
Abstract
Diffuse large B-cell lymphoma (DLBCL) with co-expression of MYC and BCL2 protein by immunohistochemistry (IHC) – that is, double-expresser lymphoma (DEL) – is associated with poor outcomes after standard frontline therapy. Less is known about the prognostic impact of DEL in patients with relapsed/refractory disease treated with salvage therapy and autologous stem cell transplantation (ASCT). We analyzed the outcomes of 167 patients with relapsed/refractory DLBCL treated with R-ICE (rituximab, ifosfamide, carboplatin and etoposide), of whom 111 patients (66%) underwent ASCT. Using predefined cutoffs for positivity by IHC at relapse for MYC and BCL2 of ⩾40% and ⩾50% of positive tumor cells, respectively, 26 patients (16%) were categorized as DEL and the rest as non-DEL. Overall and complete response rates to R-ICE did not differ between DEL and non-DEL. With a median follow up of 20 months, the 3-year progression-free survival (PFS) and overall survival (OS) rates for DEL were inferior compared to non-DEL (for PFS: 6% versus 33%, p = 0.044, for OS: 39% versus 56%, p = 0.03). The negative impact of DEL on PFS and OS remained significant on multivariable analysis. In conclusion, positive DEL status predicts poorer outcomes following salvage therapy.
Introduction
Diffuse large B-cell lymphoma (DLBCL) with co-expression of MYC and BCL2 protein by immunohistochemistry (IHC) (i.e. double-expresser lymphoma, DEL) and/or rearrangements of MYC and BCL2 or BCL6 genes (i.e. double-hit lymphoma, DHL) is associated with poor outcomes after standard frontline therapy, independent of other clinical risk factors.1–4 Less is documented concerning the impact of these genetic events in relapsed/refractory disease. R-ICE (rituximab, ifosfamide, carboplatin and etoposide) is an active regimen for patients with relapsed/refractory DLBCL and can effectively mobilize hematopoietic progenitor cells for subsequent autologous stem cell transplantation (ASCT). 5 R-ICE followed by ASCT is a common salvage approach for medically fit patients with relapsed/refractory DLBCL. In this study, we investigated the prognostic impact of DEL in the salvage setting by analyzing outcomes of patients with relapsed/refractory disease treated with R-ICE prior to planned ASCT.
Patients and methods
We reviewed records of 204 consecutive patients with DLBCL treated with salvage R-ICE and intent for ASCT from 2000 to 2015 at the Taussig Cancer Institute of the Cleveland Clinic. A total of 37 patients were excluded for inadequate clinical data and/or follow up. Data were collected from the electronic medical record with IRB approval.
Experienced pathologists confirmed all histological diagnoses using the World Health Organization classification. 6 Repeat staining was not done at the time of analysis. IHC assays for MYC (Clone Y69 Abcam Epitomics 1:50 dilution) and BCL2 (predominantly Clone 214 Cell Marque) were performed on sections of formalin-fixed, paraffin-embedded tissue collected at the time of relapse. MYC and BCL2 IHC were available for all patients included in this analysis (n = 167). Information on the type of BCL2 antibody used was unknown for 21 cases, which were outside slide reviews. For these cases, quality of staining was adequate based on internal control cells such as reactive T-cells. Predefined cutoffs for positivity by IHC at relapse for MYC and BCL2 were ⩾40% and ⩾50% of positive tumor cells, respectively.1,3 Fluorescence in-situ hybridization (FISH) studies for rearrangements involving BCL2 were available for 35 cases and were performed using dual-color, break-apart probes in 25 cases (Abbott Molecular, Des Plaines, IL) and dual-color dual-fusion probes in 9 cases (Abbott Molecular Inc.). The methodology was unknown in 1 case. FISH studies for rearrangements involving MYC were available for 36 cases and were performed using dual-color, break-apart probes for 32 cases and tri-color, dual-fusion probes for 3 cases. The methodology was unknown for 1 case.
