physiologic functions, and which is also associated with the maintenance of erectile function in men. However, overactivation of angiotensin II in hypertension contributes to oxidative stress, endothelial dysfunction, inflammation, proliferation, and fibrosis, resulting in target organ damage. The results of the current study showed that expression levels of RAS parameters were altered in vaginal tissue from untreated hypertensive rats, with increased vaginal α-SMA expression, arteriole wall thickness, and collagen deposition. These results suggest that hypertension could lead to structural modifications and impairments in female vaginal vessels, along with unbalanced RAS expression in vaginal tissue. It is therefore reasonable to regard the female genital organs as target organs in hypertension.
Despite the different impacts of irbesartan and benazepril on vaginal RAS expression, both drugs had similar effects on vaginal vascular remodeling and fibrosis. The different mechanisms of action of ACEIs and ARBs may explain the similar protective effects of benazepril and irbesartan (Figure 1). ACEIs decrease the degradation of bradykinin, which is an important mediator of ischemic preconditioning, endothelial function, and fibrinolysis. Bradykinin also leads to the release of nitric oxide and prostaglandins, resulting in additional vasodilatation. 24 In contrast to ACEIs, ARBs do not upregulate bradykinin, but bind directly to the AT1R, preventing its activation by angiotensin II. Circulating angiotensin II may then bind to other angiotensin receptors, particularly AT2R, which usually shows low expression levels in adults.24,25 However, upregulation of AT2R may have negative consequences, 24 and some effects of angiotensin II on AT2R and other angiotensin II receptors remain unclear. ACEIs and ARBs also increase the expression of ACE2, which increases that of angiotensin-(1-7), a natural agonist of angiotensin II. In the current study, both benazepril and irbesartan upregulated the expression of ACE2 in vaginal tissue, with irbesartan being more effective, but neither upregulated the expression of MasR at the protein level. The biggest differences between the two drugs were that irbesartan upregulated AT2R expression while benazepril decreased ACE expression. These results indicate that benazepril and irbesartan exert their beneficial effects mainly by blocking the disadvantageous effects of angiotensin II in vaginal tissue. In summary, irbesartan and benazepril inhibited the RAS in different ways, and their different advantages made their respective benefits hard to compare.
RAS inhibitors might attenuate sexual dysfunction by reducing hypertension-related morphologic changes and improving the blood supply to the sexual organs. Hypertension in men is associated with erectile dysfunction and with an increase in collagen fibers in the sinusoids, thus increasing vessel wall thickness and collagen deposition. Vascular alterations can decrease the blood supply to the penis. 10 Hypertension may also affect the blood flow leading to inadequate vasocongestion during sexual arousal in women, resulting in decreased lubrication and leading to dyspareunia. 26 The current results demonstrated the morphologic changes in the vaginal arteries and tissues in hypertensive rats treated with an ARB or ACEI, and the results may improve our understanding of the favorable profile of RAS inhibitors in female sexual function.
This study could not be performed in animals with FSD or impaired sexual activity because there is currently no animal model of hypertension-induced FSD. However, further studies are planned to assess sexual function and to measure vaginal and genital blood flow, and to examine the dose-related effects of RAS inhibitors.
Footnotes
Acknowledgements
We thank Professor Jiuchang Zhong from the Heart Center of Beijing Chao-Yang Hospital for guidance with writing the paper, and Professor Yingdong Li from Gansu University of Traditional Chinese Medicine for providing laboratory support.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by the Natural Science Foundation of China [grant number 81670385], the Natural Science Foundation of Gansu Province, China [grant number 1506RJZA244], and the Cuiying Scientific and Technological Innovation Program of Lanzhou University Second Hospital, China [grant number CY2018-QN05].