
Abstract
Pancreatic mature cystic teratomas are very rare with limited cases found in the literature. These lesions raise a diagnostic challenge and complicate the surgical approach not only because of their anatomic position but also because of their ever-growing size. An elusive diagnosis, usually leads to the operative theatre where surgical resection takes place. We present a rare case of a large pancreatic cystic teratoma extending into the mediastinum in a 29-year-old woman which was succesfully managed with en-bloc distal pancreatectomy and spleenectomy.
Introduction
Teratomas are congenital germ cell tumors, which originate from embryonic residues and include all 3 dermal layers, endoderm, mesoderm and ectoderm. 1 Mature cystic teratomas, or dermoid cysts, are benign, well-differentiated tumors commonly encountered in the ovaries and testes. 2
Pancreatic mature cystic teratomas are very rare with limited cases found in the literature. Kerr in 1918 was the first to describe a mature cystic teratoma of the pancreas. 3 These lesions raise a diagnostic challenge and complicate the surgical approach not only because of their anatomic position but also because of their ever-growing size.
We present a rare case of a large pancreatic cystic teratoma extending into the mediastinum in a 29-year-old woman.
Case report
A 29-year-old woman presented to the outpatient clinic complaining of abdominal discomfort, dysphagia, nausea and worsening epigastric pain for the past 5 months. She also reported new onset of dyspnea and vomiting during the past few days. Except for hypothyroidism under treatment, her past medical history was unremarkable. Her vital signs were normal while physical examination revealed a large palpable upper abdominal mass. Blood tests including white blood cells, serum amylase and lipase as well as tumor markers (CEA, CA19-9) were within normal limits. Upper GI endoscopy and esophageal manometry were normal. Abdominal CT scan revealed a hypodense mass measuring about 11 × 11 × 17 cm, arising from the body and tail of the pancreas. The mass was located between the left liver lobe, the spleen and the pancreas with evident displacement of the stomach and elevation of the diaphragm. There were no radiological signs indicative of pancreatitis or evidence of vascular invasion. Abdominal MRI revealed a huge cystic mass