
Abstract
The outcome of patients with relapsed/refractory classical Hodgkin lymphoma (rr-cHL) has improved considerably in recent years owing to the approval of highly active novel agents such as brentuximab vedotin and Programmed Death-1 (PD-1) inhibitors. Although no randomized trials have been conducted to provide formal proof, it is almost undisputable that the survival of these patients has been prolonged. As autologous stem-cell transplantation (SCT) remains the standard of care for second-line therapy of most patients with rr-cHL, optimization of second-line regimens with the use of brentuximab vedotin, or, in the future, checkpoint inhibitors, is promising to increase both the eligibility rate for transplant and the final outcome. The need for subsequent therapy, and especially allogeneic SCT, can be reduced with brentuximab vedotin consolidation for 1 year, while pembrolizumab is also being tested in this setting. Several other drug categories appear to be active in rr-cHL, but their development has been delayed by the appearance of brentuximab vedotin, nivolumab and pembrolizumab, which have dominated the field of rr-cHL treatment in the last 5 years. Combinations of active drugs in chemo-free approaches may further increase efficacy and hopefully reduce toxicity in rr-cHL, but are still under development.
Introduction
Hodgkin lymphoma (HL) is a relatively common B-cell malignancy with an annual incidence of ~2–3 per 100,000, accounting for ~10% of all lymphomas and <1% of all malignancies. The median age at diagnosis depends on the population analysed (clinical trials, retrospective series or population-based), with 10–20% of cases diagnosed after the age of 60 in most published series. However, the median age is highest (35–45 years) in SEER or UK population data, where the frequency of older age (>60 years) may exceed 20% or even 30%.1–3 The disease is characterised histologically by a minority of bi- or multinucleated or large mononuclear neoplastic cells, known as Reed-Sternberg and Hodgkin cells, respectively, and collectively called HRS cells, admixed with an abundant reactive nontumoral inflammatory microenvironment. 4 Based on morphology and immunohistochemistry, HL is subdivided into classical HL (cHL) and nodular lymphocyte-predominant HL (NLPHL), with ~95% of the cases falling into the broad category of cHL, which is discussed in this review. 5
With the advent of effective multiagent chemotherapy combinations, with or without radiotherapy (RT), during the past 50 years, HL has been transformed from a highly fatal to a highly curable disease.6,7 Further to targeting neoplastic cells, the nontumoral microenvironment also provides important therapeutic targets with clinical implications.
Summary of current first-line therapy in cHL
In localized stages without adverse prognostic factors (early stages), brief courses (two to three cycles) of adriamycin, bleomycin, vinblastine and dacarbazine (ABVD) chemotherapy followed by involved-field or involved-node radiotherapy (IFRT, INRT) produce very satisfactory results,8–11 with indicative 10-year progression-free survival (PFS) and 10-year overall survival (OS) rates of 87% and 94%, respectively. 10 The results are also satisfactory in localized stages with risk factors (intermediate stages) with four cycles of ABVD plus IF(IN)-RT,11–14 with PFS and OS of at least 83% and 91% at 10 years, respectively.10,14 Intensification with two cycles of BEACOPP-escalated plus ABVDx2 and RT improves disease control, but not OS. 13 Early response assessment with positron emission tomography (PET) after two ABVD cycles (interim PET; iPET) may permit the omission of RT, and probably reduces long-term toxicity in patients with a strictly negative iPET, defined by the 2007 International Harmonization Project criteria and roughly corresponding to a Deauville 5-point scale (D5PS) score of 1 or 2. Omission of RT is associated with minimal compromise in disease control and no detrimental effect on OS, especially in intermediate stages treated solely with six ABVD cycles. 15 In early favorable stages (or nonbulky IA/IIA), the 5-year PFS after two, three, or four cycles of ABVD alone was approximately 86%, 87% and 90%, respectively.15–17 Similar results were reported in real-life by the British Columbia group. 18 Furthermore, 12–25% of patients who remain iPET-positive after ABVDx2 may enjoy better disease control, and probably increased survival, with the addition of two cycles of BEACOPP-escalated instead of two ABVD cycles prior to RT.9,15,18 However, it appears that this benefit is restricted largely to the subset of iPET-positive patients who have more intense uptake with D5PS 4-5. 19
In advanced stages, six to eight cycles of ABVD plus RT in a selected minority of patients can produce 10-year PFS rates of 65–75% and a 10-year OS exceeding 80%.20–27 The current trend is to adopt six cycles of ABVD, especially in the PET era. The German Hodgkin Study Group (GHSG) standard of care is six cycles of BEACOPP-escalated, which has produced better results (disease control and OS 84% and 90% at 10 years) and minimized the use of RT at the expense of higher toxicity.28–31 The introduction of iPET in order to avoid bleomycin in case of negative results (defined as D5PS 1-3) and switch to BEACOPP-escalated only in the minority of patients who remain PET-positive (D5PS 4-5) after ABVDx2, may improve the outcome of fixed ABVD chemotherapy.24,32–34 Indeed, the omission of bleomycin after two cycles of ABVD in early unfavorable and advanced HL in the RATHL trial was not inferior to the continuation with full ABVD for six cycles in total. 32 However, the negative predictive value of iPET after ABVDx2 appears to be suboptimal.24,35,36 The reverse strategy, which starts with two cycles of BEACOPP-escalated and step down to ABVDx4, or only two further cycles of BEACOPP-escalated, keeping the whole six cycles only for iPET positive patients (defined here as D5PS 3-5), appears also highly effective.37–39
Recently, the introduction of brentuximab vedotin (BV) in combination with AVD, thus replacing bleomycin, was shown to improve disease control in stage III/IV cHL with minimization of lung toxicity. In the whole patient population, the 2-year modified PFS per the Independent Review Committee (IRC) was 82.1% versus 77.2% for BV-AVD and ABVD, respectively (hazard ratio 0.77, p = 0.03), 40 and the benefit appeared to be durable in the 3-year follow-up report. 41 Interestingly, increases in modified PFS by 7–9% with a ~4% increase in short-term OS were observed in high-risk subgroups, such as stage IV or any, and particularly multiple, extranodal involvement. 42 Following United States Food and Drug Administration (FDA) approval of BV-AVD for advanced cHL, and based on the above data on preplanned subgroup analyses, the European Medicines Agency (EMA) also approved the combination of BV-AVD for patients with stage IV cHL.40,42,43 Further to incorporation into the AVD regimen, the GHSG has also evaluated the incorporation of BV into a BEACOPP backbone. Among the BrECAPP and BrECADD regimens (BV, etoposide, cyclophosphamide, doxorubicin and procarbazine/predinisone or dacarbazine/dexamethasone), the latter was considered equally effective and less toxic in a randomised phase II trial. 44 Thus, BrECADD was selected to be compared with the GHSG standard of care of six cycles of BEACOPP-escalated in the HD21 trial for advanced cHL. 45
Despite these exciting results, 20–30% of patients will progress or relapse within 10 years of ABVD-based strategies, while this figure will be clearly lower with iPET- and BEACOPP-based strategies. In addition, recent data show that patients who remain in remission after 5 years from diagnosis have an almost linear incidence of very late relapses for at least an additional 20 years.46–48 Thus, a considerable proportion of patients will develop relapsed/refractory cHL (rr-cHL) and require second-line salvage therapy, which will be curative in roughly half of them.
This review will focus on second and subsequent lines of therapy for rr-cHL, the strategies that might improve the efficacy of second-line therapy and the optimal integration of novel agents and high-dose therapy (HDT) with autologous (autoSCT) or allogeneic stem-cell transplantation (alloSCT) in the treatment algorithm.
Second-line therapy for classical Hodgkin lymphoma
Following frontline treatment failure, the majority of patients with rr-cHL require systemic treatment. Local/regional salvage RT can cure a minority of patients, who experience asymptomatic, localised relapse outside the previous RT field, especially if relapse occurs >1 year after the end of treatment.49–52 Among the vast majority of patients requiring systemic therapy, most are eligible for intensive salvage chemotherapy with HDT and autoSCT. However, a minority, those aged >65–70 years or with serious comorbidities as well as the rare poor mobilizers, are not candidates for autoSCT. These patients are treated with second-line, usually noncross-resistant regimens, but generally have a poor prognosis when treated with conventional chemotherapy.53,54
Patients with relapsed/refractory classical Hodgkin lymphoma eligible for autoSCT
Standard salvage therapy and prognostic factors
Chemotherapy options. Based on the results of two randomized trials, HDT/autoSCT is considered the standard of care for eligible patients with rr-cHL who remain chemosensitive to second-line regimens.51,55 HDT/autoSCT is also the standard of care for chemorefractory patients with stable disease (SD),56,57 but second-line salvage chemotherapy is almost futile in patients with progressive disease (PD). Platinum or gemcitabine-based regimens are usually administered as salvage therapy with the aim to assess chemosensitivity, achieve an acceptable remission status, and mobilise and collect peripheral blood stem-cells. Although many regimens have been evaluated in this setting (Table 1), IGEV (ifosfamide, gemcitabine, vinorelbine, prednisone), ESHAP (etoposide, methylprednisolone, high-dose cytarabine, cisplatin), DHAP (dexamethasone, high-dose cytarabine, cisplatin), ICE (ifosfamide, carboplatin, etoposide), GDP (gemcitabine, dexamethasone, cisplatin), GVD (gemcitabine, vinorelbine, dexamethasone) or similar regimens are the most commonly used, while mini-BEAM (carmustine, etoposide, cytarabine, melphalan) and Dexa-BEAM (dexamethasone-BEAM) are much less popular because of excessive toxicity.51,55,58–72
Conventional salvage regimens in relapsed/refractory Hodgkin lymphoma.

