
Abstract
Objective
This study aimed to investigate whether differential expression of the retinoic acid receptor-related orphan receptor A (RORA) gene is related to occurrence of acute myocardial infarction (AMI).
Methods
This was a retrospective study. White blood cells of 93 patients with acute myocardial infarction and 74 patients with stable coronary artery disease were collected. Reverse transcription quantitative polymerase chain reaction and western blotting were used to measure RORA mRNA and protein expression, respectively.
Results
RORA mRNA expression levels in peripheral blood leukocytes in patients with AMI were 1.57 times higher than those in patients with stable coronary artery disease. Protein RORA levels in peripheral blood of patients with AMI were increased. Binary logistic regression analysis showed that high expression of RORA was an independent risk factor for AMI, and it increased the risk of AMI by 2.990 times.
Conclusion
RORA expression levels in patients with AMI is significantly higher than that in patients with stable coronary artery disease. High expression of RORA is related to AMI and it may be an independent risk factor for AMI.
Keywords
Introduction
The prevalence of cardiovascular disease in China is still increasing, which is similar to the international prevalence of acute myocardial infarction (AMI), and consistent with China’s cardiovascular disease report in 2017. This increase accounts for more than 40% of deaths of residents and 11 million patients with coronary artery disease. 1 Among them, AMI is a serious consequence of coronary atherosclerotic heart disease, 2 with high morbidity and mortality in cardiovascular disease,3,4 and nearly half of patients with cardiovascular disease die of AMI. 5
The first symptom of AMI is chest pain, which is not relieved for a long time. In the USA, a study reported that the first symptom of AMI in approximately 7 million people/year was acute chest pain. 6 Assessment and classification of these patients is complex, and only a small percentage of patients with acute chest pain are ultimately diagnosed with AMI. The differential diagnosis of patients with AMI depends almost entirely on determination of cardiac troponin I or cardiac troponin T levels. 7
A combination of genetic and environmental factors increases the risk of atherosclerosis. Whether there is a genetic factor for progression of stable coronary artery disease (SCAD) to AMI, in addition to the traditional risk of atherosclerosis, is unclear. SCAD and AMI have similar causes of the disease, which is atherosclerosis, and SCAD occurs at different stages of the same disease.8,9
Differential expression of genes in peripheral blood leukocytes can provide information on dynamic changes in disease status and predict the likelihood of cardiovascular events more accurately than existing technologies. 10 A change in gene expression in peripheral blood leukocytes is an indicator of the sensitivity and specificity of coronary artery disease. 11 Ikonomidis et al. 12 showed that increased expression of genes and proteins in peripheral blood leukocytes was associated with progression of coronary atherosclerosis. There is also evidence that peripheral white blood cells can be used as a window for evaluating disease. 13 Moreover, peripheral blood leukocytes are easy to obtain and to detect.
Our previous gene chip study showed that retinoic acid receptor-related orphan receptor A (RORA) gene expression was higher in white blood cells in the AMI group compared with the SCAD group. 14 Therefore, this study aimed to determine whether high expression of the RORA gene in peripheral blood leukocytes is related to AMI.
Methods
Patients
This was a retrospective study that meets the ethical standards set by the Declaration of Helsinki. All details of the patients were de-identified. All patients signed informed consent and agreed to treatment. The study was approved by the ethics committee of The Third Hospital of Jilin University (No. 2016-wjw013). All patients involved in the study signed a written informed consent form. Patients with AMI who were hospitalized in the Department of Cardiovascular Medicine in the Third Hospital of Jilin University from February 2018 to May 2018 were randomly selected as the AMI group and patients with SCAD were selected as the control group. The medical history, plasma triglyceride levels, total cholesterol levels, high-density lipoprotein levels, low-density lipoprotein levels, a biochemical examination, smoking history, diabetes history, and other relevant clinical data were recorded in detail. The diagnosis of AMI was based on the latest guidelines on AMI issued by the European Society of Cardiology in 2017 15 and met the criterion of clear vascular lesions confirmed by coronary angiography. 16 Patients with severe stenosis or occlusion (>75% of the vessels were stenosed with corresponding symptoms) of the main coronary artery branch (e.g., left main trunk, right main trunk) and main branches (e.g., left circumflex, anterior descending branch) were in the AMI group.
