
Abstract
Intraventricular schwannomas are extremely rare, typically benign tumors originating from Schwann cells, which are not normally found within the ventricular system. Their presence challenges conventional understanding of tumor origins and complicates diagnosis and management. We report the case of a 19-year-old female presenting with a drop attack and headache, with no significant medical history. MRI revealed a heterogeneously enhancing lesion in the right lateral ventricle. Differential diagnoses included malignant tumors; however, histopathological examination post-surgical resection confirmed an intraventricular schwannoma. Postoperative outcomes were favorable, with successful CSF diversion via a right occipital ventriculoperitoneal shunt for isolated right temporal hydrocephalus. This case is notable for its atypical presentation in a young patient, challenging the conventional understanding that intraventricular schwannomas primarily affect older individuals. In addition, the correct diagnosis and successful management of a rare intraventricular schwannoma underscores the importance of considering this rare diagnosis in patients with nonspecific neurological symptoms and intraventricular lesions. This case, alongside the literature review, enriches the body of evidence on intraventricular schwannomas, highlighting the critical role of surgical intervention and the need for a comprehensive diagnostic approach.
Keywords
Introduction
Intraventricular schwannomas are rare and intriguing central nervous system (CNS) tumors. 1 Typically benign, schwannomas arise from Schwann cells, which form the myelin sheath of peripheral nerves and are usually found in the peripheral nervous system. 2 Their occurrence in the brain’s ventricular system is unusual since Schwann cells are not normally present there. 3 This rare presentation challenges our understanding of tumor origins and complicates diagnosis and management. 4 These tumors are often discovered incidentally, as patients usually present with nonspecific neurological symptoms such as headaches, seizures, and signs of increased intracranial pressure due to the tumor’s mass effect.5,6 Radiologically, they may mimic other intraventricular tumors, like ependymomas or choroid plexus papillomas. 7 However, a definitive diagnosis often relies on histopathological examination, revealing classic schwannoma features and S-100 protein positivity. 8 Surgical management aims to diagnose, relieve symptoms, and achieve maximum safe resection.5,9 Postoperative outcomes are generally favorable, though the risk of recurrence necessitates long-term follow-up. 10 By presenting a new case of an intraventricular schwannoma in a 19-year-old female, which is a rare and atypical presentation, we aim to add to the body of evidence. This case is particularly significant due to the patient’s young age and the unique clinical and radiological features observed. Our report provides further insight into managing this unusual entity and highlights the importance of considering intraventricular schwannomas in differential diagnoses for young patients with nonspecific neurological symptoms.
Case presentation
A 19-year-old female presented with a drop attack, associated with a headache. There was no prior history of similar attacks, and the patient had no noteworthy prior medical conditions. There were no focal neurological deficits, and no particular findings on physical examination.
MRI of the brain revealed an intraventricular, heterogeneously enhancing lesion seen within the posterior body/atrium of the right lateral ventricle, 3.0 × 2.6 cm in the axial plane and extends for about 3.6 cm craniocaudally. It showed an intermediate signal to gray matter on T1-weighted images and a hypointense signal on T2-weighted images with avidly heterogenous post-contrast enhancement with a central non-enhancing necrotic area (Figure-1(A)). The lesion was extending into the parenchyma, specifically the right pericallosal and right periventricular white matter, causing moderate vasogenic edema in the right parietal and posterior frontal lobes. The top differential diagnoses at this stage were two malignant tumors given the appearance on imaging; choroid plexus carcinoma and glioblastoma. MRI of pre- and post-operative findings. A: T1 weighted axial MRI showing a heterogeneously enhancing mass, with a central non-enhancing necrotic area extending into the pericallosal and periventricular white matter ipsilaterally, surrounded by moderate vasogenic edema in the right parietal and posterior frontal lobes. Axial view locates it in the posterior body/atrium of the right lateral ventricle. B: T1 weighted axial MRI with no evidence of any enhancing lesions with less prominent moderate edema in the right parietal lobe compared to preoperative state. There is a right-sided VP shunt with its tip seen within the right posterior cingulate gyrus. Dural thickening and enhancement is seen along the right cerebral convexity.