ASHAP, (adriamycin, solumedrol, high-dose cytarabine, cisplatin); CR, complete response; Dexa-BEAM, dexamethasone-BEAM; DHAP, (dexamethasone, high-dose cytarabine, cisplatin); DFS, disease-free survival; EFS, event-free survival; ESHAP, (etoposide, methylprednisolone, high-dose cytarabine, cisplatin); FF2F, freedom from second failure; FFTF, freedom from treatment failure; GDP, (gemcitabine, dexamethasone, cisplatin); GEM-P, cisplatin and methylprednisolone; ICE, (ifosfamide, carboplatin, etoposide); IGEV, (ifosfamide, gemcitabine, vinorelbine, prednisone); mini-BEAM, (carmustine, etoposide, cytarabine, melphalan); NR, not reported; OS, overall survival; OR, overall response; PBSC, peripheral blood stem cell; pts, patients; PFS, progression-free survival.
Although the actual dose intensity of DHAP may affect prognosis, 73 further treatment intensification with the addition of alternating higher-dose cytotoxic agents between salvage therapy with DHAP and HDT did not improve the outcome of HDT/autoSCT. 62 In clinical practice, we prefer IGEV because of less myelotoxicity and an excellent mobilisation potential, but any of the above regimens is equally acceptable, since no proven superiority has been demonstrated over the others. The results of these salvage regimens are shown in Table 1 and suggest that a considerable percentage of patients with rrHL, up to 30%, will not be directly eligible for HDT/autoSCT after second-line salvage therapy due to the lack of chemosensitivity. Furthermore, the percentages of complete response (CR) to conventional second-line salvage therapy are rather low.
Who is eligible for autoSCT: conventional or functional imaging? In addition to chemosensitivity evaluated by conventional restaging, PET/CT after salvage therapy is also a powerful prognostic factor for the outcome of autoSCT. Patients with a negative PET following salvage therapy have very good outcomes, at least in the short term, with relapse rates generally not exceeding 15–30%.74–85 Patients who remain PET-positive have significantly inferior prognosis; however, they still have a 25–40% chance of cure, especially if they do not have PD based on conventional restaging criteria.74–85 Therefore, autoSCT should not be omitted or withheld based solely on the persistence of metabolically active disease. In addition to PET-based response to salvage therapy, the baseline FDG-PET metabolic tumor volume prior to salvage therapy can provide independent prognostic information.77,78
A major question is whether PET-positive, but conventionally responding, patients should be forwarded to HDT/autoSCT, or if further effort to achieve PET negativity should be made. Moskowitz and colleagues showed that, if a PET-negative status is achieved by a second salvage regimen (3rd-line treatment), the outcome of HDT/autoSCT is equally good with cases who directly achieve PET negativity with the first salvage regimen. However, it is not clear whether the effort to achieve PET-negativity with 3rd-line therapy is beneficial per se or whether it is just a means of selecting patients with a higher chance of cure after HDT/autoSCT. 79 Further to the pretransplant PET, it appears that the majority of the patients who are ultimately cured, are those who remain PET-negative or convert to PET-negative at 3 months after autoSCT. 85
Summarising, chemosensitive patients based on conventional imaging, and those with SD after salvage therapy, can be forwarded to HDT/autoSCT, while those with PD have a very low chance of benefitting from the procedure. Further handling of PET-positive patients without conventionally defined PD depends on the practice of each centre. Both immediate transplant and further salvage to improve remission status are acceptable. D5PS grading may predict prognosis and facilitate treatment decisions but needs prospective evaluation. However, with the potential incorporation of novel agents in earlier treatment lines in the near future, the main goal of salvage therapy will be PET negativity prior to HDT/autoSCT.
Prognostic factors. Further to PET status prior to autoSCT, many other prognostic factors have been reported to affect the outcome of HDT/autoSCT. 86 Recently, the RisPACT consortium evaluated potential risk factors for the outcome of autoSCT in 546 patients. In multivariate analysis, CR duration ⩽3 months, stage IV, a nodal lesion >5 cm, Eastern Cooperative Oncology Group performance status (ECOG PS) ⩾1 and inadequate response to salvage therapy prior to autoSCT assessed by CT or PET, were independent predictors for PFS. 87
Optimizing second-line therapy in relapsed/refractory classical Hodgkin lymphoma
More effective salvage regimens and incorporation of novel agents into second-line salvage regimens might improve either the proportion of patients who can be forwarded to HDT/autoSCT, or even the outcome of autoSCT, by increasing response rates and the depth of remission. In chemorefractory patients, who are not eligible for autoSCT, novel agents may induce responses and allow a potentially curative transplant. Finally, consolidation strategies after autoSCT might be optimized in terms of either patient selection or evaluation of other novel agents.
New conventional salvage chemotherapy regimens. Bendamustine monotherapy is active in rr-cHL following autoSCT or ineligible for the procedure, with overall response rates (ORR) 50–60% and CR rates of ~30%, but very few patients remain progression-free at 2 years.88–90 Bendamustine is also active after both autoSCT and BV failure,91–93 and can serve as a bridge to alloSCT.91,92 More recently, the BeGEV (bendamustine, gemcitabine, vinorelbine) combination was studied as second-line treatment with very promising outcomes: the ORR was 83% with 73% CRs; 97% of patients underwent successful stem-cell collection. On an intention-to-treat basis, the transplant rate was 73%. The 2-year PFS and OS rates were 80.8% and 89.3%, respectively, for those patients who proceeded to autoSCT, making this combination a very promising approach. 94
Finally, GemOx (gemcitabine, oxaliplatin) is a novel combination for rr-HL, 95 which may be active both in the setting of platinum-based salvage therapy and after autoSCT failure. 96
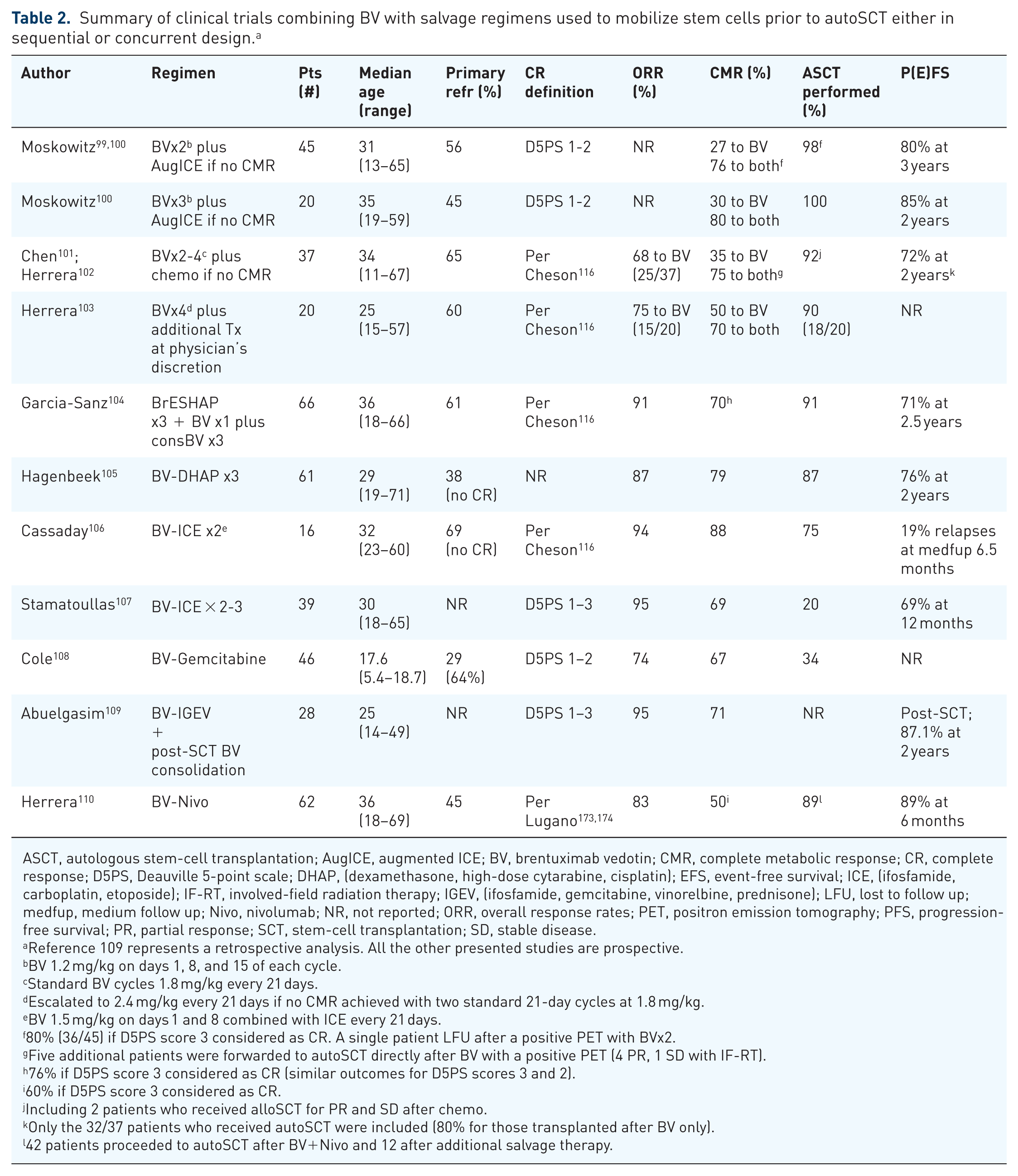
Incorporation of novel agents in second-line salvage therapy. This strategy is currently restricted to the incorporation of BV in second-line strategies, as summarized in Table 2.99–110 Other combinations, such as bortezomib-ICE, panobinostat-ICE and bortezomib-IGEV, were evaluated but were not further developed, with both bortezomib-based combinations failing to prove superior to the corresponding conventional regimens in randomised phase II trials.76,97,98
Summary of clinical trials combining BV with salvage regimens used to mobilize stem cells prior to autoSCT either in sequential or concurrent design. a
ASCT, autologous stem-cell transplantation; AugICE, augmented ICE; BV, brentuximab vedotin; CMR, complete metabolic response; CR, complete response; D5PS, Deauville 5-point scale; DHAP, (dexamethasone, high-dose cytarabine, cisplatin); EFS, event-free survival; ICE, (ifosfamide, carboplatin, etoposide); IF-RT, involved-field radiation therapy; IGEV, (ifosfamide, gemcitabine, vinorelbine, prednisone); LFU, lost to follow up; medfup, medium follow up; Nivo, nivolumab; NR, not reported; ORR, overall response rates; PET, positron emission tomography; PFS, progression-free survival; PR, partial response; SCT, stem-cell transplantation; SD, stable disease.