The exclusion criteria for AMI were as follows: (1) myocardial infarction associated with percutaneous coronary intervention or coronary artery bypass grafting; (2) secondary myocardial infarction that was related to an increase in catecholamine levels, or imbalance of blood supply and demand, or myocardial infarction caused by coronary artery spasm; and (3) myocardial infarction with cardiac surgery or non-cardiac surgery.
The inclusion criteria for SCAD met the Canadian Society of Cardiovascular Disease’s grade 4 criteria for defining SCAD as follows. In grade I, general physical activity (e.g., walking and climbing stairs) is not limited, but angina occurs during strong, fast, or sustained exertion. In grade II, general physical activity is slightly limited. Angina attacks during brisk steps, after meals, in cold or windy conditions, during mental stress, or within hours of waking up. Generally, physical activity is restricted to walking more than 200 m or climbing a flight of stairs. In grade III, general physical activity is significantly limited. Generally, walking within 200 m or climbing a flight of stairs causes angina pectoris. In grade IV, angina pectoris can occur with mild activity or rest.
In the SCAD group, patients with SCAD received resting thoracic echocardiography to exclude heart thrombosis and heart failure. Exclusion criteria in the SCAD group were as follows: (1) multiple factors or uncertain myocardial damage caused by uncertain diseases, such as severe heart failure, stress cardiomyopathy, severe pulmonary embolism or pulmonary hypertension, septicemia, critical disease, renal failure, and serious mental system diseases (e.g., stroke and subarachnoid hemorrhage); (2) immune system diseases and/or hormone use; (3) history (active or potential) or evidence of chronic or recurrent tuberculosis; and (4) serious infectious diseases, complications of malignant tumors, or suspected or confirmed immunodeficiency.
Obtaining peripheral blood lymphocytes
At 6 am, 6 mL of fasting peripheral blood from patients with SCAD was extracted into EDTA anticoagulant tubes, stored at 4°C, and lymphocytes were extracted within 4 hours after collecting samples. A volume of 6 mL of peripheral blood was collected within 20 minutes after patients with AMI were admitted to hospital, stored at 4°C, and lymphocytes were extracted within 4 hours. The reagent used was peripheral blood lymphocyte separation fluid. The detailed steps were as follows. 1) Fresh anticoagulant blood was mixed with 0.9% sodium chloride injection. 2) The mixture was carefully added to human peripheral blood lymphocyte separation fluid of the same volume and centrifuged at 1000 × g for 20 minutes. 3) After centrifugation, the fluid was divided into four layers from top to bottom, including the plasma layer, the milky white lymphocyte layer, the transparent separation fluid layer, and the red blood cell layer. The lymphocyte layer was sucked out and was used for subsequent experiments.
Synthesizing peripheral blood lymphocyte cDNA
Total RNA was extracted from lymphocytes using a total RNA extraction kit (Tiangen Biotech Company, Beijing, China). The extraction process was conducted in strict accordance with the kit instructions to avoid degradation or contamination of RNA. The obtained RNA solution was used for quality detection of RNA by polyacrylamide gel electrophoresis. The 28S and 18S rRNA bands were observed, and the 28S rRNA bands were approximately twice as bright as the 18S rRNA bands. The concentration and absorbance of samples meeting the standards were determined by an enzyme marker. The 260/280 ratio was 1.7 to 2.1 and the value of A260/A230 was >2. Reverse transcription was performed after meeting the requirements of the reverse transcription kit. According to the instructions of the reverse transcription kit, the total RNA that met the experimental requirements was reverse transcribed. The concentration of the RNA in each sample was consistent. The obtained cDNA samples were kept at −80°C for further detection by quantitative fluorescence polymerase chain reaction (PCR). This process was carried out on an ultraclean table and attention was paid to avoid contamination.
Real-time quantitative PCR
After the cDNA sample was diluted by 20 times, SYBR fluorescence quantitative reagent (Sangong Biotech Company, Shanghai, China) was used for PCR amplification. The reaction conditions were as follows: pre-denaturation at 95°C for 5 minutes; denaturation at 95°C for 3 s, annealing at 60°C for 30 s, and extension at 72°C for 20 s for 40 cycles; and dissociation and amplification curves at 95°C for 15 s, 60°C for 1 minute, and 95°C for 15 s. Glyceraldehyde-3-phosphate dehydrogenase was used as the internal reference gene and RORA was used as the target gene. The specificity of amplification conditions was determined according to the dissociation curve of software attached to the ABI-FAST7500 instrument (Applied Biosystems, Singapore). The PCR primer sequences used are shown in Table 1.
