
Abstract
Coronary artery disease and peripheral arterial disease are strong predictors of risk for a future ischemic event. Despite the utilization of effective secondary prevention strategies, the prevalence of ischemic recurrences remains high, underscoring the need for effective secondary prevention antithrombotic treatment regimens. To date, most of the tested approaches have been with the use of antiplatelet therapies, used either individually or in combination. However, most recent findings support the potential role of oral anticoagulant therapy in addition to antiplatelet therapy to reduce the risk of ischemic recurrences. This approach has been tested in both acute and stable settings of patients with cardiovascular disease manifestations. The present manuscript provides an overview on the rationale and clinical trial updates on the role of oral anticoagulant therapy, in particular rivaroxaban used at the so-called vascular protection dose, in adjunct to antiplatelet therapy (i.e. aspirin), a strategy known as dual pathway inhibition, for secondary prevention of ischemic recurrences in patients with stable atherosclerotic disease manifestations.
Introduction
Cardiovascular (CV) disorders represent the leading cause of morbidity and mortality. 1 Coronary artery disease (CAD) and peripheral arterial disease (PAD) are strong predictors of risk for a future ischemic event.1–3 Despite the utilization of effective secondary prevention strategies, ischemic recurrences occur in 5–10% of patients with CV disease each year. 3 In particular, patients with CV disease have a 20–60% increased risk of myocardial infarction (MI), 40% increased risk of stroke, and a twofold to sixfold increased risk of death.3,4 The basic pathologic mechanism of adverse ischemic events is the exposure of the subendothelial matrix to circulating blood following rupture or fissure of an atherosclerotic plaque. 5 This process triggers platelet adhesion, activation, and aggregation as well as the coagulation cascade, leading to thrombus formation. 6 These findings underscore the need for antithrombotic therapies targeting pathways leading to thrombus formation with the goal of reducing recurrences. To this extent, a number of antithrombotic strategies have been tested over the course of the past decades. 7 While most of the tested approaches have been with the use of antiplatelet therapies, used either individually or in combination, most recent findings support the potential role of oral anticoagulant (OAC) therapy in addition to antiplatelet therapy to reduce the risk of ischemic recurrences.8–10 Studies have shown that combining antiplatelet and anticoagulant therapies have synergistic effects on thrombus formation (Figure 1). 11 This approach has been tested in both acute and stable settings of patients with CV disease manifestations.8,9 We have previously reported in this journal an overview on the role of non-vitamin K antagonist (non-VKA) OACs (NOACs) in addition to antiplatelet therapy in patients with acute coronary syndrome (ACS). 9 The present manuscript provides an overview on the rationale and clinical trial updates on the role of OAC therapy, in particular rivaroxaban used at the so-called vascular protection dose, in adjunct to antiplatelet therapy (i.e. aspirin), a strategy known as dual pathway inhibition (DPI), for secondary prevention of ischemic recurrences in patients with stable atherosclerotic disease manifestations.

Interplay between antiplatelet and anticoagulant therapies on thrombus formation.
Rationale for novel secondary prevention antithrombotic strategies
Antiplatelet treatment suppresses platelet activation and subsequent aggregation. Aspirin, when used as a secondary prevention agent, lowers the risk of adverse CV events by 19%, while decreasing the risk of CV death by 9% compared with placebo. 12 However, the persistence of a high rate of ischemic recurrences underscores the need for adjunctive antithrombotic approaches.3,4 Indeed, the most studied approach has been represented by the addition of a P2Y12 inhibitor (clopidogrel, prasugrel, and ticagrelor) to aspirin therapy, also known as dual antiplatelet therapy (DAPT). 7 DAPT has indeed represented an effective therapy for patients experiencing an ACS and those undergoing percutaneous coronary intervention (PCI).13–15 Clopidogrel is the P2Y12 inhibitor of choice in patients with stable CAD undergoing PCI, whereas prasugrel and ticagrelor are recommended over clopidogrel in ACS patients owing to their superior efficacy, albeit at the expense of increased bleeding.13–15 However, CV recurrences occur despite the use of DAPT. Moreover, the benefits of prolonging DAPT beyond 1 year in ACS/PCI are counterbalanced by an increased risk of bleeding and no differences in mortality.16–18 These observations have led to investigate antithrombotic strategies targeting other pathways leading to thrombotic complications. 10
Thrombin is known to have a key role in thrombotic processes. In particular, thrombin is the most potent inducer of platelet activation via the PAR receptors. 19 The PAR-1 receptor antagonist vorapaxar used in adjunct to standard of care antiplatelet therapy was associated with a significant reduction in CV recurrences in patients with atherosclerotic disease manifestations (i.e. CAD and PAD). 20 However, there was no reduction in mortality and vorapaxar was associated with a significant increase in bleeding complications, including increased intracranial hemorrhage, among patients with a prior cerebrovascular accident (CVA).
