
Abstract
FMS-like tyrosine kinase 3 (FLT3) mutations are one of the most frequently encountered genetic alterations in acute myeloid leukemia (AML), and are generally associated with unfavorable outcomes. Several tools are currently available to provide an accurate prognosis for patients with these mutations, including FLT3 mutation type (internal tandem duplication versus tyrosine kinase domain), mutation allelic ratio (high versus low), and concurrent nucleophosmin-1 (NPM1) mutation, to help decide on optimal treatment. Recent advances in targeted therapies have paved the way for modern treatment strategies, such as the development of FLT3 kinase inhibitors. These novel drugs can be incorporated into any treatment component, including induction and consolidation, the relapse/refractory setting, bridging for transplant, salvage post-transplant, and as prophylactic long-term post-transplant maintenance. Many challenges remain though, such as their intolerability with high-dose chemotherapy in frail patients; whether their optimal use involves watchful waiting for molecular or hematologic relapse compared with prophylactic use as maintenance; and the exact role and indication for allogeneic stem cell transplantation, which arguably remains the only curative option for these high-risk patients.
Keywords
Introduction
Acute myeloid leukemia (AML) is a heterogenous disease, characterized by a myriad of symptom presentations, karyotype anomalies, and genetic alterations. Of these alterations, around 30% are accounted for by FMS-like tyrosine kinase 3 (FLT3) mutations, thus making this type of mutation one of the most frequently encountered, especially among young AML patients.1–3
FLT3 mutations are usually categorized into one of two groups: internal tandem duplication or FLT3-ITD (occurring in or near the juxta-membrane domain of the receptor), and tyrosine kinase (TK) domain point mutations or FLT3-TKD (resulting in single amino acid substitutions within the activation loop). 4 ITD mutations cause an amino acid sequence change while preserving coding frames, resulting in the activation of both TK and downstream signaling pathways and eventual cellular proliferation dysregulation. 5 ITDs are usually located in exons 14 and 15 of the FLT3 gene with heterogeneous insertion site position, number, and size of duplicated fragments. 6
Data on FLT3-TKD prognosis remains conflicting, with some studies suggesting a negative impact of TKD mutations on disease free survival (DFS), event free survival (EFS), and overall survival (OS),7–9 while others suggest no prognostic effect or benefit when the mutation is present.10,11 FLT3-ITD mutations, on the other hand, are well recognized to carry a worse outcome because of high relapse rates, with a good understanding of their impact depending on both allelic burden and concomitant nucleophosmin-1 (NPM1) mutations.9,12–15
Indication for transplant
Although many would argue that all FLT3-mutated patients should be considered ‘high-risk’, among FLT3-mutated patients, disease risk can be classified according to FLT3 allelic burden with the term ‘high-risk’ mostly reserved for those with high allelic burden (0.5), that is, patients harboring homozygous ITD mutations. These patients are usually faced with extremely poor outcomes, and are advised to undergo allogeneic hematopoietic stem cell transplantation (allo-SCT) when first complete remission (CR) is achieved in an effort to maximize prognosis and improve OS.16–18 Despite recent advances, these patients have high rates of early relapse, coupled with lack of response to further therapy and poor long-term survival,19,20 with the most dismal prognosis observed in post allo-SCT relapse patients, in whom the 1-year OS has been found to be less than 20%. 21
Some authorities, such as the European Leukemia Net (ELN), classify the disease as low-risk disease with the presence of low allelic ratio (<0.5) and concomitant NPM1 mutation. These patients usually appear to have good OS even without transplantation, thus raising the question of its benefit. Nonetheless, the prognostic value of allelic ratio is not universally accepted, with some data suggesting poor outcomes regardless of mutation status, especially when patients do not receive a transplant. A study conducted on 147 patients found that NPM1-positive patients with low allelic ITD still had unfavorable outcomes, with an OS of only 41%, but that significant improvements were seen in both relapse-free survival (RFS) and OS when patients had undergone allo-SCT in first complete remission (CR1). 22 This challenges the notion of withholding transplant for patients with a supposedly favorable outcome, suggesting its universal use could be the better alternative.
Finally, patients with low allelic ITD ratio lacking the NPM1 mutation (and lacking other adverse risk mutations) are currently considered intermediate risk and fall in a grey area with no proper consensus on optimal treatment strategy. Current practice is conflicted between universal allo-SCT for these patients, or restricted allo-SCT only for those that do not achieve minimal residual disease (MRD) negativity.
It is noteworthy that much of the available data leading to these guidelines, including the ELN recommendations, were generated in the era when tyrosine kinase inhibitors (TKIs) were not routinely added to frontline therapy.