Primer sequence of real-time polymerase chain reaction.

Fa, upstream primer; Rb, downstream primer.
RORA, retinoic acid receptor-related orphan receptor A; GAPDH, glyceraldehyde-3-phosphate dehydrogenase.
Western blot analysis
According to the diagnostic requirements of AMI and SCAD as described above, two patients with AMI and two patients with SCAD were selected for western blot analysis. After collecting leukocytes in peripheral blood of the patients by radioimmune precipitation buffer, the supernatant was centrifuged and placed in a water bath at 98°C for 10 minutes. Next, 5× loading buffer was added, and the loading amount was 30 μg protein. The internal voltage of concentrated adhesive was 60 V. When the band pressed into a line and reached the junction of concentrated adhesive and separated adhesive, the voltage was adjusted to 110 V until the end of electrophoresis. According to BD semi-dry instructions (Becton-Dickinson Company, Franklin Lakes, NJ, USA), the protein was transferred to a polyvinylidenefluoride membrane and cultured overnight with the first RORA antibody (Omnimabs, Inc., Upland, CA, USA) at 4°C. The membrane was then incubated at room temperature with the second antibody for 2 hours, and analyzed using a chemiluminescence imaging system (Omnimabs, Inc.). Experiments were repeated three times and averaged.
Statistical analysis
IBM SPSS 24.0 software (IBM Corp., Armonk, NY, USA) was used for statistical analysis. Measurement data were normally distributed and data are shown as mean ± standard deviation. The inter-group differences were compared and analyzed by the independent t test. The rank sum test was used for inter-group differences of data shown as median and quartile range. Count data were analyzed by frequency and differences between groups was analyzed by the χ2 test. P<0.05 was considered to be statistically significant. Multivariate logistic regression analysis was used to analyze the correlations between age, RORA gene expression, and AMI.
Results
Basic characteristics
There were 93 patients in the AMI group and 74 patients in the control group. There were no significant differences in sex, history of hypertension, history of smoking, and levels of serum triglycerides, serum total cholesterol, low-density lipoprotein cholesterol, and high-density lipoprotein cholesterol between the groups. However, patients in the AMI group were significantly older than those in the SCAD group (P=0.031) (Table 2).