These observations have led to re-evaluate the potential role of oral anticoagulation as a strategy to modulate the effects of thrombin as a secondary prevention strategy in patients with atherosclerotic disease manifestations. 10 Indeed, earlier investigations conducted in the era prior to the advent of P2Y12 inhibiting therapy showed that in patients with CAD, but not other atherosclerotic disease manifestations, the use of VKAs decreased the risk of subsequent CV events.21,22 However, this occurred at the expense of a substantial increase in bleeding in addition to the inherent challenges associated with the use of VKA. However, the development of the NOACs have led to a re-appraisal of the use of OACs for secondary prevention in patients with atherosclerotic disease manifestations.
Indeed, a number of NOACs used in combination with antiplatelet therapy, mostly DAPT with aspirin and clopidogrel, were tested in patients with an ACS.8,9 We have previously reported in this journal an overview on the role of NOACs in addition to antiplatelet therapy in patients with ACS. 9 In brief, only one NOAC (i.e. rivaroxaban) completed phase III clinical trial testing and met its primary endpoint. 23 In particular, in ACS patients treated with DAPT, the adjunctive use of rivaroxaban 2.5 mg or 5 mg twice daily (bid) regimen was associated with a lower risk of CV death, stroke, or MI compared with placebo. Notably, a 2.5 mg bid regimen was associated with a lower mortality rate. Indeed, rivaroxaban (at either dose) showed higher rates of major bleeding complications compared with placebo. However, the 2.5 mg bid dose of rivaroxaban was associated with less bleeding than the 5 mg bid dose, including fewer fatal bleeding events. These observations led to evaluate the potential role of the 2.5 mg bid dose of rivaroxaban, subsequently coined as a ‘vascular protection dose’, to distinguish it from dosing regimens commonly used for other indications (e.g. atrial fibrillation, deep venous thrombosis, and pulmonary embolism) in patients with stable atherosclerotic disease manifestations.
The COMPASS trial
The Cardiovascular Outcomes for People Using the Anticoagulation Strategies (COMPASS) trial was a multicenter, double-blind, randomized placebo-controlled study, comparing rivaroxaban 2.5 mg bid plus aspirin 100 mg once daily (qd) versus rivaroxaban 5 mg bid versus aspirin 100 mg qd in patients with stable CAD or PAD.24,25 The specific study entry criteria and definition of CAD and PAD are given in Table 1. In general, patients at high risk of bleeding were excluded (see Table 1 for specific study exclusionary criteria). The primary efficacy outcome was the composite of CV death, stroke, or MI. There were three secondary efficacy outcomes: the composite of ischemic stroke, MI, acute limb ischemia (ALI), or death from coronary heart disease; the composite of ischemic stroke, MI, ALI, or CV death; and death from any cause. The primary safety outcome was determined by the modified International Society on Thrombosis and Haemostasis (ISTH) criteria for major bleeding and included fatal bleeding, symptomatic bleeding into a critical organ, or bleeding into a surgical site requiring reoperation, and bleeding that led to hospitalization (all bleeding that necessitated patient care at an acute care facility or hospitalization was considered as major). The net clinical benefit outcome was the composite of CV death, stroke, MI, fatal bleeding, or symptomatic bleeding into a critical organ. Using a partial factorial design, patients not receiving a proton-pump inhibitor, were further randomized to pantoprazole versus placebo with the goal of assessing the impact of a proton-pump inhibitor on gastrointestinal complications.
Eligibility criteria.
