
Abstract
Factor VIII (FVIII) replacement therapy is the foundation of treatment in hemophilia A and is effective unless a patient develops an alloantibody (inhibitor) against exogenous FVIII. Inhibitor development is currently the most significant treatment complication seen in patients with hemophilia and is associated with considerable morbidity and a decreased quality of life. The development of an inhibitor is the result of a complex interaction between a patient’s immune system and genetic and environmental risk factors. The mainstay of treatment is the eradication of the inhibitor through immune tolerance. This review summarizes the current evidence regarding inhibitor risk factors, eradication, and hemostatic bypassing agents.
Introduction
Hemophilia A is the most common congenital severe bleeding disorder and is the result of a deficiency in the clotting protein factor VIII. Factor VIII (FVIII) deficiency is an X-linked recessive disorder occurring in 1 in every 5000 male births without an ethnic predominance [Soucie et al. 1998]. Currently the mainstay of treatment is the replacement of FVIII with the use of either plasma or recombinant FVIII concentrates to achieve hemostasis. FVIII replacement is effective unless a patient develops an alloantibody (inhibitor) against the exogenous FVIII. FVIII inhibitors interfere with the infused factor concentrates rendering them ineffective and necessitating the use of more costly and less effective alternative hemostatic agents [Di Minno et al. 2010; Gringeri et al. 2003]. Inhibitor development is currently the most significant treatment complication seen in patients with hemophilia. While improvements in hemostatic agents for patients with inhibitors have resulted in decreased mortality, inhibitors are still associated with significant morbidity, including a higher rate of bleeding complications, increased disability and a decreased quality of life[Brown et al. 2009; Darby et al. 2004; Di Minno et al. 2010; Gringeri et al. 2003; Morfini et al. 2007].
Definition of an inhibitor
An inhibitor is a polyclonal high-affinity immunoglobulin G (IgG) that is directed against the FVIII protein [Fulcher et al. 1987; Gilles et al. 1993]. IgG4 antibodies are predominant and do not fix complement [Fulcher et al. 1987; Gilles et al. 1993; Lollar, 2004]. The formation of a FVIII inhibitor is a T-cell dependent event that includes antigen-presenting cells, B- and T-helper lymphocytes [Astermark, 2006]. Antibodies can be either inhibitory or noninhibitory. FVIII contains three A domains (A1, A2, A3), one B domain and two C domains (C1, C2). Inhibitory antibodies are primarily directed against the A2, A3 and C2 domains [Fulcher et al. 1985; Scandella et al. 1989]. Antibody binding at these domains results in steric hindrance blocking functional epitopes of FVIII [Saint-Remy et al. 2004]. These functional epitopes include FIX, phospholipid and von Willebrand factor interaction sites. Antibodies in inhibitor patients can simultaneously target multiple FVIII epitopes and these epitope targets can change over time [Fulcher et al. 1988].
FVIII inhibitors are classified based on the kinetics and extent of inhibition of FVIII. Type I inhibitors follow second-order kinetics (dose-dependent linear inhibition) and completely inactivate FVIII. Type II inhibitors have complex kinetics and incompletely inactivate FVIII. Type I inhibitors are more common in severe hemophilia. Type II inhibitors are more common in inhibitor patients with mild hemophilia or in patients without hemophilia who develop an acquired FVIII inhibitor.
Laboratory characterization of an inhibitor
The most common methods used to detect and quantify FVIII inhibitors include the Bethesda assay or the Nijmegen-modified Bethesda assay [Kasper et al. 1975; Verbruggen et al. 1995]. The International Society on Thrombosis and Hemostasis FVIII/FIX subcommittee recommend that the Nijmegen-modified Bethesda assay be used secondary to improved sensitivity and specificity [Giles et al. 1998]. These assays only detect inhibitors that reduce FVIII activity (inhibitory). Both assays utilize serial dilutions of a patient’s plasma that is incubated with equal volumes of normal plasma for 2 h at 37°C [Lee et al. 2005]. The residual factor VIII level of the incubation mixtures is measured. A positive result is when there is a significant decrease in the residual FVIII. The dilutions and residual factor VIII are plotted against each other and the inhibitor titer is obtained by linear regression [Lee et al. 2005]. By definition one Nijmegen-Bethesda unit reduces the FVIII activity level by 50%.
