
Abstract
Well-differentiated thyroid carcinoma rarely spreads to soft tissues. Thyroid carcinoma arising within a mature cystic teratoma is even rarer. We report an extremely rare case of synchronous follicular thyroid carcinoma arising within a mature cystic ovarian teratoma and stage IV differentiated thyroid carcinoma. A 62-year-old woman who lived in an iodine-deficient area was accidentally diagnosed with an ovarian cyst during a radiological metastatic work-up for thyroid cancer. Following laparoscopic left salpingo-oophorectomy, histopathological examination revealed a follicular thyroid carcinoma arising within a mature cystic teratoma. After that, total thyroidectomy and surgical resection of the soft tissue lesion in the supraclavicular fossa were performed, and the patient received subsequent 131I ablation therapy, but the disease progression was recorded 3 months later. We believe that iodine deficiency plays a role in the malignant transformation of thyroid tissues within a mature cystic teratoma. In elderly individuals with significant metastases, radioactive iodine therapy is ineffective.
Introduction
Mature cystic teratoma (MCT) comprises approximately 20% of all ovarian neoplasms. It may occur at any age, with the highest incidence during the reproductive period. 1 Malignant transformation is an uncommon complication of mature cystic teratoma. It occurs in approximately 0.17–2% of cases and usually is observed in postmenopausal patients with squamous cell carcinoma accounting for more than 80%. 2 Any tissues in a mature cystic teratoma may undergo malignant transformation, including malignant melanoma, leiomyosarcoma, and thyroid carcinoma. 1
Thyroid carcinomas are the most common endocrine malignancies. They can be classified into two main categories: well-differentiated thyroid carcinoma (including papillary (PTC) and follicular thyroid carcinoma (FTC)) and poorly differentiated carcinoma (including medullary and anaplastic thyroid carcinoma). The most common thyroid cancer is PTC which accounts for over 80% of all thyroid cancers and is the predominant histology in patients exposed to radiation. The cervical lymph node metastasis rate in patients with PTC ranges from 30-80%. 3 However, distant metastases are seen at diagnosis in 2–5% of patients presenting with differentiated thyroid carcinoma. 4 Lung and bone are the most frequent sites of distant spread, and metastases are rarely identified in other soft tissues (10%). 5 The second most common thyroid cancer is FTC which accounts for 6–10% of all thyroid malignancies and is often found in iodine-deficient areas. 3
This report presents a case of synchronous follicular thyroid carcinoma arising from mature cystic teratoma of the ovary and stage IV differentiated thyroid cancer.
Case presentation
A female aged 62 years old was admitted to our institute with soft tissue metastasis of a follicular variant of papillary thyroid carcinoma, which was confirmed by biopsy (Figure 1). She reported that the tumor on her head had appeared for 3 months and gradually increased in size without any symptoms. Soft tissue metastasis of follicular variant of papillary thyroid carcinoma (HE, x400).
The patient was diagnosed with a thyroid nodule 30 years ago but did not receive any treatment. She has a history of hypertension which is currently being treated with Amlodipine. No record of radiation exposure and no family history of thyroid disease.
On examination, a firm left lobe thyroid nodule of about 2 cm which moves upon swallowing was found. The tumor on the head and the left supraclavicular fossa were around 1.5 cm and 2 cm in diameter, respectively.