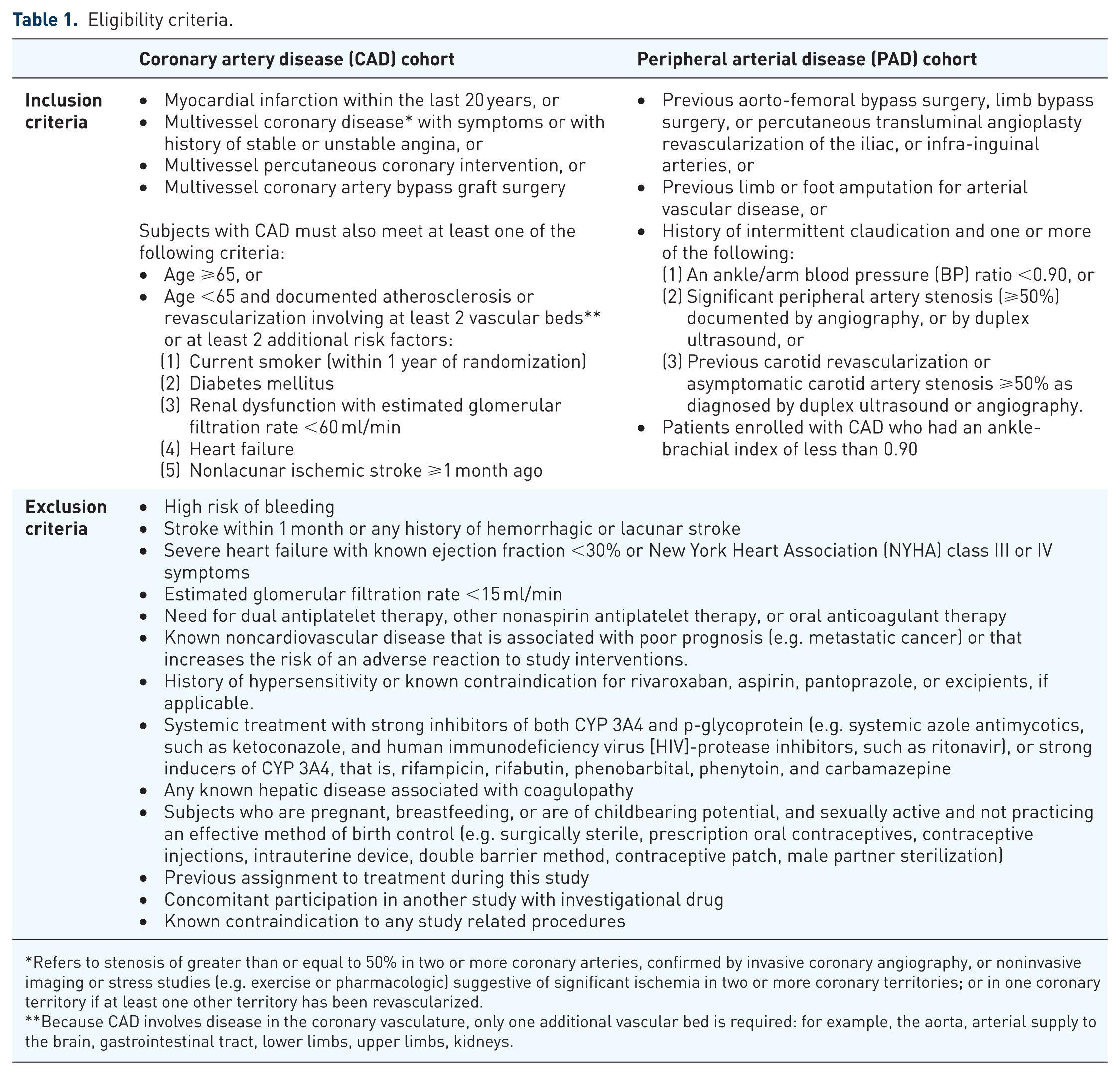
Refers to stenosis of greater than or equal to 50% in two or more coronary arteries, confirmed by invasive coronary angiography, or noninvasive imaging or stress studies (e.g. exercise or pharmacologic) suggestive of significant ischemia in two or more coronary territories; or in one coronary territory if at least one other territory has been revascularized.
Because CAD involves disease in the coronary vasculature, only one additional vascular bed is required: for example, the aorta, arterial supply to the brain, gastrointestinal tract, lower limbs, upper limbs, kidneys.