Baseline data of the patients.
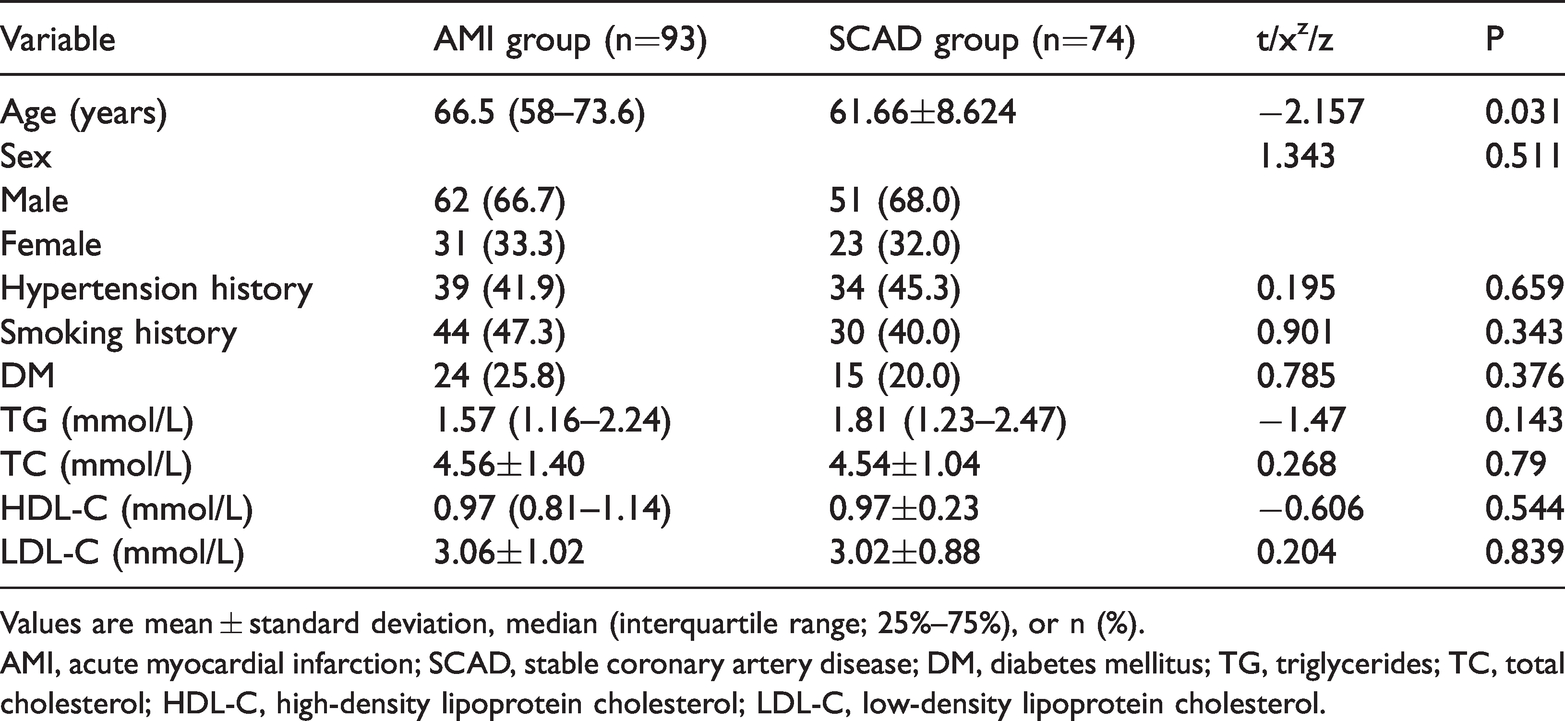
Values are mean ± standard deviation, median (interquartile range; 25%–75%), or n (%).
AMI, acute myocardial infarction; SCAD, stable coronary artery disease; DM, diabetes mellitus; TG, triglycerides; TC, total cholesterol; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol.
RORA mRNA expression levels in peripheral blood leukocytes
The amplification curves of the internal reference gene and the target gene were remarkably smooth (“S type”) and the dissociation curves were all single peaks without multiple wave peaks. This indicated that the amplification primer had strong specificity and appropriate reaction conditions. No non-specific amplification occurred (Figure 1). The results obtained by real-time PCR were repeated three times for each sample and the standard deviation was consistent with the requirements of real-time PCR. We found that the 2−△Ct in the AMI group was significantly higher (0.622, 0.233–1.157) than that in the SCAD group (0.396, 0.0786–0.753) (P<0.05). Relative RORA expression level in patients with AMI was 1.57 times higher than that in the SCAD group (Figure 2).

Dissociation and amplification curves of real-time polymerase chain reaction. (a) Dissociation curve of the target gene; (b) amplification curve of the target gene. The amplification and dissolution curves only represent the trend. The graphs are randomly selected images intended to be representative of all real-time polymerase chain reaction experiments.

Relative expression of RORA mRNA expression levels.
RORA protein levels in peripheral blood leukocytes
β-actin was used as a reference gene to detect protein levels in peripheral blood leukocytes of patients. Western blot analysis showed that RORA protein expression in peripheral blood leukocytes in the AMI group were higher than those in patients with SCAD (Figures 3 and 4).

Comparison of RORA protein expression levels between the groups. In the first western blot experiment, sample 1 was from a patient in the AMI group, and samples 2 and 3 were from patients in the SCAD group. In the second western blot experiment, sample 4 was from a patient in the AMI group, and samples 5 and 6 were from patients in the SCAD group. First, second, and third indicate three separate western blot experiments.