Reference 109 represents a retrospective analysis. All the other presented studies are prospective.
BV 1.2 mg/kg on days 1, 8, and 15 of each cycle.
Standard BV cycles 1.8 mg/kg every 21 days.
Escalated to 2.4 mg/kg every 21 days if no CMR achieved with two standard 21-day cycles at 1.8 mg/kg.
BV 1.5 mg/kg on days 1 and 8 combined with ICE every 21 days.
80% (36/45) if D5PS score 3 considered as CR. A single patient LFU after a positive PET with BVx2.
Five additional patients were forwarded to autoSCT directly after BV with a positive PET (4 PR, 1 SD with IF-RT).
76% if D5PS score 3 considered as CR (similar outcomes for D5PS scores 3 and 2).
60% if D5PS score 3 considered as CR.
Including 2 patients who received alloSCT for PR and SD after chemo.
Only the 32/37 patients who received autoSCT were included (80% for those transplanted after BV only).
42 patients proceeded to autoSCT after BV+Nivo and 12 after additional salvage therapy.
Two approaches have been adopted with BV given either sequentially or concurrently with established salvage regimens.99–107,111–115 All but one of the phase II trials of BV plus conventional chemotherapy included notably similar numbers of patients, ranging from 57 to 65.99–105 Sequential strategies include BV induction, either as two cycles of dose-dense weekly 1.2 mg/kg BV infusions on days 1, 8, and 15, every 28 days,99,100 or two to four standard dose 1.8 mg/kg BV infusions every 3 weeks.101–103 If metabolic CR was not achieved in these studies, patients received either augmented ICE,99,100 or various established salvage regimens.101–103 Concurrent strategies included the combination of BV with ESHAP (BrESHAP), 104 DHAP (BV-DHAP),105,113 or ICE.106,107 In all studies, PET-based rather than conventional response criteria were used.116,117 BV has also been combined with gemcitabine, nivolumab, or bendamustine, as will be analyzed later.108,110,114,115 In a recent retrospective trial, the combination of BV with IGEV in rr-cHL patients (half of them receiving it as a subsequent salvage line) led to a more favorable SCT outcome by improving metabolic status prior to SCT in this high-risk clinical setting. 109
The results of all phase II trials of BV plus sequential or concurrent established salvage regimens are summarized in Table 2. Almost all these trials provided high metabolic CR rates, typically 70–80%, which appear higher than those achieved with the corresponding salvage regimens without BV.99–105 In addition, minimizing the incidence of PD, they reproducibly demonstrated high SCT rates, with 87–100% of the patients ultimately undergoing autoSCT, which also appears clearly better than the rates achieved with conventional salvage therapy.99–105 In intention-to-treat analyses, the 2- or 3-year PFS rates were >70% and up to 80%, respectively.99–106
The sequential strategies also demonstrated that a brief BV monotherapy can induce metabolic CRs in 25–35% of rr-cHL as second-line therapy, thus enabling HDT/autoSCT without further chemotherapy and that the outcome of these autoSCTs is favorable.99–103,111,112 Furthermore, it was demonstrated that an additional third dose-dense BV cycle, 100 or BV dose escalation to 2.4 mg/kg after the second standard-dose 3-weekly BV infusion,102,103 are not the way to increase the metabolic CR rate.
Besides the obvious superiority of sequential and concurrent BV-salvage combinations over the corresponding conventional salvage regimens, some limitations should be kept under consideration. The CR rates should be compared with caution (Tables 1 and 2) because PET-based 116 and conventional criteria 117 have been generally applied in different time periods, so that figures may not be comparable. Furthermore, BV-chemotherapy combinations have been evaluated in moderately-sized studies and have not been directly compared with the corresponding traditional salvage regimens, while they have demonstrated relatively higher rates of grade 3–4 hematologic toxicity.
BV has also been evaluated in combination with bendamustine in rr-cHL, although HDT/auto-SCT was not intended for all patients. In a single-center phase I/II trial, LaCasce et al. assessed the efficacy and toxicity of BV 1.8 mg/kg on day 1 plus bendamustine 90 mg/m2 on days 1 and 2 of 3-week cycles for up to 6 cycles. Among 55 patients, 53 were evaluable for response: The metabolic ORR was 92% with 74% CRs and response rates were better for relapsed than primary refractory disease; only 1/53 patients had PD. Ultimately, 77% of patients without PD proceeded to HDT/auto-SCT and 60% also received consolidation with BV up to 16 infusions in total. At a median follow-up of 23 months after auto-SCT, the estimated 2-year PFS and OS were 63% and 94% overall and 70% and 95% for the transplanted patients, many of whom had not age- or comorbidity-related restrictions. Unexpectedly, severe infusion-related reactions (IRRs) were frequently observed. Stem-cell collection was adequate, despite concerns regarding potential detrimental effects of bendamustine. 114 More recently, an international, multicenter phase I/II trial of 68 heavily pretreated rr-HL patients confirmed the applicability of the above dosing regimen 114 to more extensively pretreated patients, who had received a median of 3 prior regimens (range; 1-8)including autoSCT in 57%. 115 Among the 37 patients, who received the optimal dose at the phase II portion, the ORR was 78% and the CR rate 43%. The 2-year PFS and OS exceeded 60% and 80% respectively. Both the latter studies suggest that BV-bendamustine could potentially replace platinum- or gemcitabine-based chemotherapy before autoSCT in transplant-eligible patients as an alternative, less (or equally) toxic regimen, given on an outpatient basis. Finally, Cole et al. evaluated the combination of BV with gemcitabine in young adults (⩽30 years-old) with primary refractory or early relapsing disease in a single-arm phase I/II trial. The CR rate (Deauville 1-2 on FDG-PET scan) reached 57% allowing a successful and rapid reference to HDT/SCT consolidation. 108
In the same context, Herrera et al. introduced an almost chemo-free approach, in which BV was combined with the Programmed Death-1 (PD-1) inhibitor nivolumab in the setting of second-line treatment of 62 patients with rr-cHL prior to any further chemotherapy (Table 2). On cycle 1, 1.8 mg/kg BV was administered on day 1 and 3 mg/kg nivolumab on day 8, while for the remaining cycles, 2–4, both agents were given on day 1 at the same doses. Among 60 evaluable patients, the ORR was 84% and the CR rate 62%, with 48% of CR patients achieving a D5PS score ⩽2. Only 8% of patients developed PD. Among 60 patients, 54 (90%) were forwarded to HDC/autoSCT, although 12 did so after additional chemotherapy. Post-autoSCT, nine patients received consolidation with RT, BV, or pembrolizumab (three cases each). The 15-month PFS rate was 82%. Similar results were seen in an additional series of 30 patients who received BV and nivolumab concurrently on day 1 (ORR 93%, CR 80%; 29 proceeded to auto-SCT, 25/29 directly).110,118 As a result, the BV-nivolumab combination appears as a chemo-free, potent salvage therapy for rr-cHL patients prior to autoSCT, which can be given on an outpatient basis. A further advantage is that high-cost novel agents are given for a short time period only.