There are limitations to laboratory measures of inhibitors, including a limited sensitivity for low titer inhibitors [<0.4 Nijmegen-Bethesda unit (BU)/ml]. There is also a high inter-laboratory variation in the quantitation of inhibitors with a high number of false-positive and false-negative results [Meijer and Verbruggen, 2009]. This is likely secondary to a variation in how laboratories carry out their assays (use a mix of the Bethesda and Nijmegen methods) and a lack of a reference antibody standard [Meijer and Verbruggen, 2009]. These assays are also better at detecting and measuring type I inhibitors than type II inhibitors. Enzyme-linked immunosorbent or fluorescent based immune assays can detect both inhibitory and noninhibitory antibodies and may have improved detection for low-titer inhibitors but further validation is needed to support widespread use [Dazzi et al. 1996; Ling et al. 2003; Zakarija et al. 2011].
Inhibitors are classified into low- or high-responding inhibitors based on a patient’s peak inhibitor titer after repeated FVIII exposure. The International Society on Thrombosis and Hemostasis Scientific and Standardization committee has recommended that an inhibitor titer of 5 BU differentiates low- from high-responding inhibitors [White et al. 2001]. An antibody titer that is persistently below 5 BU despite repeat challenges with factor VIII is considered a low-responding inhibitor. A high-responsive inhibitor is applied if the assay has been greater than 5 BU at any time [White et al. 2001].
Epidemiology
A systematic review regarding the epidemiology of inhibitors in hemophilia A reported an overall inhibitor prevalence of 5–7% and when limited to patients with severe disease the prevalence is much higher at 12–13% [Wight and Paisley, 2003]. The incidence of new FVIII inhibitors in patients with severe FVIII deficiency is approximately 30% [Lusher et al. 1993]. About 60% of these inhibitors are high titer (>5 BU) and the remaining are low titer (<5 BU) [Lusher et al. 1993]. Inhibitors are less common in patients with mild or moderate hemophilia occurring in approximately 3–13% of patients [Addiego et al. 1993; Ehrenforth et al. 1992; Sultan, 1992]. Most patients develop an inhibitor within a relatively short time period of exposure with a median of 9–12 exposure days [Addiego et al. 1993; Bray et al. 1994; Ehrenforth et al. 1992; Lusher et al. 1993]. A recent study from the UK revealed a previously unrecognized bimodal peak of inhibitor risk in early childhood and old age [Hay et al. 2011]. Further studies are needed to investigate this late peak of inhibitor formation and the mechanism that underlie this.
Clinical presentation
Factor VIII inhibitors can be detected either with routine laboratory testing or by clinical presentation. An inhibitor is clinically suspected when a patient experiences bleeding that does not adequately respond to hemostatic therapy. It is also prudent to check an inhibitor titer prior to an invasive procedure to ensure adequate hemostasis. Currently there is no consensus regarding the routine surveillance for inhibitors. Many providers check inhibitor titers at regular intervals within the highest risk period of the first 50 exposure days and then annually [Kempton and White, 2009]. There can be drawbacks to routine surveillance, including the detection of transient inhibitors which can result in significant patient anxiety.
Genetic risk factors for inhibitor formation
Genetic mutation
A patient’s specific FVIII genetic mutation is the most significant risk factor for inhibitor formation. While the overall incidence of inhibitor formation in patients with severe hemophilia A is approximately 30%, this proportion varies significantly among the type of factor VIII mutations. Those mutations that are null (large deletions, nonsense mutations and intron 22 inversions) and do not produce a FVIII protein are associated with the overall highest rates of inhibitor formation (21–88%) [Oldenburg et al. 2004]. The intron 22 inversion, the most common severe FVIII mutation, has an inhibitor incidence of 21% [Oldenburg et al. 2004]. Large deletions that involve multiple domains have the highest proportion of inhibitor formation of 88% [Oldenburg et al. 2004]. Mutations that result in a loss of FVIII function but retain some FVIII production (missense and splice mutations) have a lower risk of inhibitor formation (3–10%) [Oldenburg et al. 2004]. Of special interest are small deletions or insertions within stretches of adenine repeats (poly-A run) that result in a very low risk of inhibitor formation (3%) [Oldenburg et al. 2004]. It was discovered that there is endogenous restoration of the reading frame that results in a small amount of FVIII production that is likely sufficient to induce tolerance [Young et al. 1997].