A microscopic iMRI-guided right parieto-occipital craniotomy was performed, and the tumor was excised successfully; gross total resection was achieved without any acute complications. The tumor appeared grape-like, grayish, and vascular. The postoperative period involved no complications. Post-operative MRI showed no gross residual tumor with no evidence of new brain lesion. The patient then developed isolated right temporal hydrocephalus confirmed by imaging, and hence CSF diversion was inserted with a right occipital ventriculoperitoneal shunt. Brain MRI following the insertion of the shunt (Figure-1(B)) showed no evidence of any enhancing lesions with less prominent moderate edema in the right parietal lobe compared to the preoperative imaging.
Histological examination of the specimen showed typical features of schwannoma with Antoni A alternating with Antoni B areas (Figure-2(A)). Hyalinized vessels, and focal pleomorphism were seen. No evidence of necrosis or increased mitotic figures could be identified. The tumor cells were diffusely positive for S-100 (Figure-2(B)) and SOX-10 (Figure-2(C)) immunostains. Interestingly, GFAP immunostain was also positive (not shown). The tumor cells were negative for EMA, H3 K27me3, and Olig-2. Histopathological examination of the intraventricular tumor. A: There is proliferation of spindle-shaped cells arranged in nodules showing palisading of nuclei consistent with Antoni-A areas (Arrow), alternating with hypocellular areas consistent with Antoni-B. B: S-100 immunostain is positive in the tumor cells with nuclear and cytoplasmic staining. C: SOX-10 immunostain shows strong nuclear staining.
The patient was scheduled for follow-up 6 months after the shunt insertion and had an excellent uneventful recovery post intervention.
Written informed consent was obtained from the patient and is available upon editorial request.
Discussion
Schwannomas are tumors of the Schwann cells, which are responsible for producing myelin sheaths around peripheral nerves. 11 They usually behave as WHO grade 1 tumors, that is benign and slow-growing, and very rarely undergo malignant transformation. 2 They can originate from any myelinated central or peripheral nerve with Schwann cells. 12 The majority of cases are sporadic, with the remaining occurring in association with specific syndromes, most commonly neurofibromatosis type 2, schwannomatosis, and meningiomatosis with or without neurofibromatosis type 2. 13
They are considered the most common nerve sheath tumor, shaping around 89% of cases. 14 Around 60% of benign schwannomas are vestibular schwannomas, which are associated with the vestibular branch of the vestibulocochlear nerve. 15 Intracranial schwannomas are responsible for 5%–8% of intracranial tumors, however, intracerebral schwannomas account for <1% of intracranial schwannomas. 16 Moreover, intra-axial localization of these tumors, given their origin from Schwann cells, is unusual. 17 There are multiple theories attempting to explain their pathogenesis, without any clear consensus on a particular one. These include, but are not limited to the neoplastic transformation of Schwann cells derived from neural crest that remained in the ventricles after a failure of migration and differentiation during embryogenesis, 18 the transformation of multipotent mesenchymal cells to Schwann cells due to tissue injury, 19 autonomic fibers of choroid plexus undergoing neuroplastic transformation to Schwann cells, 20 and the transformation of mesoderm-derived mesenchymal leptomeningeal cells in the brain into Schwann cells. 4 These all are plausible, and any could explain the occurrence of the tumor in our case.