Tyrosine kinase inhibitors
Small-molecule FLT3 TKIs have become an integral part of FLT3 AML treatment, and several TKIs have been studied extensively in the past decade.23,24 They have been shown to have single agent activity, but work synergistically when incorporated into existing treatment strategies. Hence, they can be used during induction in combination with chemotherapy or hypomethylating agents (Table 1), as a relapse/refractory bridge for transplant, as salvage therapy for relapsed patients (Table 2), or as prophylactic maintenance therapy to preserve MRD negativity (Table 3).
FLT3 inhibitors during induction/consolidation.
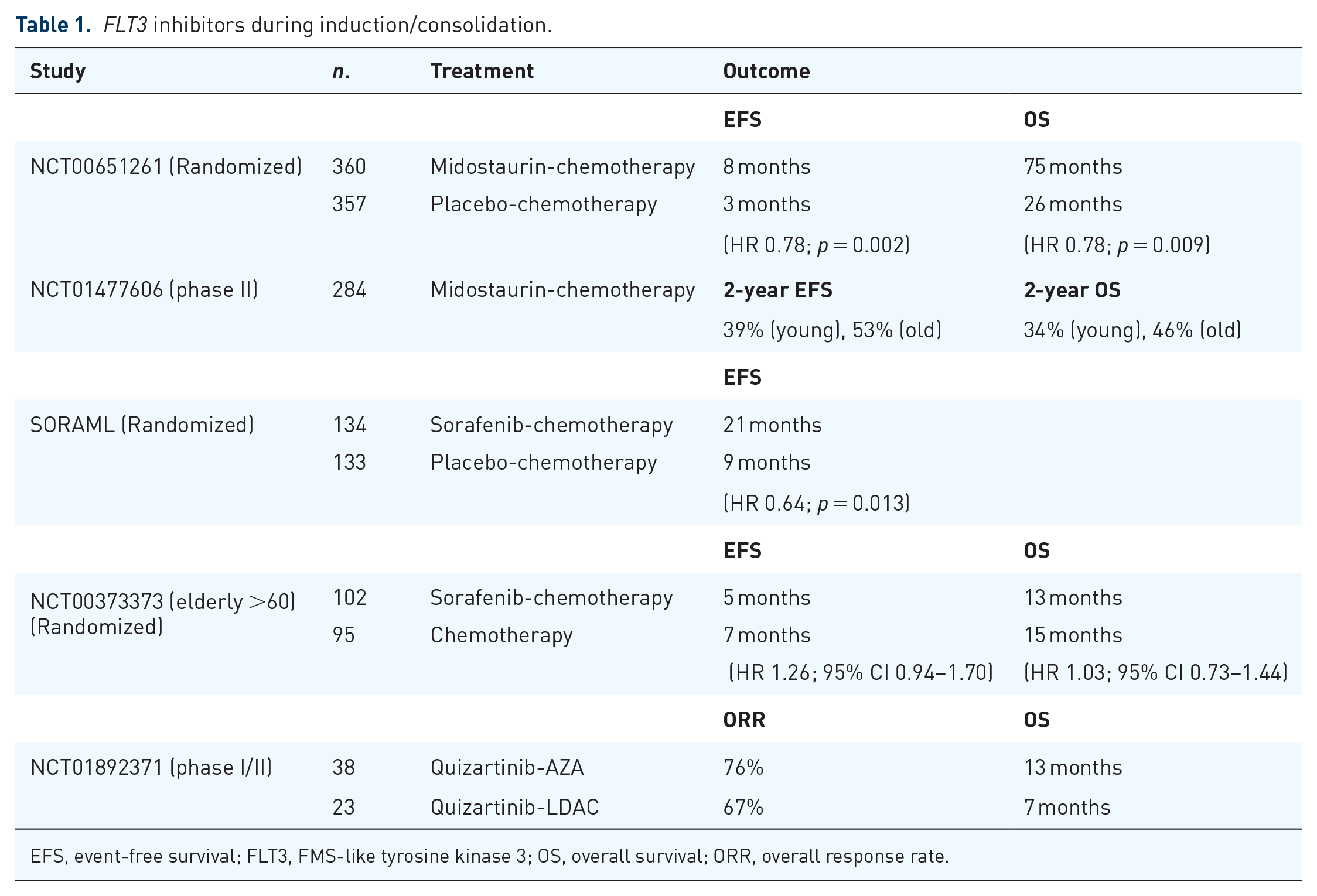
EFS, event-free survival; FLT3, FMS-like tyrosine kinase 3; OS, overall survival; ORR, overall response rate.
Sorafenib for relapsed AML including after allo-SCT.

CMR, complete molecular remission; OS, overall survival.
FLT3 inhibitors as maintenance post-allo.

CR, complete remission; GFRS, GVHD-free relapse free survival, GVHD, graft-versus-host disease; LFS, leukemia-free survival; OS, overall survival; RFS, relapse-free survival.