A recent meta-analysis of FVIII genetic mutation and inhibitor development included data from 30 different studies with a total of 5383 patients with severe hemophilia A [Gouw et al. 2012]. To date, this is the largest study on FVIII genetic mutation and inhibitor formation providing more precise estimates of inhibitor risk. Compared with the risk of inhibitor formation in inversion 22, large deletions and nonsense mutations had an increased inhibitor risk with an associated odds ratio (OR) of 3.6 [95% confidence interval (CI) 2.3–5.7]. The risk of inhibitor formation from intron 1 inversion (OR 0.9; 95% CI 0.6–1.5) and splice site mutations (OR 1; 95% CI 0.6–1.5) was equal to intron 22 inversion. For small deletions/insertions and missense mutations the risk was lower (OR 0.5; 95% CI 0.4–0.6).
Race/ethnicity
Patients of African or Hispanic heritage have an increased risk of inhibitor formation [Aledort and Dimichele, 1998; Astermark et al. 2001; Carpenter et al. 2012; Ragni et al. 2009a; Scharrer et al. 1999]. Early studies demonstrating these associations were criticized secondary to a lack of control for FVIII genotype. A recent study by Miller and colleagues when controlling for genotype still demonstrated an increased risk of inhibitor formation in patients of African or Hispanic descent [Miller et al. 2012]. The mechanisms that account for these racial/ethnic differences remain unclear. Viel and colleagues found that a difference in FVIII haplotype between patients of African heritage and recombinant FVIII products accounted for this difference [Viel et al. 2009]. Critics of the study by Viel and colleagues report concerns regarding adequate control of confounding and how the mutational analysis was completed [Eckhardt et al. 2009a; Lacroix-Desmazes et al. 2009; Peyvandi et al. 2009; Santos et al. 2009; Yang et al. 2009]. Further studies are required to confirm this finding.
Immunologic factors
Individual immune response traits may also affect a patient’s reaction to exogenous factor VIII. Explored immunologic factors include the major histocompatibility complex (MHC) class II system and polymorphisms of cytokines [interleukins (ILs), tumor necrosis factor (TNF)-α]. To date MHC phenotype has not consistently been demonstrated as a risk factor for inhibitor formation [Astermark et al. 2006a; Hay et al. 1997; Oldenburg et al. 1997; Pavlova et al. 2009]. The Malmo International Brother Study demonstrated that polymorphisms of the TNF-α gene and IL-10 are associated with an increased risk of inhibitor formation [Astermark et al. 2006a, 2006b]. Additional studies regarding IL-10 polymorphisms have revealed inconsistent results [Bafunno et al. 2010; Lozier et al. 2011; Pavlova et al. 2009]. Variation in study results is likely secondary to study design and the specific hemophilia population that is being studied. Further studies are needed to confirm these findings.
Treatment-related risk factors for inhibitor formation
Inhibitor formation is a complex immune response that depends not only on the genetic factors discussed previously but also on treatment-related risk factors. Treatment-related risk factors that have been postulated include age at first exposure, the intensity of the first exposure, ‘danger signals’, prophylaxis, and the type of FVIII product (recombinant versus plasma derived). Interpretation of the current studies regarding environmental risk factors is complicated secondary to retrospective designs, variable methodologies and lack of control for confounding factors.
There are conflicting data regarding age at first treatment as a risk factor for inhibitor formation. Two small cohort studies found an inverse correlation between the age (<6 months) of first exposure and inhibitor formation but they were not controlled for risk factors for inhibitor formation [Lorenzo et al. 2001; van der Bom et al. 2003]. Additional studies that controlled for known confounders (i.e. FVIII genetic mutation, treatment intensity) were unable to demonstrate an association with age [Chalmers et al. 2007; Gouw et al. 2007b; Maclean et al. 2011; Santagostino et al. 2005]. It is likely that the association between inhibitor development and age of first factor exposure is explained by early intensive therapy [Kempton and White, 2009].
The intensity of the first FVIII exposure is postulated to be a risk factor for inhibitor formation because significant cell injury or inflammation leads to immunologic ‘danger signals’ that stimulate antigen-presenting cells and amplify an immunologic response which could promote inhibitor development [Gallucci and Matzinger, 2001; Kono and Rock, 2008; Matzinger, 2002]. Several studies have demonstrated an increased rate of inhibitor formation after intensive treatment (i.e. surgical procedure or high-frequency treatment) [Gouw et al. 2007a, 2007b; Maclean et al. 2011; Ragni et al. 2009a]. However, a case–control study by Santagostino and colleagues did not confirm these findings [Santagostino et al. 2005]. Overall it does appear that there is an increased risk of inhibitor formation after an intense initial FVIII exposure. This association is not a reason to withhold life-saving therapy but should prompt a clinician at the time of a significant early exposure to monitor closely for the development of an inhibitor.