The concept of chemo-free approach incorporating BV and checkpoint inhibitors has also been adopted in patients heavily pretreated with cHL. Diefenbach and colleagues evaluated the combination of nivolumab and BV in 19 heavily pretreated HL patients, with a median of 3 prior therapies, including SCT and BV. The combination was generally well-tolerated, while the ORR and CR rate reached 89 and 50%, respectively. 119 Furthermore, BV has been combined with ipilimumab, 120 or both nivolumab-ipilimumab.121–123 In the recent extended follow-up report, the triplet combination demonstrated higher CR rates and potentially more durable response rates than any doublet combination, at the expense of 8.2% incidence of dose-limiting toxicity as well as deaths secondary to pneumonitis in the nivolumab-containing combinations. 123
Bridging autoSCT with novel agents in chemorefractory patients. Although the potential future incorporation of BV into second-line regimens may change the clinical landscape, as described above, a considerable proportion of patients are chemorefractory; in particular, those with PD are not deemed eligible for autoSCT with the currently approved conventional salvage regimens. Prior to performing a ‘desperate’ auto-SCT, many physicians try to get a better response with additional chemotherapy.
BV has been evaluated in this setting in retrospective studies. 124 In a UK-wide retrospective study, 99 patients with a median age of 32 years (range 13–70) received BV as further salvage after two (70%), three (24%) or four (5%) previous lines of treatment. 125 The outcome of 2nd-line salvage, mainly with platinum- or gemcitabine-based regimens, typically was PD, SD, or PR/partial metabolic response, although 10% of the patients had achieved a CR. The ORR to BV was 56%, with 29% CR/CRu or metabolic CR, and was similar irrespective of the extent of previous treatment. Approximately one-third of patients proceeded directly to auto- or alloSCT; almost all of them had responded, and two-thirds had achieved a CR on BV. An additional 27% did so after further chemotherapy, while 39% failed to undergo SCT, and received only further chemotherapy or no further treatment. Of the 38 latter patients, 10 had actually responded to BV, but the responses were partial and short-lived. The median PFS for the whole population was 5.6 months and the median OS 37.2 months, but was not reached for SCT-treated patients, being similar for those who underwent SCT directly after BV or following further chemotherapy.
The published experience of other groups demonstrates rates of ‘immediate’ SCT ranging from 34% to 47% in all studies but one, thus confirming that BV can overcome chemoresistance and permit a viable SCT in a sizeable proportion of patients ineligible for autoSCT due to being chemorefractory or inadequate response to chemotherapy, as judged by the treating physician.124–129
Consolidation after autoSCT in high-risk patients
Once autoSCT has been performed, the risk of further relapse/progression can be as high as 50%.130–132 The AETHERA trial demonstrated that disease control can be improved with 16 infusions of BV over placebo every 3 weeks, started 30–45 days after autoSCT, in patients who are deemed to be at high risk of relapse, as reflected by the presence of primary refractory disease or early (<1 year) or extranodal relapse. Based on the analysis of 329 patients, AETHERA met its primary endpoint, with a hazard ratio of 0.57 (95% CI 0.40–0.81; p = 0.0013) for PFS per the Independent Review Committee. 56 In the 5-year follow-up report, the 5-year PFS for BV versus placebo was 59% versus 41% per investigator assessment [hazard ratio 0.52 (95% CI 0.38–0.72)]. 57 Although the formal OS analysis is planned for 2020, the 3-year OS rate exceeded 80%, comparing favorably with historical survival data for high-risk HL patients undergoing autoSCT. However, OS was the same in both arms of AETHERA, with the curves being completely superimposable, probably reflecting the widespread use of BV in 87% of the relapsed patients in the placebo arm upon further progression. Based on AETHERA, BV was approved as consolidation therapy for patients with cHL who have undergone ASCT and are deemed to be at increased risk of relapse. Interestingly, the time to second subsequent therapy was improved by BV: at 5 years, 36% of patients allocated to the BV arm had received at least two subsequent lines of therapy versus 46% in the placebo arm [hazard ratio 0.66 (95% CI 0.47–0.92)]. The use of subsequent alloSCT was similarly decreased in the BV arm (12% versus 21%).
When five potential risk factors were considered, namely initial remission duration <1 year, <CR to most recent salvage therapy, extranodal disease at the time of salvage therapy, B symptoms at the time of salvage and >1 salvage regimen required to achieve chemosensitive disease, hazard ratios for PFS were much lower in favor of BV in patients with at least two or at least three risk factors (0.42 and 0.39, respectively) without any effect on OS.56,57 Along these lines, it appears that patients with worse characteristics obtain greater PFS benefit from BV consolidation. Similarly, BV consolidation produced a significant PFS benefit for patients who remained PET positive after salvage therapy, but not for PET-negative patients. However, these data should be interpreted with caution, because AETHERA was designed prior to the widespread use of pretransplant PET; thus almost one-third of the patients did not undergo PET evaluation, which was not mandatory by the protocol, while predefined criteria for PET positivity were not established. 56
In the increasingly prevalent setting that patients have been forwarded to autoSCT with the use of BV due to being chemorefractive, it appears sensible to administer BV consolidation; however, fewer cycles could be considered (for example ⩽10) in order to avoid cumulative toxicity, especially peripheral neuropathy. 111
Further to the already approved indication of BV consolidation after autoSCT in high-risk patients, other studies are currently investigating consolidation strategies in HL. The trial of panobinostat consolidation was closed prematurely due to low accrual rate. For this reason, efficacy was not formally evaluated, but 29% of patients discontinued due to PD from the placebo arm versus 11% in the panobinostat arm. 133 Pembrolizumab 200 mg IV every 3 weeks for up to eight cycles is being tested in a phase II trial as consolidation of auto-SCT in high-risk rr-cHL patients post-ASCT after two to three lines of therapy. At 1.5 years, PFS and OS were 78% and 100%, respectively, for the 30 evaluable patients. 134
Patients with relapsed/refractory classical Hodgkin lymphoma are ineligible for autoSCT due to age or comorbidities
Standard salvage therapy and prognostic factors
A small minority of younger, fit patients with asymptomatic, nodal-only relapse outside any previous RT field may not be treated with salvage chemotherapy and autoSCT, because they are potentially curable with salvage RT only. 49 However, a sizeable minority of patients with rr-cHL includes those who are not candidates for autoSCT, either due to their advanced age, or due to the presence of comorbidities or poor performance status. Unfortunately, there are no formal guidelines for the therapeutic approach of such patients, and the results of conventional salvage therapy for elderly patients with rrHL are rather disappointing.53,54 As a result, those patients who are ineligible for aggressive chemotherapy followed by HDC/autoSCT, should be treated with the aim of preserving a fragile balance between disease control and therapy-related toxicity. Treatment options for this sensitive population include noncross-resistant chemotherapy, such as ChlVPP (chlorambucil, vinblastine, procarbazine, prednisone) or MOPP (mechlorethamine, vincristine, procarbazine, prednisone), GVD, gemcitabine-vinorelbine, single-agent bendamustine (off-label), or even GDP, similarly to patients with rrHL after autoSCT failure as described below. 135
Optimizing second-line therapy in rrHL ineligible for autoSCT
The novel agent monotherapy (BV, nivolumab, pembrolizumab) has not been approved as second-line therapy but might be applicable as an off-label option, as also would be BV-bendamustine. 136 In the BV-bendamustine trial published by LaCasce and colleagues, patients who were not forwarded to autoSCT had acceptable outcomes. Although many of them were not ‘ineligible for SCT’, the BV-bendamustine combination can be a viable second-line option in this population as well. 114
Third-line therapy and beyond
Approximately 50% of rr-cHL patients undergoing autoSCT will experience further disease progression or relapse following current salvage regimens.130,137 The outlook of these patients is very poor, with an estimated median OS of 2–3 years.138–144 In addition, the expected outcome of transplant-ineligible patients, either young but chemorefractory, or elderly, or those with significant comorbidities after 2nd-line failure, is probably even worse. With the availability of BV and checkpoint inhibitors in the above distinct clinical settings where third- or subsequent-line therapy is required, treatment strategies have become similar, though the goal (palliative or curative) differs considerably.
Until recently, the management of patients who failed HDT/autoSCT was largely empirical due to the lack of effective therapeutic options and the absence of prospective clinical trials.141–143 Historically, additional chemotherapy used to be the commonly acceptable practice for relapse after autoSCT, aiming to induce remission. In this setting, eligible chemosensitive patients could receive consolidation with reduced intensity conditioning (RIC) alloSCT (see below).143,145–148 Nevertheless, a significant proportion of patients is not eligible for allo-SCT due to chemoresistant disease, lack of matched donor availability or poor performance status/comorbidities. In the era of BV and checkpoint inhibitors (nivolumab and pembrolizumab) the role of RIC-alloSCT in HL has become a matter of debate among lymphoma physicians, as discussed at the end of this review.
Brentuximab vedotin as salvage therapy for relapsed/refractory classical Hodgkin lymphoma
Brentuximab vedotin in autoSCT failures
In 2011 and 2012, respectively, BV was approved by the FDA and EMA for either patients with relapsed cHL after autoSCT or those after at least two prior chemotherapy regimens who are not candidates for autoSCT (‘when autoSCT or multiagent chemotherapy is not an option’ according to EMA). In the pivotal phase II study, 102 patients were treated with single-agent BV 1.8 mg/kg every 3 weeks for maximum of 16 cycles. 149 All patients had failed autoSCT, they had received a median of 3.5 prior regimens (up to 13), and 71% had primary refractory disease, all of which underline the marked single-agent activity of BV. The ORR was 75%, with a CR rate of 34% according to the PET-based International Harmonization Project (IHP) criteria.116,150 The median PFS was 9.3 months, with a 5-year rate of 22%, but it was much more prolonged (not reached with prolonged follow up) for those patients who achieved CR.151,152 Remarkably, PFS rates were not significantly different between CR patients who underwent alloSCT and those who did not. Recently, data on the 5-year study outcomes revealed that the estimated PFS and OS rates were 52% and 64%, respectively, for patients in CR. 152 Interestingly, 9/102 patients in the pivotal trial entered a >5-year disease-free status without additional chemotherapy or alloSCT after achievement of CR with BV post-autoSCT. 152 These results point to the potential curative role of BV in a small minority of patients with rr-cHL postauto-SCT failure.
