
Abstract
Keywords
Introduction
Gestational trophoblastic disease (GTD) is a group of benign and malignant lesions developed from placental tissue in the uterus. It occurs in approximately 1/1000 women of reproductive age. 1 This entity includes hydatidiform mole, invasive mole, placental site trophoblastic tumor, choriocarcinoma and epithelioid trophoblastic tumor. 2 Hydatidiform Mole (HM) represents 80% of GTD.1,2 There are two types of HM known as complete and partial. Complete HM results from the fertilization of an ovum without maternal chromosome by one sperm cell that duplicates its DNA afterwards (genotype 46XX) or by two sperm cells (genotype 46XY or 46 XX).2,3 Partial HM results from the fertilization of a healthy ovum by two sperm cells (genotype 69XXY/69XXX/69XYY).2,3
The diagnosis of complete or partial HM can be suggested by ultrasound findings in combination with clinical symptoms and high levels of human chorionic gonadotropin (HCG). 4
Ultrasound characteristic of complete mole is a heterogeneous intra-uterine mass with multiple round anechoic structures. In partial HM, it is possible to visualize an embryo.5,6
The final diagnosis is made on the removed trophoblastic tissue by histological examination and sometimes analysis of the karyotype. 7 Microscopic examination of complete HM shows trophoblastic hyperplasia, diffuse hydropic swelling 1 and no p57 immunostaining in the placental villi. 8 Partial HM shows different features: patchy villous hydrops and trophoblastic hyperplasia 3 with p57 immunostaining in the placental villi. 8
Suspicion of HM is classically handled by dilatation and curettage. 7 This surgical technique can have several complications such as: hemorrhage, perforation and post-operative retained product of conception (RPOC) which can sometimes lead to the realization of a second curettage. 7
HCG levels should be monitored after surgical treatment. A plateau or increase of HCG level should conduct to differential diagnosis between post-operative RPOC and gestational trophoblastic neoplasia (GTN) which occurs in 1–2% of partial HM and in 15–20% of complete HM and requires more clinical investigations and treatment. 3