There is an ongoing debate regarding the immunogenicity of factor products with a concern that recombinant products have an increased risk of inhibitor formation over that of plasma-derived products. This increased immunogenicity is hypothesized to be secondary to alterations in posttranslational modifications of FVIII and a lack of von Willebrand binding [Dasgupta et al. 2007; Grancha et al. 2011; Hironaka et al. 1992; Qadura et al. 2009]. There are conflicting reports in the literature that have led to this state of uncertainty. In comparing studies in previously untreated patients (PUPs) there is a difference in the overall reported cumulative incidence of inhibitor formation in plasma derived (10.3%) versus recombinant (28.7%) [Mannucci et al. 2012]. The difficulty in comparing the cumulative incidence from these studies is the high degree of heterogeneity in patient inhibitor risk factors, study methodology, frequency of inhibitor testing and length of follow up [Mannucci et al. 2012]. Two recent systematic reviews attempted to control for this known heterogeneity, and were unable to demonstrate a difference in inhibitor formation [Franchini et al. 2012; Iorio et al. 2010]. In the review by Iorio and colleagues, study design, study period, testing frequency and median follow up explained most of the variability and the source of factor concentrate lost statistical significance [Iorio et al. 2010]. To address this very important clinical question a prospective international randomized clinical trial (SIPPET – Survey of Inhibitors in Plasma Product Exposed Toddlers) is currently enrolling patients and is comparing inhibitor incidence in previously untreated patients exposed to either plasma or recombinant factor products [Mannucci et al. 2007].
The use of early prophylaxis at a young age has been proposed as a mechanism to induce tolerance through early controlled antigen exposure and to minimize the possibility that the first FVIII exposure is in the setting of a ‘danger signal’. Two cohort studies, an Italian cohort and the CANAL (concerted action on neutralizing antibodies in severe hemophilia A) study, reported a decreased risk of inhibitor formation for patients receiving prophylaxis versus on-demand therapy [Gouw et al. 2007b; Santagostino et al. 2005]. This was not confirmed in a cohort study from the UK [Maclean et al. 2011]. A small prospective pilot study in 26 PUPs from Germany were treated with 25 IU/kg/week as soon as bleeding tendency manifested [Kurnik et al. 2010]. The prevalence of inhibitor formation was compared with historical controls with a significant decrease in inhibitor formation in the study group with only 1/26 (3%) developing inhibitors versus 14/30 (46%) with an associated OR of 0.048 (95% CI 0.001–0.372) [Kurnik et al. 2010].This study, however, has been criticized for not having contemporaneous controls, and the quite spectacular results need to be confirmed in prospective studies.
Table 1 provides a summary of all the known current risk factors for inhibitor formation.
Risk factors for inhibitor formation in hemophilia A.

Stratification of inhibitor risk
With the advancement in the understanding of risk factors that underlie inhibitor formation, efforts have been made to create a clinical scoring system to quantify an individual’s risk. Ter Avest and colleagues created a clinical scoring system that utilizes three clinical factors (family history of inhibitor, gene mutation and intensive treatment at initial exposure) to predict inhibitor formation [ter Avest et al. 2008]. The risk score is cumulative and includes two points for a positive family history of inhibitors, two points for a high-risk gene mutation and three points if the initial FVIII treatment is intensive. Patients without any risk factors (risk score=0 points) had an inhibitor incidence of 6%, 23% in those with two points and 57% in those patients with more than three points [ter Avest et al. 2008]. The limitations of this clinical scoring system include the use of a primarily white cohort and the lack of inclusion of other well established risk factors.
While a risk score can help identify patients at the highest risk for inhibitor formation we are still left with a quandary as to how to effectively minimize this risk. As mentioned previously, some propose the institution of early prophylaxis, although further data are needed to confirm these findings. Others have proposed the use of alternative hemostatic products to delay FVIII exposure. Rivard and colleagues completed a prospective trial in 11 pediatric patients with severe hemophilia using recombinant factor VIIa to try and postpone exposure to FVIII until after 2 years of age [Rivard et al. 2005]. Owing to inadequate hemostasis with recombinant factor VIIa, especially in mouth bleeding, only 3 out of 11 children could postpone FVIII exposure until after 2 years of age [Rivard et al. 2005], making this therapeutic option limited. Challenges remain as to the most effective manner in which to minimize a patient’s risk of inhibitor formation and further studies are required.