FLT3 inhibitors during induction/consolidation
Midostaurin
Midostaurin is a multitarget kinase inhibitor that was originally developed to target protein kinase C and used for the treatment of solid tumor patients. 25 Preclinical data, however, have shown that midaustaurin has FLT3 inhibition activity, with results suggesting synergy between midostaurin and chemotherapy. 26 This prompted the start of a phase Ib study involving patients with newly diagnosed AML, which later established the safety and efficacy of oral midostaurin at 50 mg twice daily for 14 days starting on day 8 after treatment initiation of both induction and consolidation chemotherapy in FLT3 mutated patients. 27
Based on these findings, the phase III RATIFY trial was conducted (NCT00651261), evaluating the addition of midostaurin to standard chemotherapy (induction therapy with daunorubicin and cytarabine and consolidation therapy with high-dose cytarabine) compared to placebo in adult AML patients with further stratification of patients achieving CR after consolidation by midostaurin maintenance versus placebo. 33 A total of 717 newly diagnosed AML patients were randomized into three groups: FLT3-TKD mutations, mutated to wild-type ITD allelic ratio >0.7, and ITD allelic ratio ⩽0.7. Overall, 360 patients received midostaurin and 357 received placebo. High ITD allelic ratio was observed in 214 patients, low ratio in 341 patients, and TKD in 162 patients. Overall survival and EFS were significantly longer in the midostaurin group [hazard ratio (HR) = 0.78, p = 0.009 and HR = 0.78, p = 0.002, respectively], with similar adverse event rates between the groups. Importantly, subgroup analysis demonstrated midostaurin benefit in all FLT3 subtypes even after censoring patients who underwent allo-SCT. Addition of midostaurin to standard chemotherapy therefore significantly prolonged OS and EFS in FLT3 mutated AML patients, with no increased toxicity. These findings led to the drug’s recent FDA approval for use in this setting.
Shortly after the FDA approval, a phase II hypothesis-generating trial (NCT01477606) was conducted to determine whether the addition of midostaurin to intensive chemotherapy, followed by allo-SCT with single agent maintenance for 12 months is feasible and improves outcomes when compared with historical controls. 34 Of 284 newly diagnosed AML patients with FLT3-ITD, aged 18–70 years, 76% of patients achieved CR, (of which 72% underwent transplantation), and 34% received maintenance therapy (75 patients post allo-SCT, 22 patients post consolidation) for a median of 9.0 and 10.5 months, respectively. The 2-year EFS and OS was 39% and 53% in younger (18–60 years) patients and 34% and 46% in older (61–70 years) patients, respectively. Comparing EFS with 415 historical controls within five prospective trials, propensity score-weighted analysis revealed a significant improvement with the addition of midostaurin overall (HR = 0.58, p < 0.001) and in older patients (HR = 0.42, 95% CI 0.29–0.61).
Midostaurin therefore plays an integral role in the treatment of FLT3 mutated patients, appearing safe and effective with high-intensity induction/consolidation chemotherapy.
Sorafenib
Sorafenib is another oral kinase inhibitor originally developed to target the serine/threonine kinase Raf and approved for use in kidney and hepatocellular carcinomas.35–37 However, sorafenib was also found to effectively inhibit other kinases, including vascular endothelial growth factor (VEGF) receptors, cKit, platelet-derived growth factor (PDGF) receptors, and, importantly, FLT3; all of which are expressed on AML and bone marrow stromal cells supporting tumorigenesis.38–40 Preclinical in vitro and in vivo data suggested efficacy of sorafenib against AML blasts, which prompted a phase I/II study that later showed the safety and efficacy of sorafenib 400 mg twice daily for 7 days in combination with idarubicin-cytarabine-based induction chemotherapy in AML patients <65 years of age.41–46
The randomized, double-blind, placebo-controlled multicenter SORAML phase II trial (NCT00893373) evaluated newly diagnosed adult AML patients <60 years of age receiving daunorubicin-cytarabine-based induction chemotherapy followed by cytarabine consolidation plus either sorafenib (400 mg twice daily) or placebo. The drug was administered on days 10–19 of induction cycles 1 and 2, from day 8 of consolidation, and as maintenance for 12 months. 47 Overall, 267 patients were included (134 received sorafenib and 133 received placebo) with a 36-month median follow-up. Median EFS was 9 months in the placebo group versus 21 months in the sorafenib group (HR = 0.64, p = 0.013), with a 3-year EFS of 22% versus 40% respectively. Sorafenib patients experienced increased rates of ⩾grade 3 adverse events, notably fever [relative risk (RR) 1.54], diarrhea (RR 7.89), bleeding (RR 3.75), cardiac events (RR 3.46), rash (RR 4.06), and hand-foot-skin reaction observed only in the treatment arm. These findings suggest that sorafenib does have antileukemic activity which increases efficacy when added to standard chemotherapy, interestingly irrespective of FLT3 mutation status, but at the expense of increased toxicity.