BV retreatment has also shown significant efficacy, with 60% ORR (30% CR) in patients who had already received BV as salvage therapy, had achieved CR/PR but had withdrawn treatment prior to its completion, and had experienced further disease progression. The median duration of response (DOR) to retreatment was 9.2 months. 153
A pivotal study suggested that BV was effective after autoSCT failure in patient subgroups defined by disease status (relapsed or refractory), number of prior therapies, age, or disease bulk. 149 However, the exact determinants of response to BV in real life require further evaluation. For example, ORR may be inferior for patients ineligible for autoSCT due to their being chemorefractory, or for those who receive BV after further intervention following autoSCT, who may be more refractory to chemotherapy.124,126,154 These prognostic factors, as well as symptomatic or bulky disease at BV initiation, may be relevant and deserve further consideration. 124
Real-life data are consistent with the pivotal phase II trial of BV, especially considering that all these studies included not only autoSCT failures but also transplant-naïve patients, who may be even more chemorefractory.124,126,128,129,154–156 Interestingly, an Italian observational study of 234 patients confirmed that a small minority of patients (~5%) may achieve durable responses and potential cure with BV only and no additional consolidative therapy. 126
Although the potential effect of BV on the OS of patients who have failed autoSCT cannot be strictly estimated in the absence of randomized trials, it appears that an OS benefit has probably been achieved.157,158 OS rates in the BV era appear better than prior to its introduction, and this persists when only the ‘worst-case scenario’ is taken into account. 158
Brentuximab vedotin as a bridge to autoSCT after inadequate response to salvage therapy
This topic has already been discussed above in the section ‘Bridging autoSCT with novel agents in chemorefractory patients’.
Brentuximab vedotin as beyond 3rd-line salvage in patients ineligible for autoSCT
In 2017, Brockelman and colleagues published the combined German and British experience on the use of BV in autoSCT-ineligible patients due to advanced age and comorbidities. 159 A total of 136 patients with a mean age of 66.7 years received BV following at least 2 lines of therapy (116/136 patients), after being considered ineligible for autoSCT due to comorbidities (74%), age restrictions (57%), patient’s choice (15%), refractoriness to treatment (12%), or mobilization failure (3%). Notably, ECOG PS was ⩾2 in 61% of the patients. ORR was almost identical to the pivotal BV trial after autoSCT failure: ORR was 74% and CRs 35%. The median PFS was 15.1 months, without, however, reaching a plateau, while the median OS was 17.8 months. Among 51 deaths, only 33 were attributed to the disease. Thus, BV monotherapy may induce responses of considerable duration in many patients who fall into a highly unfavorable disease category.
Brentuximab vedotin in special subpopulations
In case of liver impairment, the dose of BV should be reduced to 1.2 mg/kg every 3 weeks. There are few case reports demonstrating the potential for an uneventful use of BV in patients with severely compromised liver function due to HL, in which jaundice was reversed, although the duration of the benefit was brief.160,161 The reversal of jaundice in previously untreated patients with cHL who present with this complication appears also safe and much more successful. 162 In case of severe bone marrow failure, BV may promptly reverse the blood counts, although a more pronounced hematologic toxicity is possible. 161
Checkpoint inhibitors as salvage therapy for relapsed/refractory classical Hodgkin lymphoma following brentuximab vedotin failure
Following both autoSCT and BV failure, the expected outcome of the patients becomes even worse. Only alloSCT could be a viable curative option, but is ultimately applicable only in a minority of patients. 163 Prior to the introduction of checkpoint inhibitors, treatment options were limited to additional chemotherapy regimens or experimental agents with a median PFS of 3.5 months and a short median OS. 163
Nivolumab and pembrolizumab are well-established checkpoint inhibitors. Nivolumab is a human IgG4, while pembrolizumab is a humanized IgG4 monoclonal antibody, both directed against the PD-1 molecule, which is present on the surface of T-cells. Through the inhibition of the PD-1/PDL-1 pathway, these agents potentiate T-cell activity against the neoplastic cells. Sintilimab and tislelizumab are PD-1 inhibitors developed later in China, and will also be analyzed below.
Results of major clinical trials of checkpoint inhibitors
Phase I trials of the checkpoint inhibitors nivolumab and pembrolizumab, the CA209-039 and KEYNOTE-13 studies, were based on 23 and 31 heavily pretreated patients, respectively, and produced impressive results with acceptable toxicity, thus revolutionizing the field of rr-cHL.164,165 Patient populations were rather heterogenous in terms of previous BV and autoSCT treatment. Both studies, published 4.5 and 3 years ago, are already of rather historical significance, since the mid-term results of Checkmate 205 and KEYNOTE-087, the much larger phase II trials of nivolumab and pembrolizumab, respectively, are now available.166–171
Nivolumab was further developed in patients with cHL after autoSCT failure in the four-arm Checkmate 205 trial. Arm D explored the possibility of integrating nivolumab into the AVD regimen as first-line treatment, which is outside the scope of this review. Arms A, B, and C recruited 243 patients with rrcHL who had failed autoSCT. In all three arms, nivolumab was given at a dose of 3 mg/kg every 2 weeks until disease progression or unacceptable toxicity. 166 Later, outside this trial, the approved dose for nivolumab was modified to 240 mg fixed dose every 2 weeks. 172 Arm B (n = 80) was the basis for regulatory approval of nivolumab for the treatment of patients who have failed both autoSCT and BV. 169 Arm A included 63 patients who had failed autoSCT but had not been exposed to BV, while arm C included 100 patients who had failed both ASCT and BV, which could have been given after ASCT (n = 58), prior to ASCT (n = 33), or both (n = 9). The unique feature of arm C was that nivolumab was stopped in patients who entered a sustained CR for 1 year, and could be resumed in case of relapse within 2 years of the last dose. As expected for patients having failed autoSCT, elderly patients (⩾60 years old) were very rarely enrolled, representing only 6% of the total study population. Furthermore, enrollment was restricted to patients with ECOG PS 0-1. Interestingly, an early protocol amendment permitted nivolumab to be continued after the occurrence of investigator-assessed disease progression if prespecified criteria were met (see below). Overall, the response rate to nivolumab was 69% with 16% CRs according to an IRC versus 72% and 33%, when responses were assessed by the investigators. 166 ORRs appeared similar for arms A, B, and C (65%, 68%, and 73%), but the CR rates were better in the less heavily pretreated Arm A (25% versus 13% and 12%, respectively). After a minimum follow up of 31 months, 20% of the patients were still on treatment. 171 Overall, the median DOR was 18 months, significantly longer in patients with CR as their best response compared with PR (32 versus 13 months). The median PFS per IRC was 15 months, again longer in Arm A (17 months versus 12 and 15, respectively). The median time to next treatment was 29 versus 27 versus 20 months for Arms A, B, and C, respectively. The 2-year OS was excellent at 90%, 86%, and 86%, respectively.