The COMPASS study randomly assigned on a 1:1:1 ratio 27,395 patients with CAD or PAD from 602 centers across 33 countries to rivaroxaban 2.5 mg bid + aspirin 100 mg qd, rivaroxaban 5 mg bid, or aspirin 100 mg qd. 25 Most patients (90.6%) had a past medical history of CAD, whereas 27.3% had a history of PAD. There were no significant differences in underlying characteristics among the three arms. The mean patient age was 68.2 years and 22% of subjects were females. The use of other secondary prevention medications (e.g. lipid-lowering therapy, angiotensin-converting enzyme inhibitor, or an angiotensin receptor blocker) was high overall. Subject recruitment for the COMPASS trial commenced in early 2013. This investigation was expected to end in 2018. However, in February 2017, after a mean follow-up duration of 23 months, following recommendations from the Data Monitoring Committee, the study was interrupted ahead of its original schedule owing to achieving previously specified criteria for superior efficacy. 25 In particular, the primary outcome event of CV death, stroke, or MI occurred in fewer patients in the DPI group with rivaroxaban and aspirin, as opposed to the aspirin-only group [379 patients (4.1%) versus 496 patients (5.4%); hazard ratio (HR), 0.76; 95% confidence interval (CI), 0.66–0.86; p < 0.001; z = −4.126; number needed to treat, 77] (Figure 2). 25 However, major bleeding occurred more frequently in the DPI group with rivaroxaban and aspirin compared with aspirin-only [288 patients (3.1%) versus 170 patients (1.9%); HR, 1.70; 95% CI, 1.40–2.05; p < 0.001; number needed to harm, 83]. 25 Major excessive bleeding was largely found in the gastrointestinal tract, and there was no significant intergroup difference in rates of fatal bleeding, intracranial bleeding, or symptomatic bleeding into a critical organ (Table 2). 25 There was no significant decrease in the primary outcome event in patients treated with a rivaroxaban 5 mg bid regimen compared with the aspirin only regimen [448 patients (4.9%) versus 496 patients (5.4%); HR, 0.90; 95% CI, 0.79–1.03; p = 0.12] (Figure 2). 25 Major bleeding in the group with a rivaroxaban 5 mg bid regimen was significantly higher compared with aspirin alone [255 patients (2.8%) versus 170 patients (1.9%); HR, 1.51; 95% CI, 1.25–1.84; p < 0.001] (Table 2). 25

Efficacy outcomes in the COMPASS trial.
Bleeding events in the COMPASS trial.

ICH, intracranial hemorrhage; ISTH, International Society on Thrombosis and Haemostasis.
If a participant had more than one event of major bleeding, only the most serious bleeding event was counted in these analyses.
The secondary composite outcomes of the DPI group with rivaroxaban and aspirin was shown to be significantly better than that of the aspirin-only group. 25 In particular, the secondary composite outcome of ischemic stroke, MI, ALI, or death from coronary heart disease occurred in fewer patients in the DPI group with rivaroxaban and aspirin compared with aspirin alone [329 patients (3.6%) versus 450 patients (4.9%); HR, 0.72; 95% CI, 0.63–0.83; p < 0.001]. 25 The secondary composite outcome of ischemic stroke, MI, ALI, or CV death also occurred in fewer patients in the DPI group with rivaroxaban and aspirin compared with aspirin alone [389 patients (4.3%) versus 516 patients (5.7%); HR, 0.74; 95% CI, 0.65–0.85; p < 0.001]. 25 Ultimately, mortality was lower in the DPI group with rivaroxaban and aspirin compared with aspirin alone [313 patients (3.4%) versus 378 patients (4.1%); HR, 0.82; 95% CI, 0.71–0.96; p = 0.01] (Figure 2). 25
In addition to the above-mentioned endpoints, fewer patients had strokes in the DPI group than in the aspirin group [83 (0.9% per year) versus 142 (1.6% per year); HR, 0.58; 95% CI, 0.44–0.76; p < 0.0001]. 26 Ischemic/uncertain strokes were reduced by nearly half [68 (0.7% per year) versus 132 (1.4% per year); HR, 0.51; 95% CI, 0.38–0.68; p < 0.0001] by DPI compared with aspirin. No significant difference was noted in the occurrence of stroke in the rivaroxaban alone group in comparison with aspirin: annualized rate of 0.7% (HR, 0.82; 95% CI, 0.65–1.05). The occurrence of fatal and disabling stroke (modified Rankin scale, 3–6) was decreased by DPI [32 (0.3% per year) versus 55 (0.6% per year); HR, 0.58; 95% CI, 0.37–0.89; p = 0.01]. Prior stroke was the strongest predictor of incident stroke (HR, 3.63; 95% CI, 2.65–4.97; p < 0.0001) and was associated with a 3.4% per year rate of stroke recurrence on aspirin. The effect of the combination in comparison with aspirin was consistent across subgroups with high stroke risk, including those with prior stroke. Although there was a reduction in MI in the DPI group compared with aspirin, this did not reach statistical significance [178 (1.9% per year) versus 205 (2.2% per year); HR, 0.86; 95% CI, 0.70–1.05; p = 0.14].