A phase III randomized placebo controlled trial (NCT00373373) was also conducted, assessing the combination of sorafenib with intensive chemotherapy in elderly AML patients >60 years of age compared with chemotherapy alone. 48 Overall, 197 patients were included in the study (102 and 95 in the sorafenib and placebo groups, respectively). Treatment in the sorafenib arm however did not result in improved EFS or OS, even for subgroup analyses including FLT3-ITD patients. Patients had more adverse effects during induction in the sorafenib group resulting in higher treatment-related mortality (TRM) and lower CR rates due to less consolidation therapy being given as a result of the increased toxicity. These results suggest that standard induction/consolidation chemotherapy with sorafenib is an inadequate choice for elderly AML patients due to severe toxicity.
Quizartinib
Quizartinib is another potent selective FLT3 inhibitor with proven activity in the relapse/refractory setting (discussed later in detail). This drug has been investigated in previously untreated high-risk myelodysplastic syndrome (MDS), chronic myelomonocytic leukemia (CMML), and AML elderly patients (>60 years) in a phase I/II trial in combination with 5-azacitidine (AZA) or low dose cytarabine (LDAC) in an effort to decrease toxicity and increase tolerability in elderly patients, relative to high-dose chemotherapy. 49 An overall response rate (ORR) of up to 92% has been seen with quizartinib use in previously untreated patients, with a median OS of 19 months. The combination had a very tolerable toxicity profile and proved effective (especially with AZA), showing that a hypomethylating agent combined with a FLT3 inhibitor is an effective option for previously untreated elderly patients intolerant to intensive chemotherapy. Current trials investigating upfront therapy with quizartinib in combination with induction chemotherapy in newly diagnosed AML patients are still ongoing with promising results. 50
FLT3 inhibitors for relapsed/refractory AML
Sorafenib
The efficacy of sorafenib in treating relapsed FLT3-ITD patients has been reported and has long been established.51,52 A long-term follow-up analysis of a previously reported cohort of 29 relapsed FLT3-ITD AML patients treated with sorafenib monotherapy has been conducted, whereby after a median follow-up of 7.5 years, six patients (21%) were still alive. 53 Excluding one patient who had received a second allo-SCT, the remaining five had achieved sustained CR with sorafenib monotherapy even after years of therapy discontinuation. Despite the small number of patients enrolled, sorafenib appears to be effective and associated with long-term disease control in a subset of patients relapsing after allo-SCT.
Quizartinib
Quizartinib is a potent selective inhibitor of FLT3 kinase and was evaluated in relapsed/refractory AML patients irrespective of FLT3-ITD mutation status in a phase I, first-in-human study (NCT00462761). 54 A total of 76 adult patients (23–86 years old) were enrolled with a median of three prior therapies, and quizartinib was administered orally at escalating doses from 12 to 450 mg/day. The maximum tolerated dose was 200 mg/day, with dose-limiting toxicity being QT interval prolongation. Most common treatment related adverse events were nausea (16%), QT prolongation (12%), vomiting (11%), and dysgeusia (11%), although most were mild (grade ⩽2). Treatment was associated with complete inhibition of FLT3-ITD phosphorylation with 30% of patients achieving response [13% CR, 17% partial response (PR)]. Out of 17 FLT3-ITD positive patients, 9 (53%) responded to treatment, compared with only 5 (14%) out of 37 of FLT3-ITD negative patients. The remaining 22 patients were FLT3-ITD indeterminate/not tested, and the response rate was 41%. Median overall duration of response was 13.3 weeks, with a median survival of 14 weeks. Thus, quizartinib showed significant clinical activity in relapsed/refractory AML patients, particularly with FLT3-ITD mutation, all while maintaining an acceptable toxicity profile.
Based on these findings, a global randomized phase III QuANTUM-R trial was conducted (NCT02039726), evaluating the safety and efficacy of quizartinib versus investigators’ choice of salvage chemotherapy in relapsed/refractory FLT3-ITD AML. 55 Overall, 367 adult patients aged 18–81 years old were randomized 2:1 to receive quizartinib (n = 245) 60 mg (with 30 mg lead-in) or salvage chemotherapy (n = 122) selected prior to randomization. Regimens included low dose cytarabine (LDAC) (n = 29); mitoxantrone, etoposide, intermediate-dose cytarabine (MEC) (n = 40); or fludarabine, cytarabine, or granulocyte-colony stimulating factor with idarubicin (FLAG-IDA) (n = 53). Up to two cycles of MEC/FLAG-IDA were permitted, and both quizartinib and LDAC were given until lack of benefit, evidence of unacceptable toxicity, or HSCT. Patients who had previously received FLT3 inhibitors other than midostaurin were excluded, and those that underwent transplant while in the quizartinib arm continued the drug as maintenance. After a median follow-up of 102 weeks, median OS was 27 weeks when treated with quizartinib compared with 20 weeks with chemotherapy, with an estimated survival at 1 year of 27% versus 20% for the two groups, respectively. Both arms had very similar rates of treatment-related adverse events, and only two patients had to discontinue quizartinib due to QT prolongation. These results demonstrate that use of single-agent quizartinib significantly prolongs OS in relapsed/refractory FLT3-ITD AML patients compared to standard chemotherapy alone, confirming its efficacy and safety.