Ultrasound of the thyroid revealed an 18 mm left lobe thyroid nodule, TIRADS 5 – ACR(2017). The 7 × 11 mm hypoechoic lesion in the left supraclavicular fossa. Cranial, thoracic, and abdominal computed tomography (CT) showed the 30 × 14 mm, extra-axial brain lesion without invading the right brain parenchyma; lung metastases; an 82 × 75 mm complex left ovarian mass, its content was mainly fluid with a small solid area (Figure 2(a) and (b)). Bone scan revealed bone metastases (frontal bone, mandible, right seventh anterior rib, left fourth posterior rib, L3 vertebra, and right distal tibia). The cancer antigen 125 level was 91.31 U/mL. Upper gastrointestinal endoscopy and colonoscopy were normal. Radiological findings and histopathological results of the patient. (a) Ovarian tumor. (b) Lung metastases. (c) Follicular thyroid carcinoma arising within a mature cystic teratoma (HE, x200). (d) Follicular variant of papillary thyroid carcinoma (HE, x400).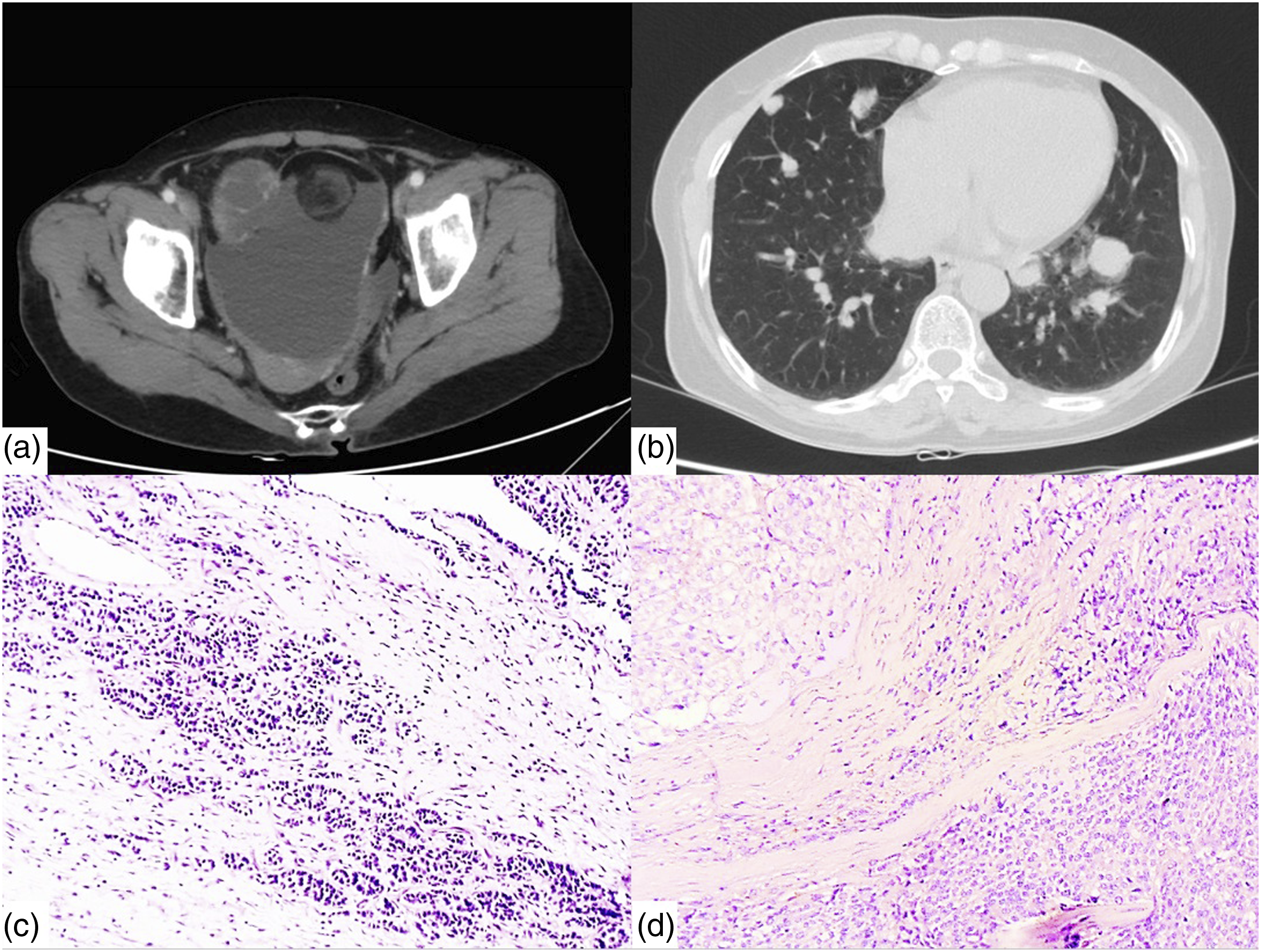
The fine needle aspiration (FNA)’s results of the left thyroid nodule and the left supraclavicular soft tissue were papillary thyroid carcinoma. A histopathology report of the biopsy of the tumor on the head was a follicular variant of papillary thyroid carcinoma. Therefore, the provisional diagnosis of this patient was the coexistence of a left ovarian cyst and stage IV thyroid cancer with metastasis to the lungs, bone, and soft tissues. The differential diagnosis was stage IV thyroid cancer with metastasis to the lungs, bone, soft tissues, and left ovary.
The patient underwent laparoscopic left salpingo-oophorectomy. Laparoscopy detected a large, rounded, smooth mass involving the left ovary, whereas other organs were free of macroscopic lesions. Specimen of the excised left ovary was sent for frozen sections which showed a granulosa cell tumor within MCT. The definitive histopathological examination revealed a follicular thyroid carcinoma arising from mature cystic teratoma (Figure 2(c)). Two weeks later, the patient underwent total thyroidectomy and surgical removal of left supraclavicular soft tissue; the histopathology of the left thyroid nodule and removed soft tissue are a follicular variant of papillary thyroid carcinomas (Figure 2(d)).