Eradication of inhibitors
Owing to the significant clinical ramifications of inadequate hemostasis in patients with high-titer FVIII inhibitors, the overarching therapeutic goal is eradication of the inhibitor. At this time the only proven method for eradication is immune tolerance induction (ITI). ITI is the regular infusion of FVIII to induce FVIII antigen-specific tolerance. There is currently no consensus regarding the specifics of ITI treatment, including the factor product source (plasma derived versus recombinant), factor dose, timing or the use of immune modulation.
Multiple immune tolerance registries were established to help determine patient- and treatment-related factors associated with immune tolerance outcome [Coppola et al. 2009; Dimichele, 2009; Haya et al. 2001; Lenk, 2000; Mariani et al. 1994]. Overall reported success rates in these registries ranged from 51% to 79% [Coppola et al. 2009; Dimichele, 2009; Haya et al. 2001; Lenk, 2000; Mariani et al. 1994]. This wide range in success rates is likely secondary to a lack of standardization in study methodologies, treatment protocols, and eradication definitions. Consistently across these registries a patient’s peak historical FVIII inhibitor titer (<200 BU) and the inhibitor titer at the time of ITI induction (<10 BU) were associated with successful immune tolerance. Other predictors have been identified but have not been consistent across studies. Table 2 provides a complete list of predictors for ITI.
Predictors of immune tolerance induction
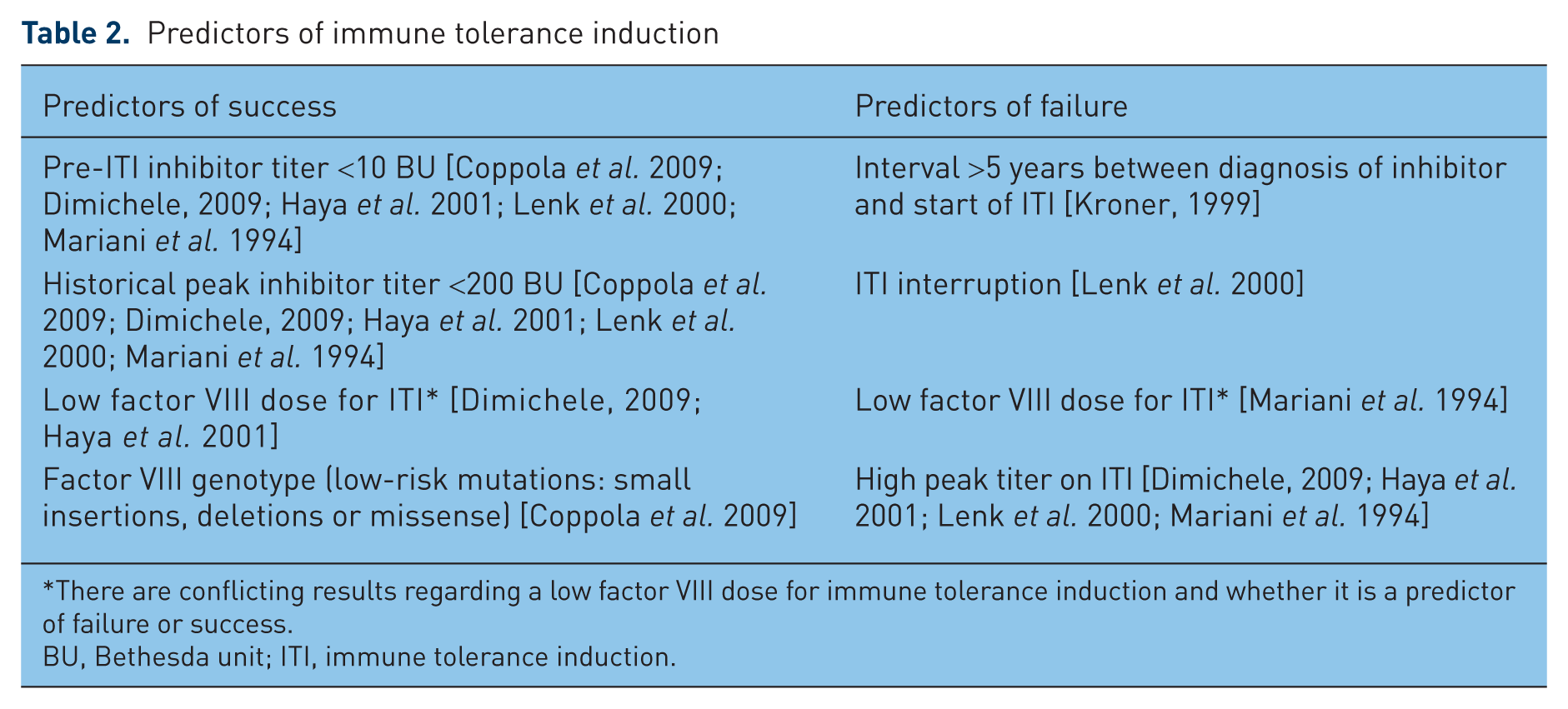
There are conflicting results regarding a low factor VIII dose for immune tolerance induction and whether it is a predictor of failure or success.