Quizartinib, however, was not granted FDA approval for relapsed/refractory AML due to concerns over the credibility and generalizability of the trial data, mostly involving imbalances in early-censored (prior to week 8 after randomization) patients for OS, the number of patients randomized but not treated, among other reasons. 56
Gilteritinib
Gilteritinib (ASP2215) is a highly selective, potent FLT3/AXL inhibitor with activity against both FLT3-ITD and FLT3-TKD, and has been recently assessed for use in the relapsed/refractory setting in a phase I/II trial (NCT02014558), which led to its approval in this setting.57,58 A total of 252 adults with relapsed/refractory AML were enrolled into one of seven dose-escalation (n = 23) or dose-expansion (n = 229) cohorts, receiving a once-daily oral dose of gilteritinib (20 mg, 40 mg, 80 mg, 120 mg, 200 mg, 300 mg, or 450 mg). The maximum tolerated dose was 300 mg/day, and most common grade 3/4 treatment-related adverse events were diarrhea (37%), anemia (34%), fatigue (33%), and elevated liver enzymes (26% AST, 19% ALT), with 7% of deaths judged as possibly treatment-related. FLT3 phosphorylation inhibition occurred at all dose levels correlating with plasma concentrations of gilteritinib, with more than 90% inhibition observed by day 8 at ⩾80 mg; 40% of patients responded to treatment, with 8% achieving CR, 4% CR with incomplete platelet recovery, and 18% CR with incomplete hematological recovery. An additional 10% of patients had PR, demonstrating the favorable safety profile of gilteritinib along with its ability to induce response in half of relapsed/refractory AML patients due to its potent FLT3 inhibition.
FLT3 inhibitors in combination with hypomethylating agents
As previously alluded to, a decrease in survival was seen in elderly AML patients with the combination of sorafenib and conventional chemotherapy due to high toxicity. A different approach was needed for these frail patients; hence, the replacement of intensive chemotherapy with hypomethylating agents.
A phase II study (NCT01254890) evaluated the use of AZA plus sorafenib in patients with FLT3-ITD mutated AML. 59 Patients received 75 mg/m2 of intravenous AZA daily for 7 days and oral sorafenib 400 mg twice daily at 1 month interval cycles. A total of 43 patients (median age 64 years) were enrolled, with 37 patients evaluated for response. The FLT3-ITD mutation was detected in 93% of patients, with a median allelic ratio of 0.32. Patients had already received a median of 2 prior treatment regimens, with nine patients having failed prior FLT3 kinase inhibitor therapy. The response rate was 46%, including 27% CR with incomplete count recovery (CRi), 16% CR, and 3% PR. A total of 64% of patients achieved adequate FLT3 inhibition (defined as >85%) from their first cycle of therapy, whereby the degree of inhibition correlated with plasma sorafenib concentrations. The combination of AZA and sorafenib therefore appears effective for relapsed FLT3-ITD AML patients, and can be an option for those intolerant of intensive chemotherapy.
Another study also evaluated the combination of sorafenib and AZA in eight relapsed FLT3-ITD AML patients following allo-SCT. 60 Patients received a median of 5 AZA cycles and sorafenib at a median daily dose of 750 mg for a median of 129 days. Furthermore, six of eight patients each received a median of two concomitant donor lymphocyte infusions (DLI). Half of these patients achieved CR and three of them achieved complete molecular remission. Median CR duration was >6 months, with two patients remaining in remission for up to 406 days. Median OS was 11 months. These results further support the efficacy of sorafenib and AZA combinations, and suggests that concomitant DLI use is an option with potentially promising efficacy requiring further evaluation in larger patient groups.
In addition to AZA, sorafenib was evaluated off-protocol in combination with decitabine in six FLT3-ITD patients, five of whom had relapsed/refractory disease.61,62 Patients received at least one to two cycles of decitabine (20 mg/m2) for 10 days and sorafenib (200–400 mg) twice daily for 28 days. The combination proved effective, with five of six patients (83%) responding to treatment, and four of the five (80%) relapsed/refractory patients achieving CR with incomplete count recovery. Median OS was 155 days, with very good tolerability, making the decitabine-sorafenib combination a valid option for patients intolerant of high-dose chemotherapy.