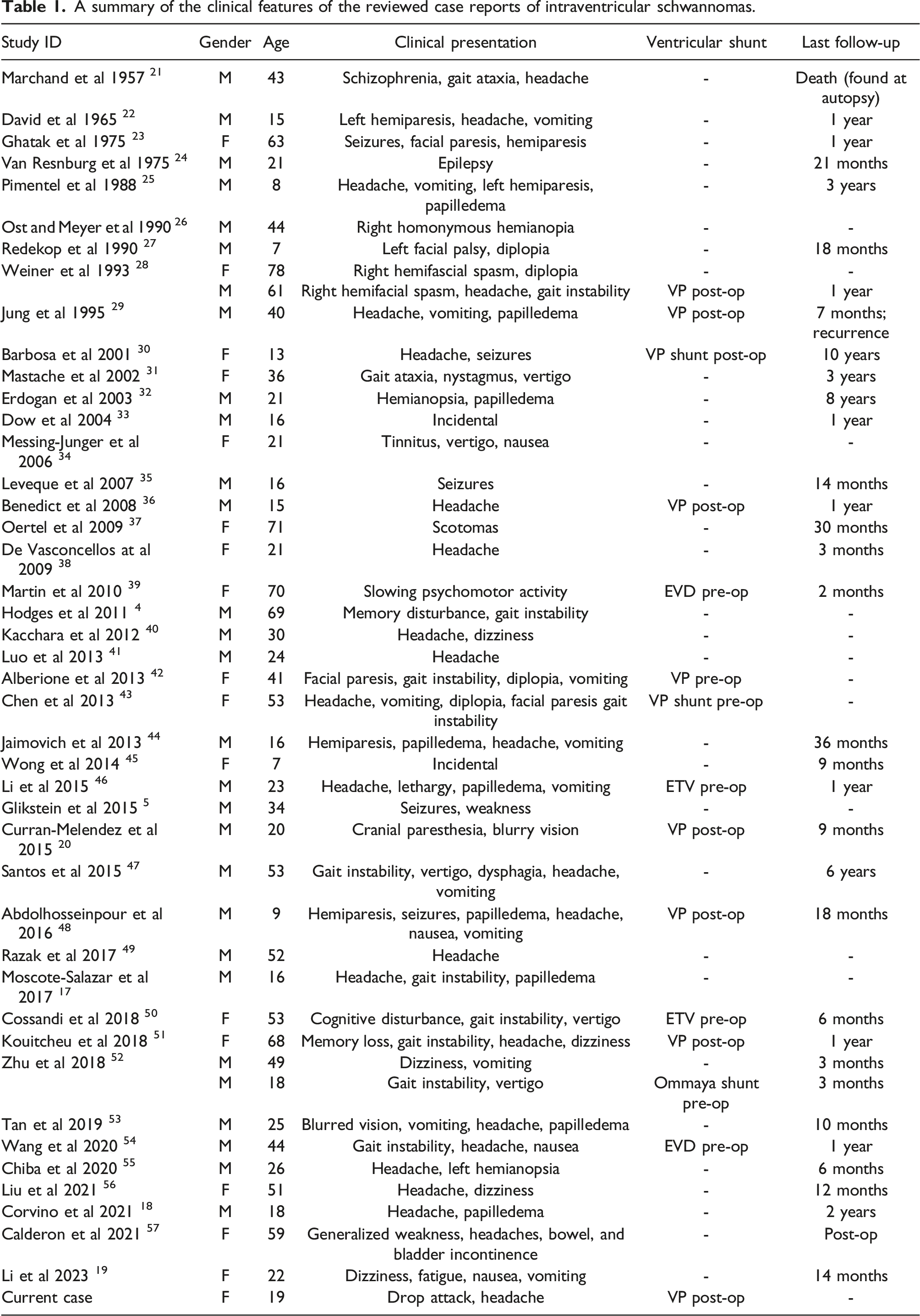
We underwent a comprehensive literature review of intraventricular schwannoma. We searched through many databases like PubMed, MEDLINE, Scopus, and Google Scholar; using keywords such as “Intraventricular Schwannoma”, “Ventricular System”,” Ventricular tumors”,” Schwann Cells”, “Neuro-oncology”, “Lateral ventricles”,” Third ventricle”, and” Fourth ventricle”. We included articles based on their relevance to intraventricular schwannomas, focusing mainly on clinical presentation, imaging characteristics, histopathological findings, and treatment outcomes. We also implemented no language or publication date restrictions when selecting articles, to ensure a broad coverage of the available literature. Data from selected articles were qualitatively analyzed to identify common patterns of this tumor’s clinical presentation, as well as radiological, histopathological features, and treatment outcomes.
A summary of the clinical features of the reviewed case reports of intraventricular schwannomas.

Findings from literature review. A: Age and gender distribution among patients reported with interventricular schwannomas. B: Annular reported cases of interventricular schwannomas. C: Locations and symptom frequencies in patients with intraventricular schwannomas.
The sizes of the tumors at the time of imaging varied, with some exceeding 25 mm in maximum diameter, suggesting variable growth rates and the potential for a significant mass effect.
Figure-3(B) illustrates the number of reported cases starting from 1957. Several factors have contributed to the marked increase in reported cases of intraventricular schwannomas in recent years. 58 Improved diagnostic imaging technologies, such as MRI, have significantly enhanced the identification of these rare tumors. 59 Additionally, a higher recorded incidence can be attributed to better reporting procedures and more comprehensive medical knowledge. 60 Increased global access to healthcare services has allowed more individuals to undergo evaluation for neurological symptoms, thereby increasing the likelihood of tumor diagnosis. 60 Therefore, publication bias towards more recent cases may also create a skewed perception of an increasing incidence.