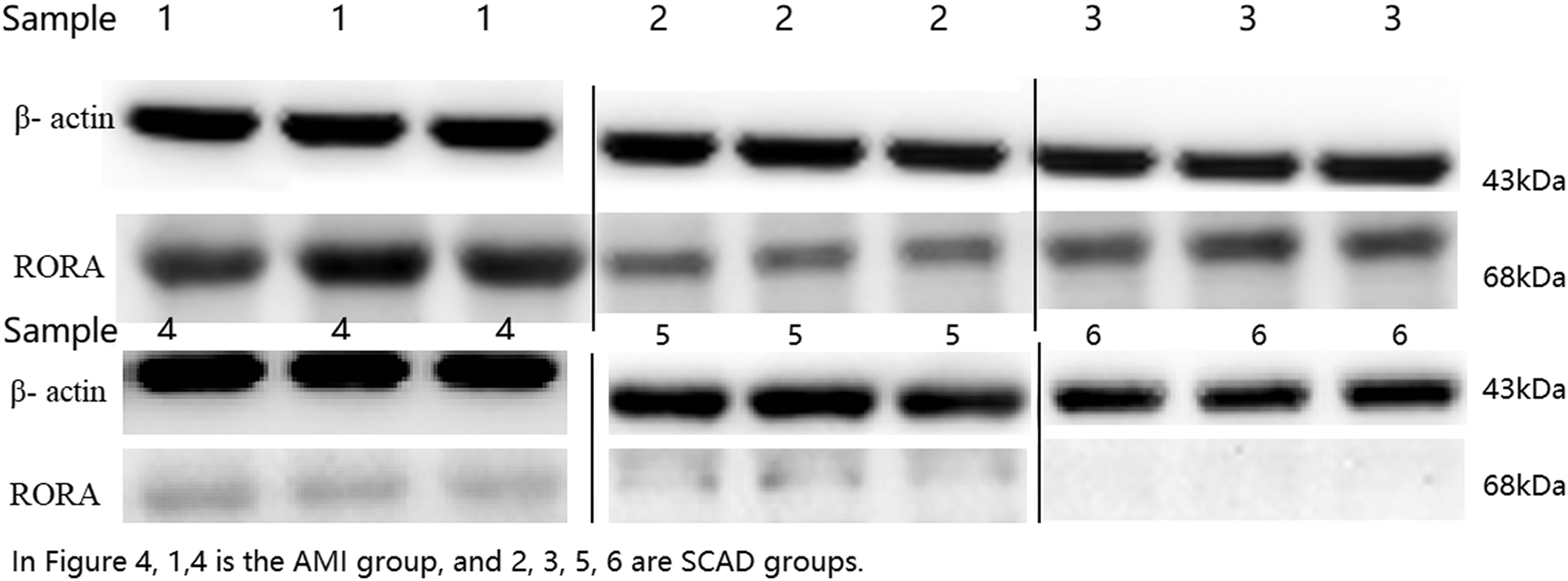
Western blot of some samples from each group. Relative expression of RORA was based on actual calculation, and the internal reference protein and the target protein were compared at the same time. Each specimen was measured three times. Samples 1 and 4 were from the AMI group, and samples 2, 3, 5, and 6 were from the SCAD group.
Univariate logistic regression analysis of AMI
Smoking, diabetes, and hyperlipidemia increased the incidence of AMI by 1.347, 1.391, and 1.591 times, respectively (Table 3).
Univariate regression analysis of smoking, diabetes, and total cholesterol related to acute myocardial infarction.

B, unstandardized beta; SE, standard error; P, probability value; Exp(B), exponent of B.
Correlation analysis between relative RORA expression levels and age
RORA mRNA expression levels and age of the patients were different in the AMI and SCAD groups. To further analyze whether RORA mRNA expression levels are related to the patient’s age, all patients were divided into an older group (>65 years) and a younger group (≤65 years) according to their age. 17 On the basis of the cut-off value, mRNA expression levels in each patient were divided into the high expression and low expression groups, and the correlation between age and RORA expression levels in each group were compared. We found no difference in RORA mRNA expression levels between the older and younger groups (Table 4).
Relative expression of RORA by age.

RORA, retinoic acid receptor-related orphan receptor A.
Multivariate logistic regression analysis of correlations between age, RORA expression, and AMI
Based on the correlation between RORA expression and AMI, the maximum value of sensitivity and specificity was taken as the cut-off value, which was 0.958. All patients were divided into the high expression group (2−△Ct ≥0.958) and the low expression group (2−△Ct <0.958) on the basis of the cut-off value of RORA expression. We found that an older age of patients in this study was not related to the occurrence of AMI, and high RORA expression increased the risk of AMI by 2.990 times (P=0.004, Table 5).
Logistic regression analysis of RORA mRNA expression levels and acute myocardial infarction.

RORA, retinoic acid receptor-related orphan receptor A; B, unstandardized beta; SE, standard error; P, probability value; OR, odds ratio; CI, confidence interval.
Discussion
In this study of patients with AMI and those with SCAD, we found the following main findings. Patients in the AMI group were older than those in the SCAD group, and an increase in age was a risk factor for AMI. However, increased gene expression was not associated with increased age. High RORA gene expression nearly tripled the risk of AMI.