With respect to the net-clinical-benefit outcome of CV death, stroke, MI, fatal bleeding, or symptomatic bleeding into a critical organ, the risk was lower in the DPI group with rivaroxaban and aspirin in comparison with aspirin only [431 patients (4.7%) versus 534 patients (5.9%); HR, 0.80; 95% CI, 0.70–0.91; p < 0.001]. The net-clinical-benefit outcome in the group with rivaroxaban alone was not significantly lower than the group with aspirin only [504 patients (5.5%) versus 534 (5.9%); HR, 0.94; 95% CI, 0.84–1.07; p = 0.36]. 25
COMPASS CAD subanalysis
The COMPASS trial enrolled a total of 24,824 patients with stable CAD as defined in Table 1.25,27 A history of MI was present in 69% (17028 patients) of these patients, 5% (1238 patients) of which had occurred within 1 year of enrolment, 29% (7234 patients) between 1 and 5 years and 34% (8520 patients) beyond 5 years from enrolment. The occurrence of the primary efficacy and safety endpoints in the CAD cohort was consistent with that of the overall COMPASS trial population. In particular, the primary outcome decreased in the DPI group with a combination therapy of rivaroxaban plus aspirin, as opposed to that of the group with an aspirin-alone regimen [347 patients (4%) versus 460 patients (6%); HR 0.74, 95% CI, 0.65–0.86; p < 0.0001, p value for interaction: 0.47]. The primary outcome of the group with rivaroxaban alone did not decrease significantly [411 patients (5%) versus 460 patients (6%); HR 0.89, 95% CI, 0.78–1.02; p = 0.094]. Compared with aspirin alone, the DPI group showed more major bleeding [263 patients (3%) versus 158 patients (2%); HR, 1.66; 95% CI, 1.37–2.03; p < 0.0001]. There were also more major bleedings with rivaroxaban alone [236 patients (3%) versus 158 patients (2%); HR, 1.51; 95% CI, 1.23–1.84; p < 0.0001]. The most frequent major bleeding site was the gastrointestinal tract. Incidences of intracranial [26 patients (<1%) versus 23 patients (<1%); HR, 1.12; 95% CI, 0.64–1.96; p = 0.69] and fatal bleeding [14 patients (<1%) versus 9 patients (<1%); HR, 1.55; 95% CI, 0.67–3.58; p = 0.30] were not significantly different between groups. Compared with the aspirin-alone group, the DPI group showed a decrease in mortality [262 patients (3%) versus 339 patients (4%); HR, 0.77; 95% CI, 0.65–0.90; p = 0.0012]. 27
Most recently the results of a preplanned substudy evaluating whether a DPI regimen was more effective than aspirin only for preventing graft failure and major adverse CV event (MACE) after coronary artery bypass graft (CABG) surgery (n = 1448) were reported. 28 In fact, patients with recent CABG are at risk for early graft failure, which increases the risk of MI and death. 28 Patients were randomized 4–14 days after CABG. Although DPI was associated with a reduction in MACE compared with aspirin as in the larger COMPASS trial, there were no differences in the primary outcome of graft failure, diagnosed by computed tomography angiogram 1 year after surgery [DPI versus aspirin, 113 (9.1%) versus 91 (8.0%) failed grafts; odds ratio (OR), 1.13; 95% CI, 0.82–1.57; p = 0.45; rivaroxaban alone versus aspirin, 92 (7.8%) versus 92 (8.0%) failed grafts; OR, 0.95; 95% CI, 0.67–1.33; p = 0.75]. There was no fatal bleeding or tamponade within 30 days of randomization. 28
COMPASS PAD subanalysis
A total of 7470 subjects meeting study entry criteria for the PAD cohort (including 1919 carotid artery disease patients) as defined in Table 1 were randomized.25,29 The composite primary endpoint of CV death, MI, or stroke in the DPI group was significantly lower compared with the aspirin-only group [126 patients (5%) versus 174 patients (7%); HR, 0.72; 95% CI, 0.57–0.90; p = 0.0047, p value for interaction, 0.61]. The composite endpoint of major adverse limb events (MALEs; defined as the development of acute or chronic limb ischemia over the course of the trial follow up, including any additional major amputations due to a vascular event that was not included in ALI or chronic limb ischemia) of the extremities, including major amputation, was also decreased in the DPI group compared with that of the aspirin-only group [32 patients (1%) versus 60 patients (2%); HR, 0.54; 95% CI, 0.35–0.82; p = 0.0037]. The rivaroxaban 5 mg bid regimen, compared with that of aspirin alone, did not significantly decrease the composite primary endpoint [149 patients (6%) versus 174 patients (7%); HR, 0.86; 95% CI, 0.69–1.08; p = 0.19]. However, rivaroxaban 5 mg bid showed a decrease in MALE, including major amputation [40 patients (2%) versus 60 patients (2%); HR, 0.67; 95% CI, 0.45–1.00, p = 0.05]. Mortality was not significantly lower with a DPI regimen of rivaroxaban and aspirin compared with aspirin only (HR, 0.91; 95% CI, 0.72–1.16; p = 0.45)