Statistical analysis
Clinical and pathologic characteristics were compared between DEL and non-DEL with the Chi-square test. ASCT was compared using the Gray test. Determination of complete response (CR) or partial response (PR) were adjudicated by clinical criteria. Progression-free survival (PFS) and overall survival (OS) were calculated relative to the start of salvage therapy. Events corresponding to PFS were clinical relapse or death after R-ICE. PFS and OS were estimated by the Kaplan–Meier method and compared between DEL and non-DEL with the log-rank test. Prognostic factors for PFS and OS were assessed with Cox proportional hazards analysis. Results are summarized as the hazard ratio (HR) and 95% confidence interval (CI). All statistical tests were two-sided and a p value <0.05 was considered significant. All statistical analyses were performed using SAS® software (SAS Institute Inc., Cary, NC, USA).
Results
Patient demographics and clinical characteristics are summarized in Table 1. For the entire cohort, the median age at time of starting salvage therapy was 60 years (range 21–86). Most patients had de novo DLBCL (75%), presented without B symptoms (76%), had Internal Prognostic Index (IPI) risk scores 0–2 (64%), and had advanced-stage disease (69% stage III–IV). A majority (93%) received frontline R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine and prednisone) or R-EPOCH (rituximab, etoposide, prednisone, vincristine, cyclophosphamide and doxorubicin). Only eight patients (5%) did not receive rituximab, either as monotherapy or in combination therapy, prior to first relapse.
Patient demographics and clinico-pathologic characteristics at time of salvage therapy.
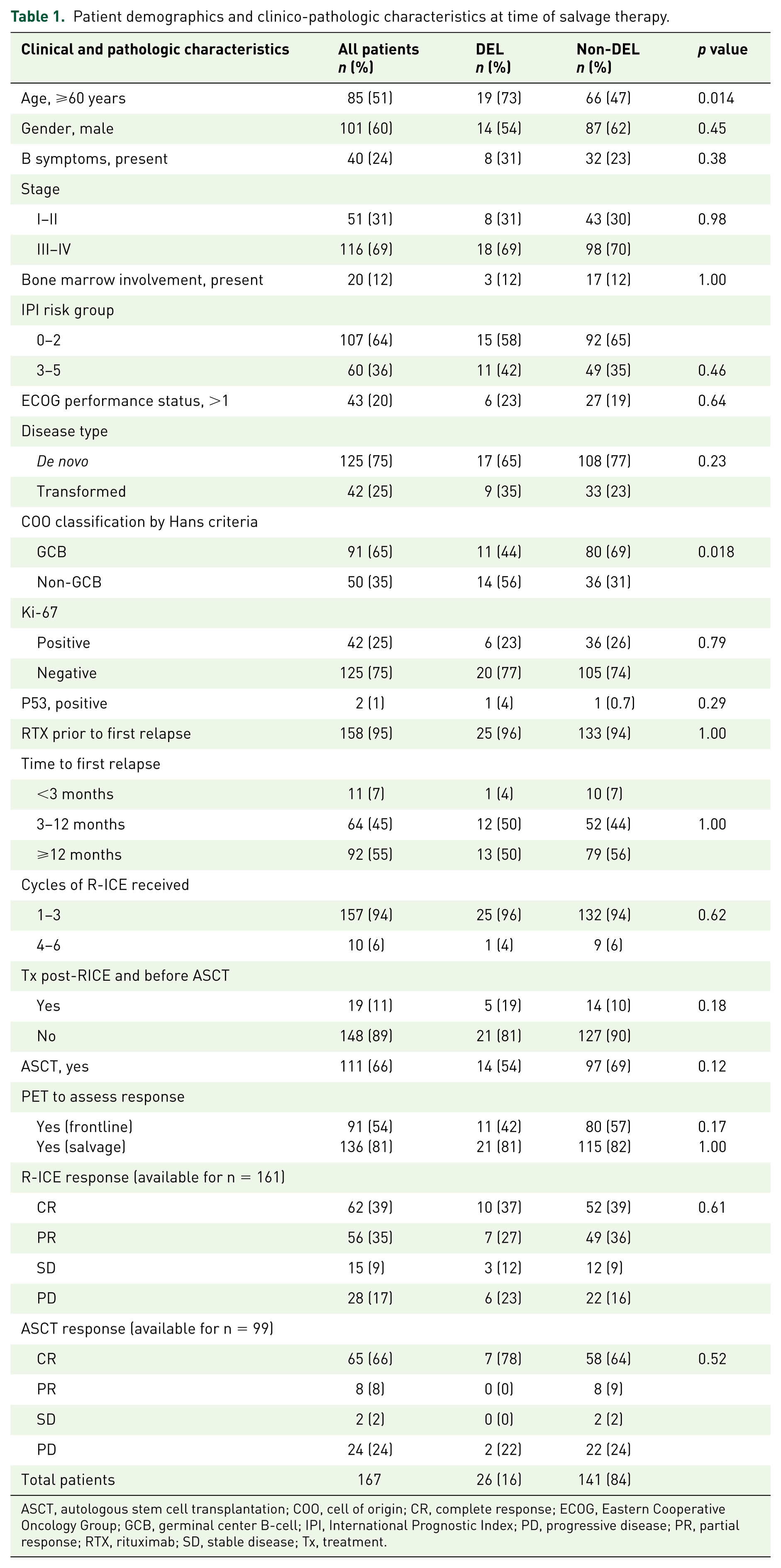
ASCT, autologous stem cell transplantation; COO, cell of origin; CR, complete response; ECOG, Eastern Cooperative Oncology Group; GCB, germinal center B-cell; IPI, International Prognostic Index; PD, progressive disease; PR, partial response; RTX, rituximab; SD, stable disease; Tx, treatment.