As previously discussed, quizartinib is a potent and selective FLT3 inhibitor that demonstrated activity in the relapsed/refractory setting, with suggested in vitro synergy when added to AZA or LDAC. A phase I/II study (NCT01892371) was therefore conducted to determine dose limiting toxicity/maximal tolerated dose (in phase I) and thus determine the combination’s clinical activity (in phase II). 49 During phase I, patients with relapsed/refractory high-risk MDS, CMML, and AML were included irrespective of FLT3 mutation and salvage status. Phase II, on the other hand, enrolled patients >60 years of age with untreated MDS/CMML/AML as well as patients with FLT3-ITD AML receiving salvage treatment irrespective of age. Patients received 28 days treatment cycles comprising AZA 75 mg/m2 for 7 days per cycle, or cytarabine 20 mg twice daily for 10 days per cycle along with quizartinib at either 60 mg (dose level 1) or 90 mg (dose level 2) daily. A total of 61 patients (12 in phase I, 49 in phase II) were enrolled, 38 in the AZA arm and 23 in the LDAC arm. Median age was 68 years, median number of prior therapies was one, and eight patients had received prior FLT3 inhibitors. For both combinations, quizartinib at 60 mg daily was identified as the recommended phase II dose. A total of 67% of patients in the LDAC and 76% patients in the AZA group responded to treatment, with an ORR of 73% (92% for previously untreated, 68% for previously treated). Furthermore, 23% of the 43 patients that responded (n = 10) reached CR, and 12% (n = 5) achieved MRD-negativity. Median OS in untreated patients was 19 months compared with 11 months in the previously treated group. The ORR of FLT3-ITD patients reached 76% with 9% MRD negativity, and 80% of patients previously exposed to FLT3 inhibitors responded to treatment. Although not statistically significant, patients treated with AZA had better outcomes, with an OS of 13.4 months compared with 6.7 with LDAC, with similar results for RFS (7 versus 3 months). Most common reported grade 3/4 toxicities were electrolyte imbalance, liver enzyme elevation, and cardiorespiratory toxicity. These findings point to the efficacy and tolerability of combining quizartinib with AZA/LDAC, and, perhaps especially, with AZA in AML patients particularly when FLT3-ITD mutations are present. The ORR was higher than expected than either agent alone confirming the preclinical observed synergy.
Sorafenib for relapse after allo-SCT
While FLT3 inhibitors have shown activity in both upfront AML therapy combined with high-dose chemotherapy/hypomethylating agents, and in the relapsed/refractory setting, outcomes are still very poor, and many patients usually succumb to their disease eventually. Allogeneic-SCT has been proposed to be the only curative approach for these patients, with a synergistic effect when combined with FLT3 inhibitors. Sorafenib use was evaluated before or after allo-SCT, not only facilitating allo-SCT by inducing remission but also allowing sustained CR post allo-SCT. 63
A total of 65 patients with FLT3-ITD AML were also evaluated with sorafenib monotherapy, all except 2 of which had relapsed or were chemotherapy-refractory after a median of three prior treatment cycles, with 45% having already undergone allo-SCT. 28 Responses were reported as 37% hematological remission, 8% bone marrow remission, 23% CR (with and without peripheral count normalization), and 15% molecular remission with undetectable FLT3-ITD mRNA. Patients who underwent allo-SCT, however, saw significantly higher rates of complete molecular response, up to 24% compared with 8% in the conventional group. Furthermore, 47% of patients without prior allo-SCT developed sorafenib resistance after a median treatment duration of 136 days, while only 38% of prior transplanted patients developed resistance with a significantly later onset (197 days). Sustained remissions were seen exclusively in the allo-SCT group, highlighting the synergistic effect of sorafenib monotherapy with allo-SCT in inducing a durable response.
The latest published data evaluating sorafenib therapy for FLT3-mutated AML was reported by the Acute Leukemia Working Party of the European Society for Blood and Marrow Transplantation (EBMT). 29 Overall 152 adult patients who relapsed post allo-SCT were included, with a median follow-up after relapse of 22 months. Of these, 34 patients had received sorafenib salvage either alone or in combination whereas 118 had not. It is worth noting that 35% of the patients on sorafenib had dose reductions due to reported toxicities. Sorafenib induced CR in 39% of patients, with multivariate analysis showing significant improvements in OS (HR = 0.44; p = 0.001). Matched-pair analysis of 60 patients further illustrated a 1-year OS of 51% with sorafenib versus 17% for controls and a 2-year OS of 38% versus 9%, respectively. Sorafenib was therefore not only safe, but also very effective as salvage therapy for FLT3-AML post allo-SCT resulting in significant improvements in long-term survival.
One proposed mechanism for this observed synergy is through sorafenib’s promotion of graft-versus-leukemia effect mediated by IL-15 production in FLT3-ITD AML cells. 64 The observed increase in IL-15 production by FLT3-ITD leukemia cells is thought to synergize with the allogeneic CD8+ T cell response, allowing for long-term survival in mouse models. This increase was also observed in human FLT3-ITD AML cells obtained from sorafenib responders with findings indicating the synergism between T cells and sorafenib being mediated via reduced ATF4 expression causing activation of the IRF7-IL-15 axis. It therefore appears that, in addition to its effect inhibiting FLT3, sorafenib could also have another immune-mediated mechanism accounting for its observed efficacy.