Pembrolizumab was further developed in patients with cHL in the 3-cohort Keynote-087 trial, which had major similarities, but also crucial differences from Checkmate 205. Interestingly, cohort 2 included 81 patients who were considered ineligible for autoSCT but had failed BV. Cohort 1 was identical to Arm B of Checkmate 205, including 69 patients who had failed both autoSCT and BV, while cohort 3 recruited 60 patients with rr-cHL who had failed ASCT, and had not received BV post-autoSCT, although 42% had been exposed to BV prior to transplant. 168 Notably, the dose of pembrolizumab was ~80% lower compared with Keynote-013: the drug was given at the fixed dose of 200 mg every 3 weeks, which is the currently approved scheme, instead of 10 mg/kg every 2 weeks, until disease progression, or intolerable toxicity, or investigator decision, or a maximum of 2 years. 168 Keynote-087 was the basis for the regulatory approval of pembrolizumab for the treatment of patients with rr-cHL in the circumstances described at the end of this section. Similarly to Checkmate 205, elderly patients were very rare, representing only 9% of the total study population (⩾65 years old), although the percentage was 18% in cohort 2. Enrollment was again restricted to patients with ECOG PS 0-1. Interestingly, continuation of pembrolizumab beyond the first assessment of disease progression was permitted if the patient was clinically stable, and both the investigator and the sponsor agreed. Overall, the ORR to pembrolizumab was 69%, with 22% CRs according to blinded independent central review (BICR) in the initial report (168); these figures increased to 72% and 28%, respectively, when best responses were taken into account at the 2-year report. 170 Best ORR and CR rates appeared similar for cohorts 1, 2, and 3 [77% (26%), 67% (26%) and 73% (32%), respectively]. 170 In the 2-year report, after a median follow-up of 27.6 months (maximum 32.9), the median PFS was 13.7 months, being shorter in cohort 2 of transplant-ineligible patients (and presumably more chemorefractory). Median PFS was 16.4, 11.1, and 19.4 months for cohorts 1, 2, and 3, respectively. Overall, the median DOR was 16.5 months (22.1, 11.1, 24.4 in cohorts 1, 2, and 3, respectively), being significantly longer in patients with CR as their best response compared with PR (not reached versus 10.9 months). 170 Interestingly, the application of Lugano 2014 response criteria was associated to a higher CR rate compared with Cheson 2007 values.116,173,174 In the most recent update of KEYNOTE-087, the 3-year OS was maintained at exceptionally high levels, reaching 86.4% in the total population (86.3%, 85.7%, 87.6% in cohorts 1, 2, and 3, respectively). Notably, pembrolizumab could be discontinued in patients attaining a CR, provided that they had received at least two doses after the documentation of CR, and had completed ⩾6 months of treatment. In this setting, 17 patients received a second course of pembrolizumab (up to 1 year administration, ~17 doses). The ORR to this second course was 68.8% with CR, PR, and SD rates being 31.3%, 37.5%, and 25.0%, respectively, although grade 3–4 treatment-related adverse event (AEs) occurred in 11.9% of patients. 175
More recently, two other PD-1 inhibitors, sintilimab and tislelizumab, were introduced and tested in Chinese Centers in the phase II trials ORIENT-1 for sintilimab 176 and BGB-A317-203 for tislelizumab, 177 including 92 and 70 patients, respectively. These trials included patients with rr-cHL who had failed at least two prior therapies. Although elderly patients were minimally represented, only 19% of the patients had undergone autoSCT in both trials, because the procedure is not affordable for many patients in China. Furthermore, only 6% had been exposed to BV in the ORIENT-1, and 21% had been exposed to ‘immunotherapy’ in the BGB-A317-203 trial, since BV lacked approval in China. Thus, these patient populations were less heavily pretreated compared with those in Checkmate 205 and Keynote-087. The ORR by IRC was 80% (CR 34%) in the ORIENT-1 and 86% (CR 61%) in the BGB-A317-203. At a median follow up of 10.5 months and 7.9 months, respectively, the 6-month PFS was 78% and 80%, which appears numerically similar to that achieved within the Checkmate 205 and Keynote-087 trials in rather worse patient populations. Toxicities were mild, and consistent with those of nivolumab and pembrolizumab (see below). Based on these data, sintilimab was approved in China, and will be tested in the western world. Further details on the Checkmate 205, Keynote-087, ORIENT-1, and BGB-A317-203 trials have been provided elsewhere. 178
In conclusion, the Checkmate 205 and Keynote-087 phase II trials confirmed the high response rates, which were almost equally applicable in the prespecified different clinical circumstances of rr-cHL in terms of BV and ASCT pretreatment, as well as the well-tolerated side effects of checkpoint inhibitors. Furthermore, the midterm results confirm that responses can be durable. After appropriate testing, sintilimab and tislelizumab might provide additional options for rr-cHL, raising cost issues, which are becoming increasingly significant.
Currently, the official indication for nivolumab is adult rr-cHL following failure of both autoSCT and BV both in FDA and EMA, although FDA has extended the approval to include patients with rr-cHL who have failed at least 3 lines of therapy, including autoSCT. According to EMA, the official indications for pembrolizumab include the treatment of adult patients with rr-cHL who have either failed both auto-SCT and BV, or have failed at least two regimens and BV, but are ineligible for autoSCT. However, the FDA has granted approval for patients with refractory HL, or who have relapsed after three or more lines of therapy, in both adult and pediatric populations. 178
Treatment with checkpoint inhibitors beyond conventionally defined progression
The unique mechanism of action of PD-1 inhibitors may permit the initial growth of the tumor. Immune activation, the basis of the therapeutic action of these drugs, may induce an early ‘inflammatory’ increase of already existing lesions, or the appearance of others that might not have been visible previously. Alternatively, a delayed tumor response may permit an early tumor growth with subsequent reduction, simulating early disease progression. 179 This should not be misinterpreted as treatment failure, and this is the reason for the development of another set of response criteria specifically designed for lymphomas.179,180 However, even after exclusion of such cases of transient tumor flare, several patients may experience disease progression by conventional or PET-based current definitions, but continue to gain clinical benefit from PD-1 inhibitor therapy, even for prolonged time periods. As noted above, an early amendment of the Checkmate 205 permitted nivolumab to be continued after the occurrence of investigator-assessed disease progression if prespecified criteria were met. These criteria included stable PS and perceived clinical benefit per investigator assessment. However, treatment was withdrawn in case of further progression defined by ⩾10% further increase in tumor burden. Among 130 patients who developed PD, 80 (62%) were treated beyond progression (TBP) and 50 were not. The 2-year OS rate for those TBP was 87%, and was significantly better than OS in patients not eligible to be TBP. Interestingly, at the last report, the 3-year OS of Checkmate 205 patients who achieved a CR was clearly >90%, while it was ~80% for both patients with PR and SD as best response, despite their clearly different PFS. However, even the minority of patients (11%) who had PD as best response had a 3-year OS of 50% or more. 171 These data suggest that checkpoint inhibitors exert a prolonged beneficial effect on the disease, which is not solely determined by the depth of response, and highlight the importance of TBP, as long as a clinical benefit is being obtained. Whether the ‘10% further progression’ stopping rule should be applied in clinical practice as done in Checkmate 205, is not clear and should be evaluated in clinical trials and real-life studies.
Modulation of the efficacy of checkpoint blockade and potential effect of checkpoint inhibitors on subsequent chemotherapy
In the era of novel agents, one of the main concerns in modern therapeutic approach of rr-cHL remains the treatment of patients that fail checkpoint blockade therapy. In the earliest phase of clinical introduction of checkpoint inhibitors in ‘real-world’ practice, Falchi and colleagues suggested the potential favorable role of hypomethylating agent 5-azacitidine on checkpoint blockade response through a synergistic priming effect on the immune system. 181 Later, in a phase II study of 86 rr-cHL patients who had received at least two lines of previous therapy, the addition of low-dose decitabine to the checkpoint inhibitor camrelizumab led to higher CR rates in anti-PD1-naïve patients that reached 71% versus 32% in the anti-PD1 monotherapy arm. The study revealed the potential of the combination to induce responses in patients who had been previously refractory to PD1 inhibition. 182
Besides evidence supporting the optimization of tumor response to PD1-blockade with the addition of hypomethylating agents, a retrospective trial of 30 patients with rr-cHL and unsatisfactory response to anti-PD1 therapy proposed the beneficial effect of previous checkpoint blockade on the following chemotherapy administration, either alone or in combination with the previous anti-PD1 agent, by demonstrating 61% and 90% objective response rates in the ‘sequential’ and ‘combination’ strategy, respectively. 183 Recently, Carreau and colleagues evaluated 77 heavily pretreated cHL patients who received a subsequent line of therapy after anti-PD1 blockade. Although, ORR to post-anti-PD1 agent correlated with the previous PD-1 blockade response, ORR of nonresponders to anti-PD1 treatment (SD and PD) was 37%, without statistical difference in survival based upon treatment choice, implicating that a small, but significant, proportion of unfavorable patients who had failed on PD-1 blockade, may be sensitized to subsequent therapy and proceed to SCT. 184 However, further prospective studies are required to shed light on this attractive hypothesis.
Toxicities of checkpoint inhibitors
The nature of adverse reactions induced by checkpoint inhibitors differs for traditional cytotoxic therapy, and is due mainly to T-cell hyperactivation. In Checkmate 205 and Keynote-087, drug-related AEs, which occurred in ⩾10% of the patients, included skin rash and fatigue in both studies, plus diarrhea, pruritus, nausea, and infusion-related reactions with nivolumab, and hypothyroidism and pyrexia with pembrolizumab. These AEs are mild and easily manageable. Grade 3/4 drug-related AEs were rare; those occurring in ⩾2% of the patients included neutropenia in both studies and elevations in lipase, amylase, and transaminases in Checkmate 205. Similar grade 4 events were observed at lower frequency with pembrolizumab. In updated reports of both studies, approximately 7% of the patients had discontinued treatment due to drug-related AEs. Among them, pneumonitis (2%) and autoimmune hepatitis (1%) were notable in Checkmate 205, while pneumonitis (3%) and infusion-related reactions were recorded in the Keynote-087 study. However, myocarditis, myelitis, myositis, epilepsy, organizing pneumonia, cytokine release syndrome, etc., were the cause of treatment discontinuation in isolated cases. Interestingly, all deaths recorded in these studies were unrelated to the study drugs.