BU, Bethesda unit; ITI, immune tolerance induction.
There are conflicting data regarding the ITI factor VIII dose and success of ITI. The International Immune Tolerance Registry demonstrated improved ITI success with high doses (200 IU/kg) while the North American and Spanish Immune Tolerance Registries demonstrated improved success with lower dosing strategies [Dimichele, 2009; Haya et al. 2001; Mariani et al. 1994]. A meta-analysis of the International and North American Registries found that FVIII dosing did not influence ITI success [Kroner, 1999]. To address this discrepancy the International Immune Tolerance Study was completed [Hay and DiMichele, 2012]. This multicenter randomized clinical trial compared high-dose (200 IU/kg/day) with low-dose (50 IU/kg three times/week) regimens in patients with severe hemophilia A and high-titer inhibitors (>5 BU). Product choice was left up to the managing clinician; 90% received recombinant FVIII products. This study was stopped early secondary to increased bleeding events in the low-dose arm. There was no difference in the proportion of ITI success between the two arms but the time to achieve ITI success was shorter in the high-dose arm. Because the study was stopped early it lacked statistical power to demonstrate therapeutic equivalence below the 30% boundary of equivalence. It appears that a high-dose strategy achieves tolerance at a faster rate and this may explain the associated decreased bleeding rate.
Controversy also remains regarding the source of product for immune tolerance and the impact on ITI success. The role of von Willebrand factor in achieving tolerance is unclear. The current published data are limited by small sample size, retrospective design and lack of control for known confounders. A recent comprehensive literature review in comparing these studies found no difference in ITI success based on factor product, with success rates of 75–87% in plasma-derived FVIII, 68–91% in von Willebrand factor containing products and 63–82% in recombinant products [Franchini and Lippi, 2011]. The RESIST (Rescue Immunotolerance Study naive) trial is currently enrolling patients and is a randomized clinical trial that compares ITI success in high-risk patients (age >6 years, peak historical inhibitor >200, pre-ITI titer >10 BU, time between inhibitor formation and ITI >2 years) using von Willebrand factor containing FVIII versus recombinant FVIII [Gringeri, 2007]. At this time the available evidence does not support the superiority of one product source over another for use in ITI.
Although not common to most ITI protocols the use of immune modulation has been reported as a method to improve tolerance success. In Sweden the Malmo protocol uses a combination of immunoabsorption (to acutely decreased the FVIII inhibitor titer), cyclophosphamide, intravenous immunoglobulin and daily high-dose FVIII [Nilsson et al. 1988]. The reported benefit appears to be decreased time to tolerance but the overall success rate is comparable to ITI protocols without the risks associated with immune modulation [Berntorp et al. 2000]. Recently there has been an interest in the use of the monoclonal anti-CD20 antigen (rituximab) that inhibits B cells and interferes with IgG production. A phase II single-arm clinical trial used rituximab as a single agent in patients with high-titer inhibitors whose condition had failed to respond to prior ITI attempts. The results of this trial were presented as an oral presentation at the 2011 American Society of Hematology Annual Meeting [Leissinger et al. 2011b]. The authors reported that only 3 out of 16 subjects enrolled (18.8%) had a major response (fall in the inhibitor to <5 BU without an increase in the inhibitor titer after rechallenge to FVIII) [Leissinger et al. 2011b]. It appears that as a solo agent in patients previously treated with inhibitors, rituximab had a small effect but further studies are needed to determine if rituximab could be more effective if used with ITI.