In vivo T cell depletion
With sorafenib’s suggested immunomodulatory effect, it is expected to increase the rates of graft-versus-host disease (GVHD), thus potentially increasing morbidity. The use of anti-thymocyte globulin (ATG) prophylaxis was shown to be effective in reducing acute and chronic GVHD post allo-SCT, but could theoretically increase relapse rates when given in high doses (>6 mg/kg ATG Thymoglobulin or >15 mg/kg ATG Fresenius) to patients with high-risk AML. A retrospective analysis from the EBMT was therefore conducted, assessing adult AML patients with intermediate/poor-risk cytogenetics or secondary AML who underwent reduced intensity conditioning (RIC) allo-SCT from matched sibling donors while in CR1, with or without ATG use. 65 In total, 1750 patients were included, 205 of which received high-dose ATG. Median follow up was 45 months. There was no difference in 3-year OS (55% versus 54%) and leukemia free survival (46% versus 50%) between the two groups (high-dose ATG versus control), with similarly nonsignificant differences in relapse incidence (RI) (41% versus 34%), nonrelapse mortality (NRM) (12% versus 16%), and GVHD-free relapse free survival (GFRS) (43 months versus 50 months at 1-year, 31 months versus 36 months at 3-years), respectively. AML patients in CR1 with intermediate/poor-cytogenetics undergoing allo-SCT, even with RIC conditioning, can therefore be safely given ATG, with no negative influence on outcome.
Maintenance post allo-SCT
Midostaurin
As previously discussed in the RATIFY study, midostaurin maintenance after induction/consolidation chemotherapy resulted in significant benefit in EFS and OS in newly diagnosed FLT3-mutated adult AML patients. Despite the high rates of sustained remission provided by allo-SCT, relapse rates remained high (30–59%), necessitating further improvement that could be offered by post-transplant maintenance therapy. 66
The RADIUS trial is a randomized, open-label phase II trial (NCT01883362) investigating post allo-SCT maintenance with 50 mg twice daily midostaurin compared to standard of care treatment. 67 A total of 60 adult patients aged 18–70 years were randomized (30 patients per arm) with treatment starting 28–60 days post allo-SCT over a minimum of 24 months follow up. Median exposure to midostaurin was 10.5 months, with a median dose intensity of 93 mg/day. Estimated relapse rates at 18-months were 24% in the standard of care group and 11% in the midostaurin group, equivalent to a 46% relative reduction with the addition of midostaurin. Severe adverse events were reported in 57% and 30% of patients, respectively, the most common being diarrhea (7% versus 13%), nausea (10% versus 3%), vomiting (10% versus 3%), and pyrexia (7% versus 7%). GVHD rates were generally similar between the two groups. Midostaurin maintenance post allo-SCT significantly reduces relapse rates with no major safety concerns.
Sorafenib
Sorafenib has been extensively studied as maintenance post allo-SCT, demonstrating benefit in survival and improvement of outcome. A phase I trial (NCT01398501) was conducted whereby 22 FLT3-ITD AML patients received sorafenib 45–120 days post allo-SCT for 12 cycles of 28 days. 68 Of these 22 patients, 16 were in CR1, 3 in CR2, and 3 had refractory disease. Maximum tolerated dose was established at 400 mg twice daily, and median follow up for surviving patients was 17 months post allo-SCT. Progression-free survival (PFS) was 85% at 1 year (95% for patients in CR1/CR2), with an impressive OS of 95% (100% for patients in CR1/CR2).
Six patients with FLT3-ITD AML were retrospectively assessed after receiving sorafenib (n = 5 maintenance, n = 1 salvage) post allo-SCT, with similarly encouraging results over a median follow-up period of 12 months after sorafenib initiation. 30 Five of these patients developed skin corticosteroid sensitive GVHD within a few days of sorafenib initiation, suggesting a possible immunomodulatory effect, and, remarkably, all patients had sustained molecular remission.
A retrospective analysis was conducted comparing 26 patients who received sorafenib maintenance post allo-SCT to 55 historical controls who did not, all of which had FLT3-ITD AML and were transplanted in CR1. 31 Median time to sorafenib initiation was 68 days post allo-SCT, with a median follow-up of 27 months for the sorafenib group and 38 months for controls. Patients on maintenance had significantly improved 2-year OS (81% versus 62% in controls), with similarly improved PFS (82% versus 53%) and lower RI (8% versus 38%). No difference in 2-year NRM or 1-year chronic GVHD rates were observed, supporting the evidence for sorafenib’s benefit in this setting.