It should be stressed that immune-related adverse AEs (IMAEs) are the most notable form of toxicity of checkpoint inhibitors, including some of the above mentioned events, as well as others occurring even more rarely. Thus, hypothyroidism and thyroiditis, or, rarely, hyperthyroidism, rash, hepatitis, pneumonitis, colitis, diabetes, hypophysitis, adrenal insufficiency, autoimmune nephritis, etc., should be kept in mind and excluded in cases of clinical suspicion or even carefully monitored over time. The median time to occurrence of IMAEs is ~12 weeks (range between 1 and 112 weeks). Specific guidelines for the management of the IMAEs associated with checkpoint inhibitors have been published elsewhere185,186
In addition, pseudoprogression, an immune-mediated tumor flare, may be observed early during checkpoint inhibitor therapy, and may provoke treatment discontinuation. For this purpose, modified criteria of response have been developed in order to account for this and avoid inappropriate premature drug discontinuation, as discussed above. 179 Finally, PD-1 inhibition in patients who have relapsed after alloSCT may be complicated with relatively high rates of GVHD, though being highly efficient.187,188
Other promising novel agents for relapsed/refractory classical Hodgkin lymphoma
Several novel agents had shown promising results, but their development was delayed or stopped with the appearance of the impressive results obtained with BV and checkpoint inhibitors. The potential role of such targeted agents in rr-cHL, including mTOR inhibitors, lenalidomide, histone deacetylase inhibitors (HDACi), and JAK inhibitors, as well as inhibitors of the B-cell receptor (BCR) pathway,189–210 and details of major clinical trials of these agents are summarized in Table 3.
Experimental agents in relapsed/refractory classical Hodgkin lymphoma.
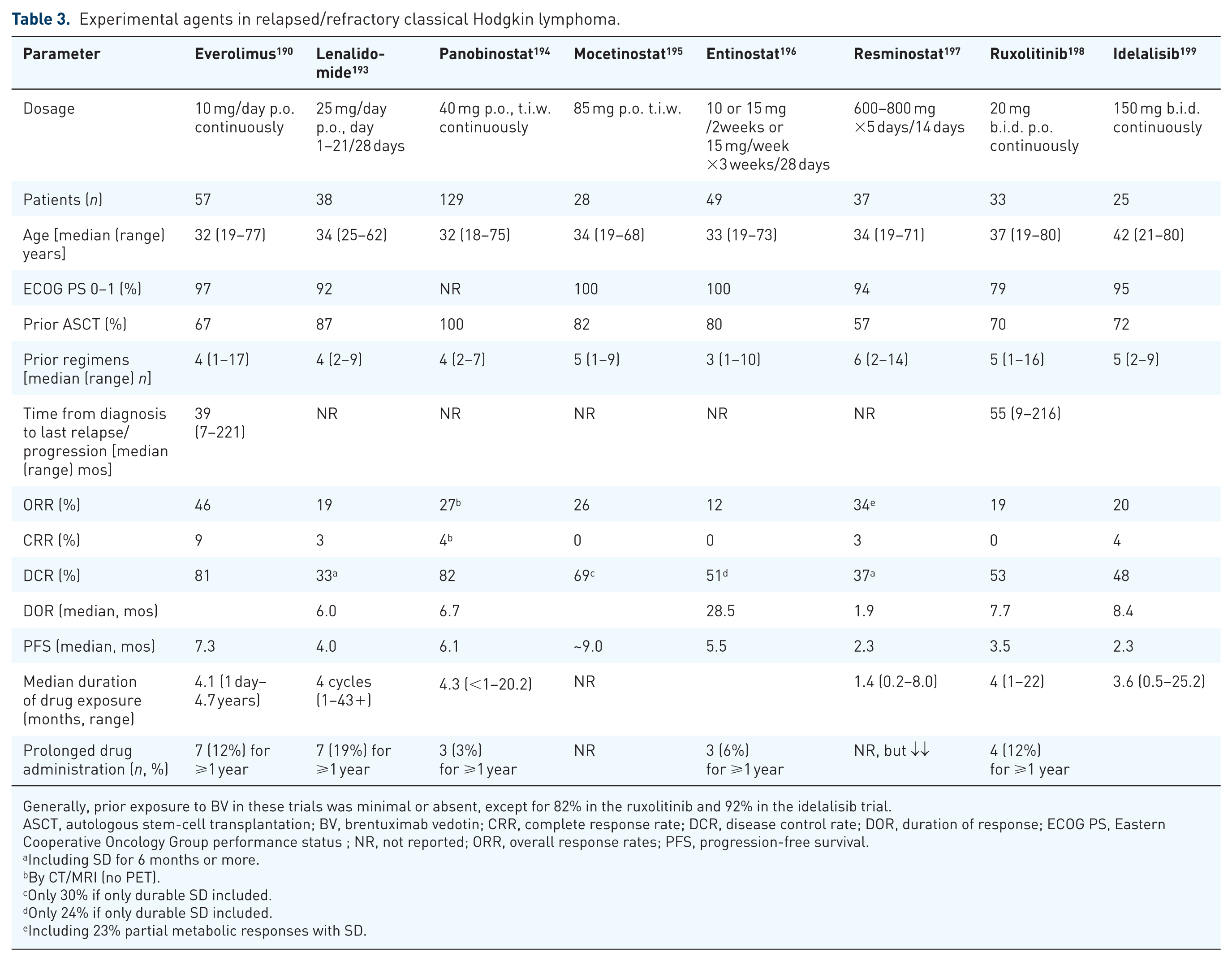
Generally, prior exposure to BV in these trials was minimal or absent, except for 82% in the ruxolitinib and 92% in the idelalisib trial.
ASCT, autologous stem-cell transplantation; BV, brentuximab vedotin; CRR, complete response rate; DCR, disease control rate; DOR, duration of response; ECOG PS, Eastern Cooperative Oncology Group performance status ; NR, not reported; ORR, overall response rates; PFS, progression-free survival.
Including SD for 6 months or more.
By CT/MRI (no PET).
Only 30% if only durable SD included.
Only 24% if only durable SD included.
Including 23% partial metabolic responses with SD.
Everolimus is an oral inhibitor of the phosphatidylinositol 3-kinase/mammalian target of rapamycin (PI3K/mTOR) signaling pathway. Following the encouraging results of an initial phase II study on 19 patients, 189 everolimus 10 mg daily p.o. was evaluated in a phase II study of 57 evaluable, heavily pretreated rrHL patients (details in Table 3). 190 The ORR was 46% with 9% CRs, the disease control rate 81%, the median time to response was 57 days, and the median PFS 7.3 months. Seven patients were long-term responders (12 months or longer), including five in PR. Notably, one PR patient has been on everolimus for 4.7 years. 190 Similar results were reported in a retrospective analysis of 33 heavily pretreated rr-cHL patients from Brazil. 191 The major toxicities of the drug include thrombocytopenia, anemia, fatigue, rash, and stomatitis, 190 while pneumonitis can be an issue in a minority of patients, being grade 3/4 very rarely. 191 Despite the single agent activity of everolimus, the combination everolimus-DHAP did not prove successful in the HD-R3i trial. 192
Lenalidomide is an agent exerting immunomodulatory activity mainly through direct induction of apoptosis, antiangiogenesis, and activation of T-cell mediated immune response. Two small clinical trials demonstrated the efficacy of lenalidomide in heavily pretreated rr-cHL. Later, in a multicenter study of 38 patients, the ORR was 17% with one CR. 193 Recently, the efficacy of lenalidomide-bendamustine combination was evaluated in a phase I/II study, with 75% ORR and 44% CRs independently of previous autoSCT. 200
Panobinostat, Vorinostat, Mocetinostat, and Entinostat regulate several oncogenic pathways by inhibiting histone deacetylase (HDAC). Panobinostat (40 mg t.i.w. in 21-day cycles) was evaluated in a large pivotal international phase II study of 129 rr patients after autoSCT, with ORR of 27% and SD rates of 55%. The median DOR and PFS were 6.9 and 6.1 months, respectively. The most common grade 3/4 toxicities were, by far, thrombocytopenia, followed by anemia and neutropenia. 194 Few studies have examined the combination of panobinostat with either everolimus, with a synergistic effect in HL cell lines, 201 or with lenalidomide in rr-HL patients with no additional favorable outcome compared with the single agents.202,203 Vorinostat had limited efficacy in a phase II study of 27 patients. 204 Lastly, Younes and colleagues evaluated the efficacy and tolerability of mocetinostat in an open-label, single-arm, phase II study in 51 patients with rr-HL, 28 of which received the finally recommended dose of 85 mg p.o. t.i.w. and achieved an ORR of 26%. The 110 mg dose level provided slightly better ORR, but was not well tolerated, with two deaths potentially related to treatment, while the results of entinostat and resminostat were less encouraging.195–197
JAK inhibitors could be active in HL through the blockade of the JAK-STAT pathway. Unfortunately, the clinical results of pacritinib and ruxolitinib were heterogenous and rather disappointing (Table 3).198,205,206 A further study of ruxolitinib is ongoing (NCT02164500). 207
Targeting the B-cell receptor (BCR) pathway with ibrutinib, an oral Bruton’s kinase inhibitor, has shown some efficacy in a limited number of patients.208,209 Ibrutinib is also being evaluated in combination with BV (NCT02744612) and nivolumab (NCT02940301). 210 Similarly, idelalisib, a selectivePI3Kδ inhibitor, might be active in HL, exerting its effects both on the HRS and T-cells. It has shown modest activity in 25 patients heavily pretreated with rr-cHL (Table 3). The median DOR for the five responders was 8.4 months. Rash, diarrhea, and pneumonitis (4%) were AEs of special interest. 199
The potential role of chimeric antigen receptor-modified T cell (CAR-T) therapy in HL is currently under development, while the clinical benefit from the use of such strategies remains obscure. In cHL, the main molecular targets are CD30 and CD123 proteins or EBV-related proteins. Ramos and colleagues reported the administration of CD30+ CAR-T in seven patients with HL. 211 Similarly, Bollard and colleagues reported the infusion of autologous T-cells against EBV antigens latent membrane protein 1 and 2 (LMP1 and LMP2) in 50 patients with EBV-associated lymphoma, including 25 HL patients: when administered in patients with active, relapsed disease, the ORR was ~50%, while all high-risk patients who received these products as consolidation therapy remained in remission. 212 Further details on CAR-T cells and other forms of immunotherapy as discussed in more detail elsewhere. 178
The role of allogeneic stem-cell transplantation in the era of novel agents
Being, in the past, the only strategy with curative potential in rr-cHL, the role and the optimal timing of alloSCT have been questioned in the era of BV, and, especially, PD-1 inhibitors. Although patients who fail autoSCT now have improved outcomes, and a small minority may even be cured with novel agents, they still represent an unmet medical need.130,131 The existence of graft versus HL effect is suggested by the association of chronic GvHD (cGVHD) with lower relapse rates, and this forms the rationale of alloSCT in HL.213,214
Historically, the applicability of alloSCT can be divided in three time periods. During the first period, up to 2000, the use of myeloablative conditioning (MAC) was the rule, with disappointing OS of 20–30%, owing mainly to unacceptable nonrelapse mortality (NRM) of 30–50%.213,215–218 During the second period, 2000–2010, the use of reduced intensity conditioning (RIC) dominated, leading to substantially lower NRM rates of 15–30%,147,148,213,219–222 lower incidence of acute graft versus host disease (aGvHD) with similar chronic GvHD (cGvHD), and, consequently, an OS still in favor of RIC. 214 The superiority of RIC alloSCT over conventional chemotherapy after autoSCT failure was suggested by a large, Italian, donor versus no donor retrospective study, 214 demonstrating PFS rates between 30% and 40%, and RIC had, therefore, been established as the standard therapeutic strategy for patients who progress after autoSCT.214,223–225 Despite the improvement in the outcomes of alloSCT for rr-cHL during this second period, as recently shown in a meta-analysis including 42 trials, 224 no plateau in the survival curves was evident, implying that there was still room for improvement. 224 During the currently evolving third period, the introduction of novel agents, mainly BV and PD-1 inhibitors, the reappraisal of RIC, and the feasibility of haploidentical transplants incorporating the new immunosuppressive strategy of post-transplant cyclophosphamide (PtCy) for GvHD prevention, are changing the field of alloSCT in rrHL.