The recent progress in hysteroscopic technology allowed to use this technique for the diagnosis of HM.9,10 Only one case of hysteroscopic resection (HsR) for partial HM has been described in the literature. 11 To our knowledge, there is no study regarding the feasibility of this technique for a larger number of patients.
Materials and methods
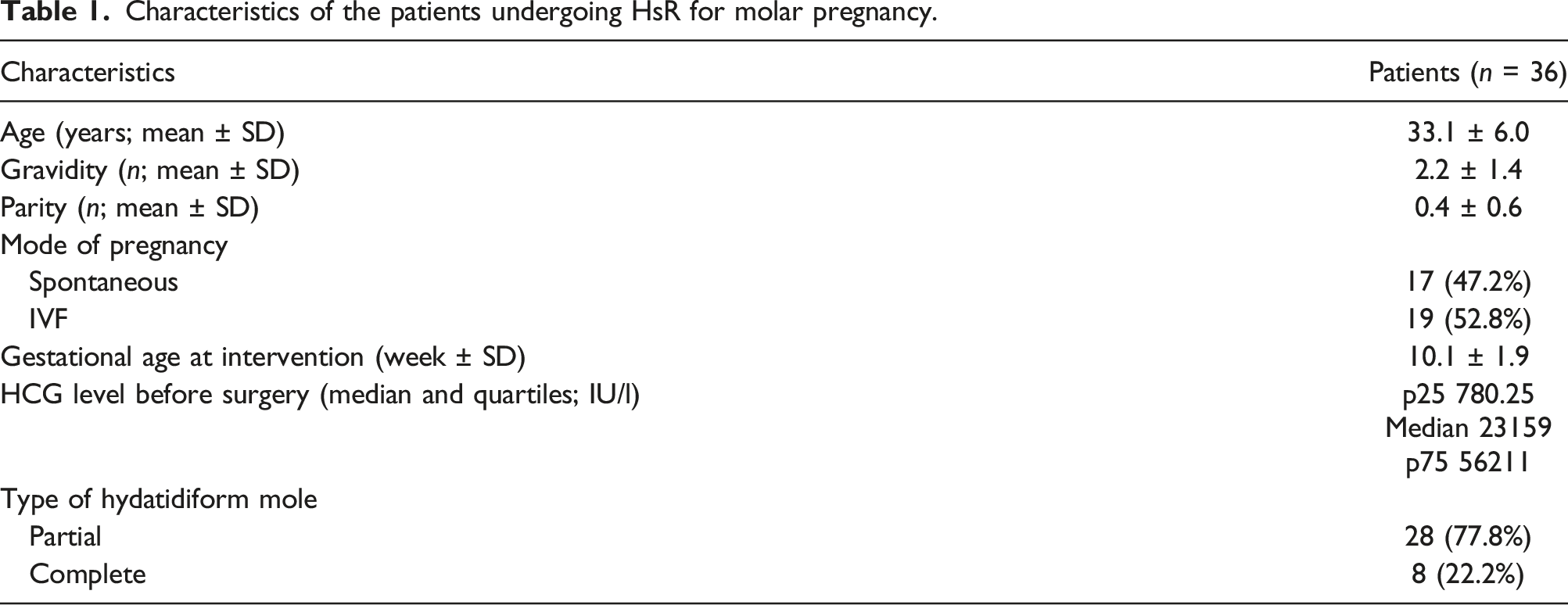
Suspicion of molar pregnancy as well as miscarriage is typically handled by HsR in the department of gynecology of our hospital. After approval of our ethics committee (reference number: 2021/06JAN/002), we proposed a retrospective review of the clinical experience at Cliniques Universitaires Saint-Luc Brussels from 2007 to 2019 and identified 36 women with HM treated by HsR. Data extraction was carried out using Medical Explorer® software. Medical records were analyzed to collect demographic data, surgical details, post-operative complications and follow-up. The primary outcomes were operative complications such as post-HsR glycine resorption (systematically used as we work with unipolar energy), perforation and hemorrhage. The secondary outcome was the presence of post-procedure RPOC.
Operative technique
The surgery is performed under general anesthesia. The cervix is dilated up to Hegar no. 10. Hystero-resectoscope is introduced in the cavity. With the loop, we take off the trophoblastic material. This surgical procedure requires gentle motions without application of electric energy. The procedure is performed with glycine flow. Hystero-resectoscope is then removed and a polyp forceps is inserted into the cavity to remove the freed material. The hysteroscope is reintroduced to check for uterine vacuity. We rarely used unipolar energy on small surface for hemostasis in case of persistent bleeding or for the resection of adherent trophoblastic tissue. Glycine is collected during the procedure in a plastic bag placed underneath the patient at the beginning of the surgery. After the procedure, we evaluate a potential glycine absorption (>1000 mL). In the situation of significant blood loss the anesthetist will inject 10 units of Syntocinon® intravenously. This surgical procedure remained unchanged during all the studied period.
Results
Characteristics of the patients undergoing HsR for molar pregnancy.
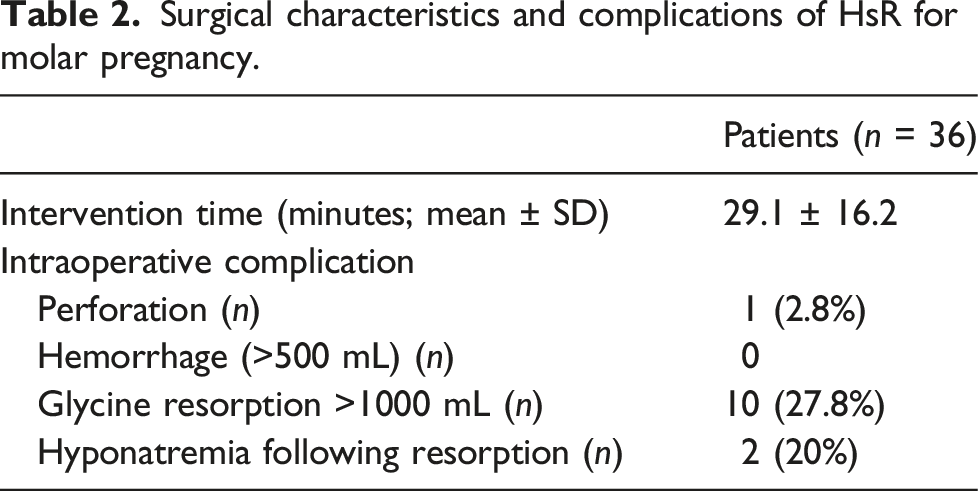
Surgical characteristics and complications of HsR for molar pregnancy.