The clinical presentation of intraventricular schwannomas varies widely. Being benign and slow-growing, schwannomas are expected to produce symptoms once they are large enough to exert a mass effect on surrounding structures or, given their location, cause obstructive hydrocephalus, 61 which was observed at presentation in nearly 24% of the reviewed cases.
Symptoms ranged from incidental findings to significant neurological manifestations, such as headaches, focal neurological deficits, gait ataxia, and seizures. 62 Also, some patients exhibited signs of increased intracranial pressure, such as papilledema. 63 Common locations and frequencies of encountered symptoms in the reviewed cases are depicted in Figure-3(C). Although typically benign, and this location is no exception, 64 the first ever reported case of an intraventricular schwannoma was malignant, 21 with a total of two cases of malignant intraventricular schwannomas reported in our review.
MRI is the preferred modality for diagnosing schwannomas, typically revealing post-contrast enhancement and heterogeneous signal intensity, especially in cases with cystic degeneration. 65 These tumors are usually accompanied by vasogenic edema The imaging findings reported in our review were consistent, with approximately 40% of cases displaying a cystic component, around 39% showing vasogenic edema, and some instances of calcification. The rarity of schwannomas in this location complicates diagnosis based solely on imaging, as numerous neoplastic entities commonly arise from the ventricles such as colloid cysts, glioblastomas, astrocytomas, craniopharyngiomas, ependymomas, meningiomas, among others.41,66 Often, the diagnosis would be presumed to be one of these entities until confirmed by histopathological analysis.
A summary of the histological findings and MRI findings of the available case reports of intraventricular schwannomas.

As in the current case, surgical resection is considered the treatment of choice, as these tumors can cause obstructive hydrocephalus and other complications due to their mass effect.51,70 In this specific case, the patient underwent a microscopic iMRI-guided right parieto-occipital craniotomy, resulting in the successful gross total resection of the tumor without acute complications.
Approximately 31% of the reviewed cases involved CSF diversion procedures, either preceding or following surgery, 64% of which were ventriculoperitoneal shunts; the remainder utilized EVD, ETV, and Ommaya shunts. In our case, a VP shunt was placed in the patient post-surgery.
The favorable outcome underscores the importance of a tailored surgical approach and vigilant postoperative care, even when initial symptoms do not directly correlate with the lesion’s presence.
Conclusion
We present a rare case of an intraventricular schwannoma in a 19-year-old female that was successfully treated through surgical intervention. This entity’s rarity and the paradoxical presence of Schwann cells within the ventricular system of the brain underscore the need for a high index of suspicion and a comprehensive diagnostic approach, integrating radiological and histopathological analyses to achieve an accurate diagnosis. The significance of reporting such cases lies in enriching the existing literature, thereby enhancing our understanding of their clinical presentation, diagnostic challenges, and management strategies. This case, alongside a review of the literature, contributes valuable insights into the management of intraventricular schwannomas. It highlights the importance of considering this rare diagnosis even in younger patients, the role of MRI and histopathological examination in accurate diagnosis, and the critical importance of surgical intervention in achieving symptom relief and tumor control.
Footnotes
Authors Contributions
R.M.H. Conceptualization and design of the study, acquisition of data, drafting the initial manuscript, and revising it critically for important intellectual content. Provided final approval of the version to be published. Z.J. Analysis and interpretation of data, revising the manuscript critically for important intellectual content, and provided supervision throughout the project. Ensured that questions related to the accuracy or integrity of any part of the work were appropriately resolved. S.A.S. Contributed to the literature review and analysis, assisted in drafting the manuscript, and contributed to the interpretation of data. Participated in revising the manuscript critically for important intellectual content. M.A.H. Provided pathological analysis and interpretation, contributed to the writing of the pathology sections of the manuscript, and critically reviewed the manuscript for important intellectual contributions. M.O. Involved in the case management and data collection, contributed to drafting and revising the manuscript, and provided insights into the clinical aspects of the case.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Data availability statement
The data that support the findings of this study are available on request from the corresponding author.