Of 167 cases, 26 (16%) were categorized as DEL while the rest (n = 141) were categorized as non-DEL (75 BCL2+/MYC–, 8 BCL2–/MYC+, 58 BCL2–/MYC–). Four patients (2%) had DHL, and 4 (2%) had both DEL and DHL. Patients with DEL were older [median age 66 years (range 35–82 years) versus 58 years (range 21–78 years), p = 0.009] and more likely to have a non-germinal center B-cell subtype (56% versus 31%, p = 0.018), as defined by the Hans criteria. 7
The time from initial diagnosis to beginning of salvage R-ICE was similar between DEL and non-DEL patients [median 12 months (range 0.9–212 months) versus 14 months (range 2–197 months), respectively, p = 0.92]. A total of 157 patients (94%) received 1–3 cycles. Ten patients (6%) received 4–6 cycles as an alternative to ASCT due to patient refusal of ASCT, advanced age (>70 years) or reduced functional and/or mental capacity. PET imaging was used to assess response to R-ICE for a majority (81%) of patients. Objective response rate (ORR) to salvage R-ICE was 74% (39% CR and 35% PR). Nineteen patients (11%) received additional therapy following R-ICE with the intent of proceeding to ASCT. Most patients received consolidative ASCT (n = 111, 66%), of whom 99 were evaluable for response. The ORR was 74% (CR in 66% and PR in 8%). Median follow up was 20 months (range 0.3–174 months).
The ORR was similar between patients with DEL and non-DEL (64% and 75%, respectively, p = 0.61), with no difference in CR rate (37% versus 39%). Patients with DEL had significantly inferior 3-year PFS (6% versus 33%, p = 0.044) compared with patients with non-DEL (Figure 1). In univariate analysis, positive DEL status (HR 1.65, CI 1.01–2.70, p = 0.047) along with shorter time from initial diagnosis (HR 0.90, CI 0.83–0.98, p = 0.019) and higher IPI risk score (HR 1.82, CI 1.22–2.70, p = 0.003) predicted an inferior PFS. These values retained significance in multivariate analysis (Table 2): positive DEL status (HR 1.86, CI 1.09–3.17, p = 0.024), shorter time from initial diagnosis (HR 0.90, CI 0.81–0.99, p = 0.038) and higher IPI risk score (HR 1.58, CI 1.02–2.47, p = 0.042).

Kaplan–Meier estimation of PFS, DEL versus non-DEL, after salvage R-ICE +/– ASCT.
Multivariate analysis of the effect of different factors on outcome.

CI, confidence interval; COO, cell of origin; DEL, double-expresser lymphoma; GCB, germinal center B-cell; IPI, Internal Prognostic Index.
Eight levels were identified based on 6-month intervals (level 1 was <6 months, level 8 was ⩾42 months). This variable was not included in the multivariate analysis for overall survival due to low number of total events.