The most important prognostic factor for a favorable outcome of alloSCT remains chemosensitive disease, although a small fraction of chemoresistant patients may be cured.147,214,223,225,226 However, consecutive chemotherapy regimens to induce remission frequently impair patients’ PS, rendering them ineligible for alloSCT. In this perspective, novel agents may induce a ‘low burden’ state without significant PS decline in previously ‘chemoresistant’ patients, turning them into ideal candidates for alloSCT. Nevertheless, by changing the natural history of rr-cHL from a fatal to a ‘chronic’ disease, novel agents pose a great dilemma on whether, and when, patients should be referred for alloSCT.
Given that <10% of all patients who receive BV for rr-cHL after autoSCT can achieve long-term disease control without further treatment,124,152 it was thought reasonable to consolidate patients with PR/SD to BV with alloSCT as soon as possible, 227 taking into consideration that pre-alloSCT BV does not negatively affect the outcome of transplantation. 228 Furthermore, due to the evolving position of BV in the treatment algorithm of HL, we will encounter patients who will have already received BV earlier in disease course. Thus, after autoSCT failure, BV will not be an option for many patients, especially those who progress after autoSCT consolidation.
The introduction of PD-1 inhibitors has produced even more uncertainty on whether, and which, patients should be referred for an alloSCT, and when, as both nivolumab and pembrolizumab induce rapid, impressive, and durable responses in approximately 70% of patients who have failed multiple treatments, including autoSCT and BV, albeit with low CR rates.166,168 Patients progressing on BV should be treated with PD-1 inhibitors, given the dismal results with alloSCT in chemoresistant cases. Whether patients who achieve PR/SD with BV should be treated with PD-1 inhibitors in an effort to deepen responses before alloSCT is a matter of debate. A few facts have to be considered; firstly, the achievement of metabolic CR is not necessarily associated with significantly better SCT outcomes; that is, a positive PET/CT should not preclude alloSCT, while increasing lines of treatment prior to the procedure correlate with NRM. 229 Secondly, there is some evidence, although as yet immature, that PD-1 inhibitors before alloSCT may be associated with more frequent liver veno-occlusive disease, severe (grade IV) GvHD, and a noninfectious febrile syndrome responding to steroids.230,231 Taking these facts into consideration, patients with a PR, or even SD, and a low disease burden after BV, should be at least referred for alloSCT consultation. Recent evidence suggests that, despite the moderate risk of alloSCT complications after PD-1 blockade, the long-term efficacy of alloSCT may be actually enhanced by prior exposure to these agents. However, a close collaboration between the treating physicians and the transplant center is mandatory in decision making and transplant preparation.
Although the follow up of PD-1 inhibitors’ studies is still short, there is compelling evidence that even nonresponders or progressors according to conventional criteria derive long-term benefit from TBP, and may not need next antilymphoma treatment for protracted periods of time, rendering rr-cHL a chronic disease. It would be desirable for these new ‘immunologic’ drugs to alleviate the need for an alloSCT; however, the field is still evolving. Given the complexity of patient and timing selection, specific recommendations on the application of PD-1 inhibitors in the context of alloSCT have been published recently: experts in the field recommend to keep responders on PD-1 inhibitors rather than stopping treatment and proceeding to alloSCT, whereas heavily pretreated patients due to multiply refractory disease are the ones who should be considered for an early alloSCT, after response to PD-1 treatment. 232 For patients scheduled for alloSCT, a 6-week PD-1 treatment-free period is recommended before the procedure. Other considerations include the use of bone marrow grafts instead of peripheral blood, the use of PtCy for GvHD prevention, and prompt implementation of GvHD treatment. 232
On the other hand, the immune effects of PD-1 inhibitors are even more detrimental when given after alloSCT. Although responses are impressive and durable in this setting as well, GvHD has been reported in 30–55% of patients, most frequently acute. PD-1-induced aGvHD occurs after the initial one to two infusions, and is frequently severe and steroid-refractory.187,188 The probability of acute GvHD is higher, the closer to alloSCT the PD-1 inhibitor is given, and in patients with a previous history of aGvHD, 187 although PD-1-induced aGvHD was observed also in patients with no prior history of aGvHD. 188 Previous post-Cy or antithymocyte globulin GVHD prophylaxis may be associated with less aGvHD, with PD-1 blockade after alloSCT. Further recommendations include avoiding PD-1 inhibitors during the first 6 months after alloSCT, and initiating treatment at lower doses (e.g. 0.5 mg/kg nivolumab). 232
Another recent evolution is the reconsideration of the conditioning regimens and type of transplants. The most intriguing progress has been made in haploidentical transplantation with PtCy, providing a donor in a timely manner for the majority of rr-cHL patients, while PtCy as GvHD prophylaxis is associated with less immune complications in the era of PD-1 inhibitors, before or after alloSCT, without alleviating graft versus lymphoma effect. Results are impressive, with PFS and OS rates of 51–63% and 63–77%, respectively, with acceptable NRM (4–31%).233–235 In the haploidentical alloSCT setting, disease status pretransplantation is of prognostic importance, with SD patients having a dismal prognosis. The use of peripheral blood stem-cells as graft source is associated with better long-term outcomes due to lower relapse rates. 233 However, excessive complications may be encountered with PBSC in the context of previous PD-1 treatment, as stated above.
As the role of alloSCT is changing in the era of novel agents, its exact position in rr-cHL is not yet clearly defined. PD-1 inhibitors may actually not undermine its role, but establish alloSCT as another tool after PD-1 failure, especially in the haploidentical PtCy setting.
Conclusion
The outcome of patients with rr-cHL has improved considerably in recent years owing to the approval of highly active novel agents in the form of brentuximab vedotin and PD-1 inhibitors. Although no randomized trials have been conducted to provide formal proof, it is almost undisputable that the OS of these patients has been prolonged, since, in most of them, a rapidly lethal disease can be transformed in a chronic, smoldering, disease. As autoSCT remains the standard of care for second-line therapy for most patients with rr-cHL, optimization of second-line regimens with the use of brentuximab vedotin, or, in the future, checkpoint inhibitors, is promising to increase both the eligibility rate for transplant and the final outcome. The need for subsequent therapy, and especially alloSCT, can be reduced with brentuximab vedotin consolidation for 1 year, while pembrolizumab is also tested in this setting. Several other drug categories appear to be active in rr-cHL but their development has been retarded by the appearance of brentuximab vedotin, nivolumab, and pembrolizumab, which have dominated the field of rr-cHL treatment during the last 5 years. Combinations of active drugs in chemo-free approaches and modulation of PD-1 inhibitors’ activity by hypomethylating agents may further increase efficacy, and hopefully reduce toxicity in rr-cHL, but are still under development.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and publication of this article.
Conflict of interest statement
TPV has been an advisory board member and has received honoraria from TAKEDA, BMS and MSD. MKA has been an advisory board member and has received honoraria from TAKEDA and BMS.