New strategies for immunomodulation in FVIII inhibitors
Currently there is ongoing research in mouse models focusing on novel products and methods to modulate the immune response to factor VIII [Miao, 2010; Waters and Lillicrap, 2009]. Multiple methods have been used to manipulate antigen presentation, including oral or nasal administration of FVIII peptides, infusion of immature dendritic cells or apoptotic fibroblast cells [Qadura et al. 2008; Ragni et al. 2009b; Rawle et al. 2006; Su et al. 2010]. While these methods demonstrated a decrease in the immune response to FVIII they were unable to completely mitigate this response. Diverse strategies have also been explored that evade the immune response to FVIII. These include the preparation of less immunogenic FVIII proteins or through the ongoing exposure to FVIII through novel gene therapy methods including neonatal gene transfer, ex vivo transduction of hematopoietic stem cells or site-specific FVIII gene expression in platelets [Miao, 2010]. Additional focus has also been placed on targeted immunosuppression of either the T- or B-cell pathways. The most successful of these immunosuppressive efforts include those that increase T-regulatory cells using either protein replacement or gene therapy [Miao, 2010]. While much of this research is currently in mouse models, it is anticipated that many of these protocols warrant further consideration for clinical translational research. At this time it is unclear whether any of these strategies could be used alone, in combination or in concert with current ITI management. The ultimate goal for immunomodulation therapy is a therapy that allows a patient’s immune system to function appropriately while mediating long-term FVIII tolerance.
Hemostatic agents for patients with an inhibitor
Treatment of bleeding in a patient with an inhibitor is based on the classification of the inhibitor. A low-titer and low-responding inhibitor (<5 BU) can commonly be overcome with higher doses of FVIII, while patients with high-titer/high-responding inhibitors must be treated with bypassing agents. In general, bypassing agents can achieve hemostasis but they are not as effective as FVIII replacement in patients without an inhibitor. Options for bypass therapy include an activated prothrombin complex concentrate (aPCC; FEIBA, FVIII inhibitor bypassing activity; Baxter AG, Vienna, Austria) or recombinant factor VIIa (rFVIIa; NovoSeven, Novo Nordisk A/S, Bagsvaerd, Denmark). Porcine factor VIII is not currently available although a recombinant version is in development [Kempton et al. 2012]. Both rFVIIa and aPCCs have been demonstrated to be effective in the treatment of bleeding for patients with inhibitors [Buchanan and Kevy, 1978; Hilgartner and Knatterud, 1983; Kurczynski and Penner, 1974; Lusher et al. 1998; Shapiro et al. 1998; Sjamsoedin et al. 1981]. A randomized crossover trial of rFVIIa versus FEIBA assessed patient reported efficacy 6 h after treatment and did not demonstrate statistical equivalence between the two products. [Astermark et al. 2007]. However, the confidence interval of the difference only slightly exceeded the 15% boundary (–11.4% to 15.7%), p = 0.59[Astermark et al. 2007]. The efficacy between products was rated quite differently by a substantial portion of subjects [Astermark et al. 2007.
In determining which bypassing product to use in an individual patient it is important to consider multiple factors, including the need to avoid FVIII exposure to prevent anamnesis and a patient’s individual response to therapy. In a patient with a newly diagnosed inhibitor whom one is waiting for the FVIII inhibitor titer to fall before initiating ITI it is prudent to use rFVIIa because aPCCs contain a small amount of FVIII and have been shown to increase the inhibitor titer. It is well recognized that there can be significant patient variability in their individual hemostatic response to bypassing agents. In some patients bleeding can be unresponsive to monotherapy and may require alternating products [Gringeri et al. 2011a; Schneiderman et al. 2004]. Secondary to the risk of developing thrombosis or disseminated intravascular coagulation from alternating bypassing agents, this therapy should be used with caution and only in an inpatient setting [Ingerslev and Sorensen, 2011].
It is clear that prophylaxis in patients with severe hemophilia (without an inhibitor) is effective in preventing bleeding [Gringeri et al. 2011b; Manco-Johnson et al. 2007]. Recently two trials have demonstrated the efficacy of bypassing agents as secondary prophylaxis for patients with inhibitors [Konkle et al. 2007; Leissinger et al. 2011a]. The first trial compared the efficacy of daily rFVIIa prophylaxis (90 μg/kg versus 270 μg/kg) in 22 inhibitor patients and demonstrated decreased bleeding at both dose levels (45% versus 59%) [Konkle et al. 2007]. Subsequent analysis also demonstrated an improvement in quality of life [Hoots et al. 2008]. More recently, a randomized crossover clinical trial compared the use of an aPCC (85 units/kg on three nonconsecutive days a week) with on-demand therapy and demonstrated a 62% overall reduction in all bleeding episodes [Leissinger et al. 2011a]. It is unclear which inhibitor patients should be considered for prophylaxis and this should be determined on a case by case basis. It is recommended that prophylaxis be considered for patients whose condition has failed to respond to ITI and who have recurrent significant bleeding (i.e. a target joint or life-threatening hemorrhages) [Young et al. 2011]. The use of bypassing agents for prophylaxis while a patient is undergoing an initial course of ITI should be done with caution because a patient’s FVIII level could improve while receiving a bypassing agent which could be prothrombotic [Young et al. 2011]. This is the subject of an ongoing clinical trial.