Bleeding outcomes followed a similar pattern as seen in the overall COMPASS trial. The DPI group showed an increase in major bleeding, largely gastrointestinal, in comparison with the aspirin-only group [77 patients (3%) versus 48 patients (2%); HR, 1.61; 95% CI, 1.12–2.31; p = 0.0089]. Likewise, the rivaroxaban 5 mg bid regimen showed more major bleeding [79 patients (3%) versus 48 patients (2%); HR, 1.68; 95% CI, 1.17–2.40; p = 0.0043]. There were no differences in fatal or critical organ bleeding. 29
Another subgroup analysis of the COMPASS trial evaluated outcomes from 6391 patients with only PAD of the lower extremities. The DPI group with rivaroxaban and aspirin not only had fewer MALEs, but also when they occurred they had less severe and fewer complication than in aspirin only group. 30 In particular, a total of 128 patients had MALEs. The cumulative risk of hospitalization following an episode of MALE, was 61.5% (HR, 7.21; p < 0.0001); the risk of vascular amputation, 20.5% (HR, 197.5; p < 0.0001); the risk of death, 8.3% (HR, 3.23; p < 0.001). Compared with an aspirin-alone regimen, the DPI regimen reduced the incidences of MALE by 43% (p = 0.01), total vascular amputation by 58% (p = 0.01), peripheral vascular intervention by 24% (p = 0.03), and all peripheral vascular outcomes by 24% (p = 0.02). 30
Recommendations for clinical practice
Antithrombotic treatment is a key component of secondary prevention following an ACS, particularly among patients undergoing coronary stent implantation.7,15 Indeed, to this extent the use DAPT with aspirin and a P2Y12 inhibitor is the standard of care therapy during the first year after an event. 15 However, the optimal duration of treatment post-ACS remains a topic of ongoing debate.15,18 Indeed, prolonged (e.g. >1 year) DAPT in high-risk patients with a history of MI reduces ischemic events, mainly attributed to a reduction of MI, whereas such benefit is less pronounced among patients who underwent PCI for stable CAD.15,18 However, recent findings show that in patients with stable CAD, two-thirds of whom had a history of MI, DPI with very-low-dose rivaroxaban and aspirin also results in improved ischemic outcomes, including reduced CV mortality. 25 Both strategies are associated with increased bleeding.15,25 However, to date there are no head-to-head comparisons between DAPT versus DPI for such high risk patient population. Therefore, choosing the most appropriate antithrombotic treatment strategy can be challenging, and requires a careful assessment of both the risks of ischemia and bleeding. 31 To this extent, risk scores have been developed to aid in defining the balance between ischemia and bleeding.32–35 An understanding of the trials conducted in this setting and how they are reflective of real-world clinical practice may help in the decision-making process of choosing whether to continue or not with additional antithrombotic therapy and which regimen to choose (DAPT versus DPI). A recent analysis applying inclusion and exclusion criteria of the COMPASS trial to patients with CAD or PAD in the REduction of Atherothrombosis for Continued Health (REACH) registry (n = 31,873) found that 29.9% patients had exclusion criteria and an additional 17.2% did not fulfil the inclusion criteria and thus would not have been eligible for COMPASS. 36 The main reasons for exclusion were high-bleeding risk (51.8%), use of oral anticoagulation (44.8%), requirement for DAPT within 1 year of an ACS or PCI (25.9%), history of ischemic stroke <1 year (12.4%), and severe renal failure (2.2%). As such, a substantial proportion of patients in the REACH registry (52.9%), reflecting a real-world cohort of candidates to secondary and tertiary prevention, would be theoretically eligible to the DPI regimen. Notably, these patients experienced higher annualized primary outcome event rates than patients enrolled in the reference aspirin arm of COMPASS (4.2% versus 2.9% per year, p < 0.001).