Long term follow up after HsR for molar pregnancy.

Discussion
Suspicion of molar pregnancy is classically managed by D&C. With this paper, we offer a surgical alternative in the form of endoscopic management. Progress in surgical endoscopic technology has allowed to use hysteroscopic procedure for the management of “classic” miscarriage. 12 The advantage of this technique is to perform the resection of the trophoblastic product under visual control. Some small studies comparing HsR to D&C for indication of the surgical treatment of miscarriages showed fewer intrauterine adhesions, 13 better pregnancy rate 13 and quicker post-operative pregnancy.13–15
Gonzalez et al. (2018) 11 described the first hysteroscopic management of a partial HM in an 8 weeks pregnant patient. The procedure was uncomplicated and post-operative follow-up showed a good decrease of HCG levels. Office hysteroscopy was performed at 3 months showing a normal cavity. The authors emphasize that HsR, with direct visualization of the procedure could reduce the risk of RPOC in comparison with D&C.
Our department has a great experience in HsR for miscarriage 16 and suspicion of molar pregnancy is managed with the same procedure. The most frequent complication is glycine resorption which occurred in 27.8% of surgical procedures but did not lead to any major adverse event thanks to immediate diagnose and treatment. The standard rate of this complication described in the literature is 5% 17 but depend on the type of surgery. The trophoblastic tissue, being well vascularized, may be a reason for the high rate of fluid overload in our study. The development of bipolar hysteroscope (which was not available in our department at the time of the study) should reduce the consequences of this complication with the use of saline solution for uterine distention. We experienced one perforation of the uterus which represents 2.8% of the patients. This perforation was not predictable as it was the patient’s first pregnancy, she had no uterine pathology and had never been operated. The only particularity of this patient was the development of a post-operative GTN. To our knowledge, there are no data in the existing literature mentioning the standard rate of perforation in D&C. We found 16.7% of post-operative RPOC. Three studies in the existing literature describe the rate of RPOC after D&C for molar pregnancies: 33.3% in the series of Sato et al. (2019) 18 with 51 patients, 41% in the series of Yomamoto et al. (2019) 19 with 173 patients and 13.3% in the series of Padron et al. (2018) 20 with 1206 patients. In comparison with the literature, our rate of post-operative RPOC with HsR procedure seems to be in the range of those after D&C. RPOC can be managed by different methods: curettage, office hysteroscopy or operative hysteroscopy. We used the last two techniques for this indication in our series. The recent work of Raz et al. 21 shows that office hysteroscopy should be preferred in case of RPOC smaller than 2 cm as being safer (less perforation, hemorrhage, cervical tear) and quicker than operative hysteroscopy.
The retrospective design of our study is clearly limiting the strength of our observations but the description of HsR as a new procedure for the treatment of molar pregnancy with few adverse events could help to build more qualitative studies to compare it with D&C in randomized controlled trial.
Conclusion
The present study shows that hysteroscopic resection of molar pregnancy seems to be a safe new approach for the management of this pathology. Further studies are necessary to evaluate its potential benefits in comparison with D&C.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval to report this case series was obtained from Saint-Luc-UCLouvain’s Hospital-Faculty Ethics Committee (2021/06JAN/002).
Contributorship
MDC collected the data and wrote the manuscript. PJ, ML, JLS, MMD, CM, AG were part of the surgical team who treated the patients. JFB and EM were part of the oncological and pathology team respectively. Every authors participated actively in drafting sections of the manuscript, editing and approving the final submitted version. AG is the main supervisor of this work and she revised the final article.
Data availability
All data analyzed during this study are included in this article. Further enquiries can be directed to the corresponding author.