In a multicentric study, 27 FLT3 AML patients (aged 15–57 years) received sorafenib maintenance post-allo-SCT. 32 It was introduced at a median time of 70 days after transplant, with a median treatment duration of 8.4 months. Most reported toxicities were mild (grade 1/2), observed in 11/27 patients, and chronic GVHD was reported in 13 patients (9 limited, 4 extensive). At a median follow-up of 18 months, 25 patients were in complete molecular remission, with 1-year PFS and OS rates reaching 92%. Newly reported updates after a median follow-up of 40 months further demonstrate favorable long-term outcomes with sorafenib maintenance, with 2-year PFS and OS reaching 73% and 80%, respectively. 69
In addition, a large multicenter retrospective analysis conducted by the EBMT assessed outcomes in 462 allografted FLT3 AML patients over a median follow-up of 39 months, 70 with 40% having matched related donors, 49% unrelated, and 11% haploidentical donors. Day-100 grades II–IV and III–IV acute GVHD rates were 26% and 9%, respectively, whereas the 2-year incidences of chronic and extensive chronic GVHD were 34% and 16%, respectively. The 2-year RI and NRM values were 34% and 15%, and leukemia-free survival (LFS), OS, and GRFS were 51%, 59% and 38%, respectively. On multivariate analysis, the need for more than one induction negatively affected outcome with transplant in CR1, improving RI, LFS, and OS. NPM1 mutation also improved outcomes, including RI, LFS, OS, and GRFS. In vivo T-cell depletion reduced chronic GVHD and increased LFS, OS, and GRFS. Lastly, post-transplant maintenance with sorafenib significantly reduced the RI (HR = 0.39; p = 0.05), and improved LFS (HR = 0.35; p = 0.01), OS (HR = 0.36; p = 0.03), and GFRS (HR = 0.44; p = 0.02). Matched-pair analysis was also performed on data from 52 patients (26 in the sorafenib group and 26 controls) who engrafted and survived post allo-SCT with no relapse or grade II–IV acute GVHD until sorafenib initiation. The 2-year LFS was 79% in the sorafenib group versus only 54% in controls, similarly for OS, rates were 83% versus 62%, respectively. Sorafenib maintenance post allo-SCT appears to reduce RI, improve LFS, and OS, and does not affect NRM.
Recently, sorafenib maintenance was assessed in the randomized, double-blind, placebo-controlled SORMAIN trial across 14 centers in FLT3-ITD adult AML patients who had undergone allo-SCT (matched sibling donor, 10/10 or 9/10 matched unrelated). 71 A total of 80 patients were randomized 1:1 to receive either sorafenib (up to 400 mg twice daily) or placebo for up to 24 months. After a median follow up of 42 months, median RFS was 31 months in the placebo group compared to ‘not reached’ in the sorafenib group [corresponding to a 2-year RFS of 53% versus 85% (HR = 0.39, p = 0.0135)]. Overall, sorafenib was well tolerated, with the most common grade 3/4 adverse events in both groups being acute GVHD (18% in placebo versus 21% in sorafenib group). These findings build on the previously reported data and strongly confirm that sorafenib maintenance therapy post allo-SCT in FLT3-ITD AML patients is both feasible and efficient in significantly reducing RI while improving survival.
Gilteritinib
Gilteritinib is also currently being prospectively assessed for maintenance use in FLT3-ITD AML patients post allo-SCT in a phase III, randomized, double-blind, placebo-controlled multicenter trial (NCT02997202). 72 It is being conducted in 149 sites, and aims to enroll 532 adult patients in CR1 randomized 1:1 to receive either 120 mg of gilteritinib or placebo, for 2 years. The primary endpoint is RFS and secondary endpoints are rates of NRM, EFS, OS and GVHD.
Conclusion
FLT3-mutated AML is frequently encountered and leads to unfavorable outcomes. Several prognostic factors should be accounted for when deciding on an optimal treatment strategy, including FLT3 mutation type (ITD versus TKD), mutation allelic ratio (high versus low), and concurrent NPM1 mutation. Many strategies have been implemented to overcome this disease, mainly with the development of FLT3 kinase inhibitors such as midostaurin, sorafenib, quizartinib, and gilteritinib to name a few, which can be added to induction therapies, used in the relapse/refractory/salvage setting, or as maintenance post allo-SCT.
Currently available data suggest positive activity of FLT3 inhibitors in all settings; however, the disease remains incurable for the most part even with their incorporation. The most effective curative option allowing sustained deep remissions for these high-risk patients remains allo-SCT, where transplant appears to synergize with FLT3 inhibitors such as sorafenib through an immunomodulatory effect, inducing a crucial graft-versus-leukemia effect mediating long-term survival. We therefore recommend FLT3 inhibitor combinations with high-dose chemotherapy when feasible as induction therapy, followed by allo-SCT with long-term maintenance of at least 2 years with sorafenib post-transplant. Sorafenib may also be combined with hypomethylating agents in unfit patients not able to receive intensive therapy.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and publication of this article.
Conflict of interest statement
MM received lectures honoraria from Novartis and Daiichi Sankyo whose products are discussed in this manuscript.
AB received lectures honoraria and research support from Novartis whose products are discussed in this manuscript.