Inhibitors in mild hemophilia A
As discussed previously inhibitor development in mild hemophilia is less common then severe hemophilia with an estimated incidence of 3–13% [Addiego et al. 1993; Ehrenforth et al. 1992; Sultan, 1992]. Patients with mild hemophilia form inhibitors against the exogenous infused factor VIII and commonly there is inhibitor cross reactivity against the patient’s endogenous FVIII decreasing a patient’s baseline FVIII level. This decrease changes the patient’s bleeding phenotype from mild to moderate or severe. Inhibitors can be detected through routine screening or with a change in a patient’s bleeding pattern. Some patients may have bleeding manifestations that are more commonly seen in patients with an acquired inhibitor, including extensive mucocutaneous or urogenital bleeding. Others may experience bleeding more common to hemophilia with joint and intramuscular hemorrhage. Both type I and II inhibitors have been reported in mild hemophilia but there appears to be a predominance of type II inhibitors [Franchini et al. 2010].
Risk factors for inhibitor formation in mild hemophilia include later age with first factor VIII exposure, intensity of the factor exposure, family history of inhibitors and type of genetic mutation [Eckhardt et al. 2009b; Hay et al. 1998; Kempton et al. 2010; Mauser-Bunschoten et al. 2012; Sharathkumar et al. 2003]. Multiple studies have reported an association between the Arg593Cys genetic mutation and an increased risk of inhibitor formation [Eckhardt et al. 2009b; Hay et al. 1998; Mauser-Bunschoten et al. 2012]. However, in a recent study from the USA the Arg593Cys genetic mutation was not associated with an increased risk of inhibitor formation [Kempton et al. 2010]. HLA genotype has also been explored as a risk factor for inhibitor formation in patients with mild hemophilia with the Arg593Cys genetic mutation and no association was found [Bril et al. 2004].
There is no established standard of care for the treatment of patients with mild hemophilia and an inhibitor. Spontaneous resolution has been reported in up to 60% of cases after a median of 9 months (range 0.5–46) [Hay et al. 1998]. However, 75% of patients with spontaneous resolution experienced anamnesis with repeat FVIII exposure [Hay et al. 1998]. Eradication has also been achieved with the use of immune tolerance by itself or combined with immune modulation (prednisone, cyclophosphamide or rituximab) [Franchini et al. 2008; Hay et al. 1998; Robbins et al. 2001; Vlot et al. 2002]. The primary treatment strategy for patients with mild hemophilia should be inhibitor prevention. A desmopressin (DDAVP) trial should be completed for all patients with mild hemophilia. DDAVP should be used preferentially over factor products in those who are responders. Mutation analysis and family history can also be used to identify patients at the highest risk.
Conclusion
In conclusion, the development of an inhibitor is the most significant treatment complication in hemophilia A and is the result of complex interaction between a patient’s immune system and genetic and environmental risk factors. Great strides have been made in understanding the important risk factors for inhibitor development, including delineation of risk by genetic mutation, ethnic/racial differences, immunologic factors, and intensity of early factor exposure, but further elucidation is needed. Questions remain regarding the product source and the risk of inhibitor formation and we await the results of the SIPPET trial to help provide further clarification [Mannucci et al. 2007]. Data regarding early prophylaxis and inhibitor prevention are intriguing but prospective studies are needed to confirm these findings. ITI is considered standard of care for inhibitor eradication and a recent randomized clinical trial demonstrated that a high-dose (200 U/kg daily) regimen achieved tolerance faster and with less bleeding when compared with a low-dose (50 U/kg three times/week) regimen [Hay and DiMichele, 2012]. Uncertainty continues about the ITI product source, timing, dosing regimen, and the use of immune modulation. There is also new evidence to support the use of prophylaxis with a bypassing agent in patients with inhibitors, although it is unclear which inhibitor patients are the best candidates for this therapy [Konkle et al. 2007; Leissinger et al. 2011a; Young et al. 2011]. While significant progress has been made in the care of patients with inhibitors there remain many unanswered questions. Ideally in the future we will be able to accurately predict a patient’s individual risk of inhibitor formation and accordingly modify their individual treatment plan to minimize or abolish their risk of inhibitor formation.
Footnotes
Funding
This review article received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Conflict of interest statement
GY has received honoraria as a speaker for Baxter and Novo Nordisk. CW has no conflicts of interest to declare.