The combination of rivaroxaban 2.5 mg bid and low-dose aspirin is approved by the US Food and Drug Administration to reduce the risk of major CV events (CV death, MI, and stroke) in patients with chronic CAD or PAD. 37 Rivaroxaban is contraindicated in patients with active pathological bleeding and severe hypersensitivity reaction to rivaroxaban. 37 The combination of rivaroxaban 2.5 mg bid and low-dose aspirin is approved by the European Medicines Agency for the prevention of atherothrombotic events in adult patients with CAD or symptomatic PAD at high risk of ischemic events. 38 However, the treatment regimen may not be suitable for certain subgroups of patients with increased risk of bleeding, and is not recommended in patients with creatinine clearance <15 ml/min. 38 In addition, contraindications of rivaroxaban include hypersensitivity to the active substance, active clinically significant bleeding, a lesion or condition that is considered a significant risk of major bleeding, concomitant treatment with any other anticoagulants, and hepatic disease associated with coagulopathy and clinically relevant risk of bleeding. 38 In Canada, rivaroxaban 2.5 mg bid, in combination with aspirin, is approved for the prevention of stroke, MI, and CV death, and for the prevention of acute limb ischaemia and mortality in patients with CAD with or without PAD. 39 Contraindications include clinically significant active bleeding (including gastrointestinal bleeding), lesions or conditions at increased risk of clinically significant bleeding (e.g. recent cerebral hemorrhagic or ischaemic infarction), active peptic ulcer disease with recent bleeding, spontaneous or acquired impairment of hemostasis, and hypersensitivity to rivaroxaban. 39 Thus, it is always recommended to assess the risk of bleeding and consider the benefit–risk profile for each individual patient prior to commencing therapy.
From a practical perspective, in patients who are at high risk for bleeding, any additional therapy should be in general avoided. Prolonged DAPT has greater efficacy at reducing recurrent MI and stent thrombosis as opposed to the greater efficacy of DPI at reducing stroke.15–17,25 Indeed, the different mechanisms of action of a P2Y12 inhibitor and rivaroxaban suggest that the former may be more effective at preventing occlusive coronary thrombosis, whereas the latter more effective at preventing cardiac thromboembolism.15–17,25 It cannot be excluded that these therapies have differential effects on vascular inflammation and progression of atherosclerosis. 31
During the first year after an ACS, in the absence of contraindications, the new-generation P2Y12 inhibitors (ticagrelor or prasugrel) are preferred over clopidogrel in ACS patients.13–15 Among patients at high risk for ischemia and low risk for bleeding who tolerate ticagrelor 90 mg bid for a year, de-escalating to ticagrelor 60 mg bid, in addition to aspirin, for an additional 3 years as conducted in the PEGASUS (Prevention of Cardiovascular Events in Patients With Prior Heart Attack Using Ticagrelor Compared to Placebo on a Background of Aspirin) trial is a guideline recommended option. 16 It is important to note that in the PEGASUS trial only patients ⩾50 years who were 1–3 years post-MI were enrolled who also required at least one enrichment factor for atherothrombosis (age ⩾65 years, diabetes mellitus on medication, chronic kidney disease, second prior MI, multivessel CAD); patients with a prior stroke were excluded. 16 These study entry criteria are very different from those of the COMPASS trial (Table 1). However, in those who switched P2Y12 inhibiting therapy during the first year due to nonbleeding side effects (e.g. dyspnea) and have completed their intended course of DAPT, starting rivaroxaban 2.5 mg bid upon completion of 12 months of DAPT can be considered. 40 In stable high-risk CAD patients who have been off DAPT and on aspirin (e.g. remote history of ACS with at least two risk factors such as extensive CAD, diabetes mellitus, PAD, chronic kidney disease, or recurrent MI), the addition of rivaroxaban 2.5 mg bid may also be a treatment option. Although the COMPASS trial showed consistent results across its various subgroups, patients at highest baseline ischemic risk are more likely to derive a greater absolute risk reduction in ischemic events. 25