Following surgery, the patient was treated with Levothyroxine (LT4) and 131I (150 mCi per cycle). After the first dose, the whole body Radioactive Iodine (RAI) scan showed a skull, thyroid bed, mediastinal lymph nodes, two lungs, bilateral ilium, and bilateral femur uptake. A routine CT scan performed 3 months after the first 131I dose revealed disease progression (new lesions in the right hypochondrium, back, left thoracic wall, and left side of the forehead). Two weeks later, the patient’s health suddenly deteriorated, so she stopped taking LT4 and passed away 3 months later.
Discussion
Mature cystic teratoma comprises approximately 20% of all ovarian neoplasms. It is usually benign, but sometimes one of its contents may undergo malignant transformation. Mature cystic teratoma occurs most commonly during the reproductive years, but a malignant transformation of this tumor (about 2%) is usually observed in postmenopausal patients. 1 Although this complication is rarely diagnosed pre-operatively, due to its rarity, features such as larger tumor size (>10 cm), older patient age (>50 years), and elevated CA-125 level have been demonstrated to be predictive of malignancy. 1 In our case, we found an ovarian mass by chance while performing a CT scan, and the patient was old and had an elevated CA-125 level. These above factors can predict the malignant potential of the tumor. In addition, she also had stage IV thyroid cancer. 30 years ago, she found a thyroid nodule without any symptoms, so she received no treatment and had regular medical checkups. We all know that differentiated thyroid carcinoma is usually asymptomatic for a long period and commonly presents as a solitary thyroid nodule and benign thyroid nodules are also typically asymptomatic, giving no clinical clue to their diagnosis, 5 so the patient was incautious. By the time she presented with severe symptoms, her disease had already advanced.
Struma ovarii is an ovarian teratoma composed predominantly (over 50%) or entirely of thyroid tissue. 6 Although histologic characteristics of thyroid carcinoma are found in approximately 3% of struma ovarii type tumors and fewer than 200 cases have been reported in the medical literature,1,4 well-differentiated thyroid carcinoma arising from an MCT is even rarer. Pineyro et al. reviewed 20 cases of thyroid carcinoma arising within a mature cystic teratoma. The histopathologic types were papillary thyroid carcinoma (55%), a follicular variant of papillary thyroid carcinoma (40%) and only 1 case of follicular thyroid carcinoma (5%). 7 Since then, five additional cases have been reported, but none were FTC.8–12 Follicular thyroid carcinoma is more common in iodine-deficient areas. 3 Our patient lived in the Mekong Delta, Viet Nam. Coincidentally, in the aughts, this region had the lowest consumption of adequately iodized salt and median urinary iodine concentration of women in Viet Nam. 13 Besides, thyroid tissue as a teratoma component has histologic features like normal thyroid tissue and subjects to the same thyroid diseases as inflammation, hyperplasia, and tumors. 14 So, we believe iodine deficiency contributes to the malignant transformation of thyroid tissues within an MCT. To our knowledge, this is the second case of follicular thyroid carcinoma arising in MCT without evidence of struma ovarii and is the first case associated with the iodine-deficient area.
Patients in whom postoperative RAI is planned should undergo total thyroidectomy. 3 In our case, thyroidectomy serves two purposes: (1) it allows the proper clinical assessment (thyroid carcinoma with ovarian metastasis, or follicular thyroid carcinoma occurring in MCT); and (2) it potentiates iodine therapy. Although we can’t completely remove all distant metastatic lesions, thyroidectomy and surgical removal of the lesion in the supraclavicular fossa are performed. Moreover, the different histological type of carcinoma rules out the potential of ovarian metastasis. According to ATA (2015), the efficacy of RAI therapy is related to the mean radiation dose delivered to the thyroid cancer tissue and the radiosensitivity of tumor tissue. The radiosensitivity is higher in younger patients, with small metastases from well-differentiated papillary or follicular carcinoma. 15 Although, the histopathology of both thyroid and teratoma of this patient are well-differentiated thyroid carcinoma and there was uptake outside the thyroid bed on the first post-treatment whole body RAI scan, she was at an advanced age and had multiple metastatic lesions. These two factors lowered the radiosensitivity of tumor tissue and led to disease progression despite a significant concentration of RAI. We believe that this contributes to RAI refractory.
Conclusion
Follicular thyroid carcinoma arising within mature cystic teratoma is a rare condition with little information in the literature. People who reside in iodine-deficient areas have a higher risk of developing this complication. Radioactive iodine therapy in elderly patients with large metastases is not effective.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Can Tho Oncology Hospital does not require ethical approval for reporting individual cases or case series.