OS was also inferior in patients with DEL (median OS of 11 months versus 63 months, 3-year OS of 39% versus 56%, p = 0.03) compared with patients with non-DEL (Figure 2). In univariate analysis, de novo DLBCL (HR 1.95, CI 1.04–3.63, p = 0.036), higher-risk IPI score (HR 2.38, CI 1.48–3.83, p < 0.001), and ECOG performance status 2–3 (HR 2.04, CI 1.19–3.50, p = 0.010) were prognostic for inferior OS. Although DEL patients were older than non-DEL patients, age was not prognostic in univariate analysis (HR 1.12, CI 0.90–1.39, p = 0.32). Multivariate analysis (Table 2) demonstrated that the poorer OS of DEL patients remained significant regardless of DLBCL subtype (HR 2.23, CI 1.18–4.21, p = 0.013 with subtype versus HR 1.98, CI 1.09–3.60, p = 0.025 without subtype). No difference in OS was observed between DHL and non-DHL groups (p = 0.83), likely due to the small number of DHL cases.

Kaplan–Meier estimation of OS, DEL versus non-DEL, after salvage R-ICE +/− ASCT.
Discussion
The findings of our study suggest that the negative prognostic effect of DEL carries into the salvage setting, as co-expression of MYC and BCL2 was associated with inferior 3-year PFS and OS after R-ICE with or without consolidative ASCT. Recently, in a study by Bosch and colleagues of patients treated on a prospective clinical trial with GDP (+/− R) (gemcitabine, dexamethasone and cisplatin +/− rituximab) or DHAP (+/− R) (dexamethasone, high-dose cytarabine and cisplatin +/− rituximab), each followed by ASCT, 91 patients had samples available for IHC. Similar to our study, the ORR to salvage therapy was not significantly different between patients with DEL or non-DEL (p = 0.51). Patients with DEL had significantly worse 3-year event-free survival (0% versus 40%, p = 0.001) and OS rates (20% versus 54%, p = 0.004). 8 Miura and colleagues 9 reported similar inferior outcomes for patients with relapsed/refractory aggressive B-cell lymphomas based on DEL status. This study evaluated 38 patients following salvage R-IVAD (rituximab, ifosfamide, etoposide, cytarabine and dexamethasone) and found a lower ORR (35% versus 71%, p = 0.048) and CR (35% versus 71%, p = 0.048) as well as a significantly lower 2-year PFS (9% versus 67%, p = 0.001) and OS (35% versus 71%, p = 0.037) when comparing DEL to non-DEL patients.
Consolidative ASCT for patients with relapsed/refractory DLBCL who achieve CR or PR with second-line chemotherapy may be curative.10–12 Notably, Herrera and colleagues 13 reported an inferior 4-year PFS (37% versus 52%, p = 0.001) when comparing DEL to non-DEL patients with relapsed/refractory DLBCL following ASCT, regardless of remission status. Following consolidative ASCT, our study found no difference in CR for DEL and non-DEL patients (78% versus 64%, p = 0.52), yet 3-year PFS and OS were significantly worse for DEL patients. This suggests the need for improved pre-ASCT cytoreduction and/or post-ASCT consolidation strategies.14–16
A limitation of this study is the small number of patients with available FISH data. The findings of this study, therefore, cannot suggest salvage outcomes for patients with DHL or both DHL and DEL. Additionally, our series had a slightly lower DEL rate (16%) than other reports, suggesting institutional differences in the application of IHC cutoffs.
Conclusion
While second-line immunochemotherapy followed by consolidative ASCT may benefit some patients with relapsed/refractory DLBCL, positive DEL status appears to predict poorer outcomes following salvage therapy. These findings suggest alternate treatments such as those targeting BCL2 and/or MYC may be rational therapeutic strategies to test as a way of potentially improving outcomes for patients with relapsed/refractory DLBCL.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Conflict of interest statement
Joshua Allen: No competing interests. Ana Lucia Ruano Mendez: No competing interests. Lisa Rybicki: No competing interests. Yazeed Sawalha: No competing interests. Deepa Jagadeesh: Celgene advisory board. Robert Dean: No competing interests. Brad Pohlman: No competing interests. Mitchell R. Smith: No competing interests. Eric D. Hsi: Research support for Eli Lilly, Abbvie, and Cellerant Therapeutics; honorarium for HTG molecular diagnostics and Seattle Genetics. Brian T. Hill: Research funding from Genentech.