Further research is needed to compare the two strategies (DAPT versus DPI) and aid with individualizing antithrombotic treatments for secondary prevention. Moreover, defining strategies to reduce the risk of bleeding in patients who can benefit from more aggressive antithrombotic treatment regimens is a topic of ongoing investigation. 41 Although the use of proton-pump inhibitors has already been shown to reduce bleeding in patients treated with a P2Y12 inhibitor and is recommended in patients treated with full-dose oral anticoagulation and antiplatelet therapy, this did not show any significant benefit in patients treated with a DPI regimen.42–44 In particular, in the analysis for the effects of proton-pump inhibitors in the COMPASS trials, compared with placebo pantoprazole 40 mg daily did not reduce upper gastrointestinal events (defined as a composite of overt bleeding, upper gastrointestinal bleeding from a gastroduodenal lesion or of unknown origin, occult bleeding, symptomatic gastroduodenal ulcer or ⩾5 erosions, upper gastrointestinal obstruction, or perforation), although a reduction in bleeding from gastroduodenal lesions was observed. 44
In contrast to patients with CAD, patients with PAD have less antithrombotic treatment options. In fact, for nearly two decades the only evidence of a strategy superior to aspirin in PAD patients was that shown in the CAPRIE (Clopidogrel versus Aspirin in Patients at Risk of Ischemic Events) trial in which clopidogrel monotherapy was associated with a greater reduction in ischemic events compared with aspirin monotherapy in patients with stable vascular disease (CAD, PAD, and cerebrovascular disease), a finding which was driven mostly by the PAD cohort. 45 However, a strategy of more potent P2Y12 inhibition with ticagrelor monotherapy failed to show any benefit over clopidogrel monotherapy. 46 The benefit of a DAPT regimen over single antiplatelet treat in PAD patients is unclear and derive from small subgroup analysis.47,48 Whereas adjunctive treatment with vorapaxar showed a reduction in hospitalization for ALI and peripheral revascularization compared with standard of care therapy (aspirin and/or clopidogrel), this did not significantly reduce the primary composite ischemic endpoint and major bleeding, including intracranial hemorrhage, was increased.20,49 Therefore, a DPI regimen with aspirin and low-dose rivaroxaban showing the most significant CV and limb protection for PAD patients represents a very attractive treatment regimen for these patients, particularly if at low risk of bleeding complications.25,29,30
Conclusion
CAD and PAD patients are at high risk for ischemic recurrences. Despite the utilization of effective secondary prevention strategies, the prevalence of ischemic recurrences remains high, underscoring the need for effective secondary prevention antithrombotic treatment regimens. Most recent findings support the potential role of OAC therapy in addition to antiplatelet therapy to reduce the risk of ischemic recurrences. In particular, the results of the COMPASS trial recently tested the impact of rivaroxaban used at the so-called vascular protection dose in adjunct to aspirin, a strategy known as DPI, for secondary prevention of ischemic recurrences in patients with stable CAD and PAD manifestations. In particular, compared with aspirin monotherapy, such DPI regimen was associated with a significant reduction in MACEs, including CV mortality, in the overall population. Moreover, a reduction in MALEs was observed in patients with PAD. Such benefit occurred at the expense of increased bleeding. However, the net clinical benefit was still in favor of DPI which now represents an approved regimen for secondary prevention in CAD and PAD patients.
Footnotes
Conflict of interest statement
S.W.C. does not have any disclosures to report. F.F. declares consulting fees or honoraria from AstraZeneca and Sanofi. D.J.A. declares that he has received consulting fees or honoraria from Amgen, Aralez, AstraZeneca, Bayer, Biosensors, Boehringer Ingelheim, Bristol-Myers Squibb, Chiesi, Daiichi-Sankyo, Eli Lilly, Haemonetics, Janssen, Merck, PLx Pharma, Pfizer, Sanofi, and The Medicines Company and has received payments for participation in review activities from CeloNova and St Jude Medical. D.J.A. also declares that his institution has received research grants from Amgen, AstraZeneca, Bayer, Biosensors, CeloNova, CSL Behring, Daiichi-Sankyo, Eisai, Eli Lilly, Gilead, Idorsia, Janssen, Matsutani Chemical Industry Co., Merck, Novartis, Osprey Medical, and Renal Guard Solutions.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.