The RORA-encoded protein, which is a member of the nuclear receptor (NR) 1 subfamily of nuclear hormone receptors, acts as a monomer or homodimer that binds to hormone response elements upstream of several genes to enhance expression of these genes. 18 NR is a member of the DNA-binding transcription factor family and it regulates a variety of functions, such as homeostasis, reproduction, development, and metabolism. Depending on the different mechanism of action or function, the NR super family is divided into seven types as follows: NR1 (thyroid hormone-like), NR2 (liver cell nucleus factor IV analogue-like), NR3 (estrogen-like), NR4 (nerve growth factor-like), NR5 (fushi tarazu-F1-like), NR6 (germ cell factor-like), and NR0 (with collaborative features). 19
Leukocytes and type 2 cytokines are involved in the processes of inflammation. Cytokines are derived from T helper-2 (Th2) cells and group 2 innate lymph (ilc2) cells. The Th2 response is derived from interleukin-13 produced by ilc2, while ilc2 cells are derived from normal lymphoid progenitor cells, and their growth depends on RORA. 20 AMI is an inflammatory disease. Inflammation increases the incidence of complications of AMI and increases the mortality rate of patients. 21 The inflammatory response of AMI is a key factor in determining the size of myocardial infarction. A continuous inflammatory response can lead to left ventricular remodeling after myocardial infarction, making inflammation an important therapeutic target to improve the prognosis of AMI. 22
Increased RORA gene expression leads to hypothyroidism in rats. RORA is widely expressed in the heart, lungs, liver, and peripheral blood leukocytes. 23 Studies have shown that unstable release of thyroid hormone and a decrease in thyroid hormone production can cause the left ventricular cavity to become smaller through thickening of the left ventricular wall, and strengthening contraction of the atria and ventricles, thus leading to occurrence of AMI. 24 The main function of RORA is to encode NR1 (thyroid hormone) and regulate the circadian rhythm. The circadian rhythm is important for the body to maintain a healthy state. More importantly, RORA has been shown to facilitate transcriptional regulation of some genes involved in the circadian rhythm. 25 One factor regulating the circadian rhythm is thyroid hormones. 26 Hypothyroidism leads to hyperlipidemia, vascular inflammation, and aggravation of heart remodeling, which leads to occurrence and poor prognosis of AMI.27–31 RORA indirectly causes thyroid hormone secretion disorders or decreases thyroid hormone secretion by controlling encoding of NR1. 32 Additionally, uneven distribution of unstable thyroxine and thyroid hormone in the body directly causes an imbalance of the circadian rhythm, which leads to occurrence of AMI in patients with SCAD. 33 Therefore, RORA might affect the circadian rhythm by affecting thyroid function, which ultimately leads to AMI. 34
Atherosclerosis cause SCAD and AMI. Atherosclerosis is a dynamic process, and the degree of stenosis gradually progresses with an increase in age. The risk of AMI increases with age, regardless of whether SCAD is present. Our study also showed that patients in the AMI group were older than those in the SCAD (controls) group. An increase in age is a risk factor for progression of SCAD to AMI. A 17-year study in the USA showed that 1448 of 5258 cases of AMI occurred, and concluded that age was a risk factor and it was an important risk factor for recurrent AMI. 35 A 15-year study in Sweden showed that 283,014 patients had AMI and that patients older than 75 years were at greater risk. 36
This study has some limitations. This was a retrospective study without measurement of thyroid hormones and observation of the circadian rhythm. Clarifying how RORA participates in release of thyroid hormones and how it affects the circadian rhythm by prospective studies is required. The causal relationship between RORA gene overexpression and AMI needs to be proven by prospective studies.
Conclusion
RORA gene expression levels in patients with AMI are significantly higher than those in patients with SCAD. High RORA gene expression is related to AMI and it may be an independent risk factor of AMI.
Footnotes
Availability of data and materials
Acknowledgment
We thank Shenyang Huibai Company for its support for western blot experiments in this study.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research was funded by the Health Commission of Jilin Province in 2018 (Project number: 2018SCZ008). All funding bodies were not involved in the study design, data collection, analysis and interpretation of data, or writing of the manuscript.
Author contributions
Conceptualization: HM and FM; data curation: HM and LL; formal analysis: HM, XT, JR, and FM; funding acquisition: FM; investigation: HM, JR, and XT; methodology: XW and FM; project administration: FM; resources: WC; software: FM. All authors have read and approved the manuscript.