with well-defined margins measuring 12 × 10 × 18 cm with a solid fat component. The mass was projecting in the mediastinum, displacing the lower third of the esophagus anteriorly. There were no evident pathological lymph nodes or vascular invasion from the mass Figure 1. Dermoid cyst of the pancreas in CT and MRI scans (a). Sagital plane CT scan (b). Coronal plane CT scan (c). Transverse plane CT scan (d). Transverse plane MRI scan (e). Coronal plane MRI scan.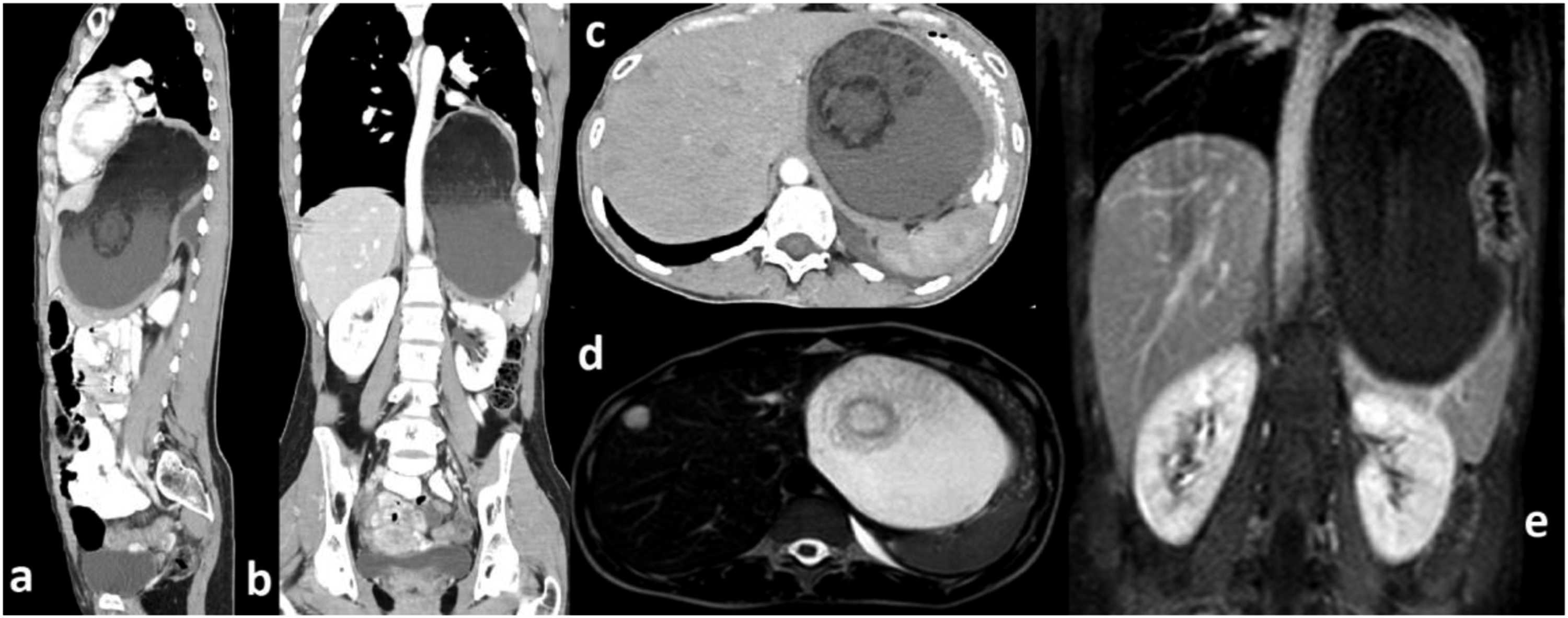
Due to the suspicion for mucinous cystadenoma along with the deteriorating long-lasting symptomatology and the increased tumor size, surgical exploration was decided at the MDT meeting. The patient underwent exploratory laparotomy through a midline incision. The cystic mass was found to originate from the body and tail of the pancreas, adherent to the posterior aspect of the stomach. The splenic vessels were encased within the mass and were ligated proximally. The mass was carefully mobilized from the retroperitoneum and the posterior stomach wall. As it was entering the mediastinum through the esophageal hiatus, it was dissected from the mediastinal pleura, which was left intact, and the diaphragmatic esophageal hiatus was suture-repaired. The resection was completed by en bloc distal pancreatectomy and splenectomy Figure 2. The patient had an uncomplicated postoperative course and was discharged on postoperative day 7. Surgical specimen. Dermoid cyst (ruptured) along with spleen and pancreatic body and tail.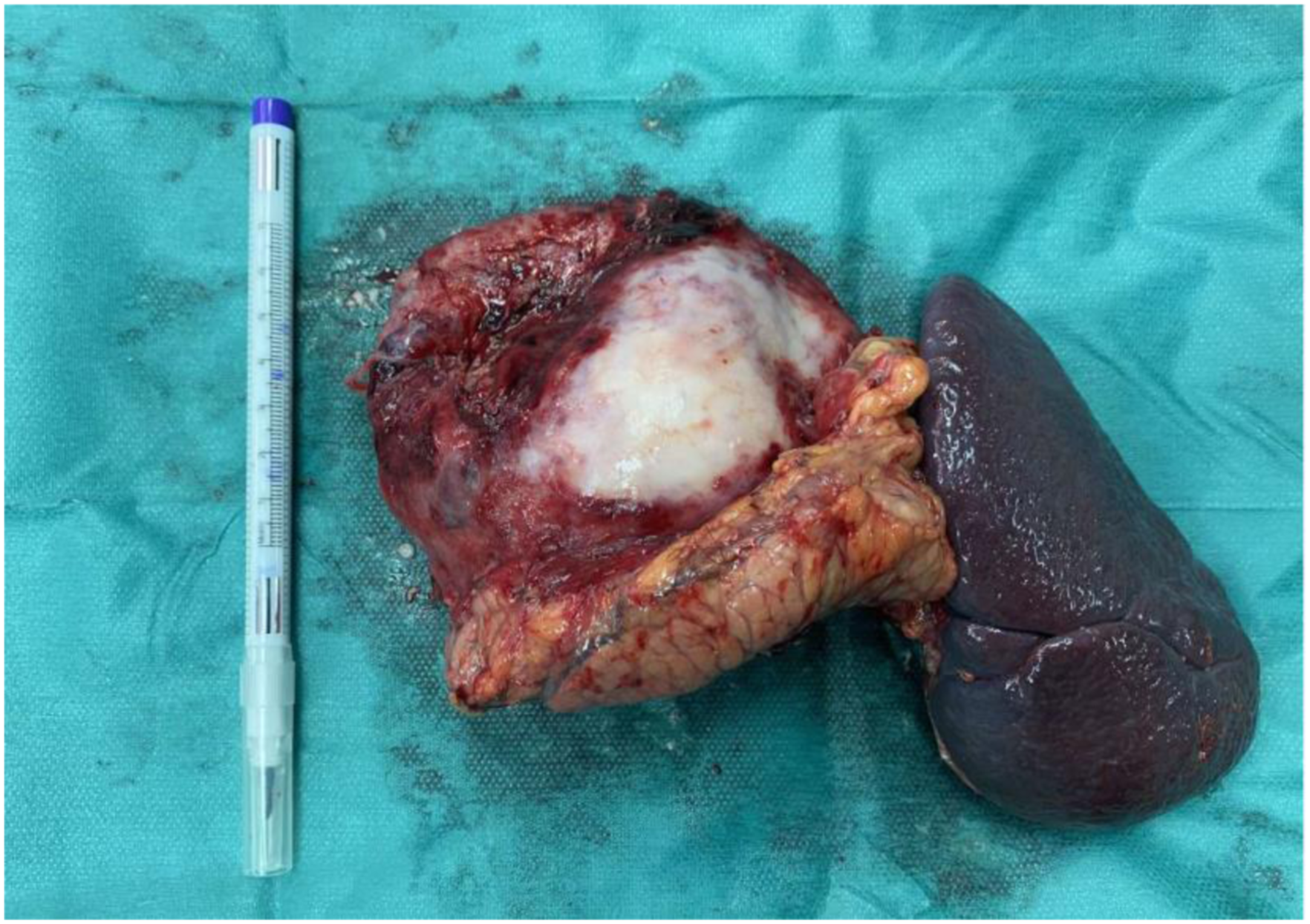
Gross examination revealed a 12 cm well-described cystic tumor with a reddish tun outer surface, covered by a thick wall. On cross-section, it was filled with keratin material and hair. Histopathological evaluation included complete sampling of the cyst wall in order to exclude the presence of immature foci indicative of malignancy. Microscopically the cyst was lined by a single layer of keratinizing squamous epithelium with sebaceous glands and dermal appendages, such as hair follicles. The cyst wall adjacent to the portions of skin contained abundant lymphoid tissue and inflammatory cells Figure 3. There was no evidence of malignancy within the cyst lining or the surrounding pancreatic tissue. Final diagnosis was that of a dermoid cyst. MDT decision was follow-up. The patient is asymptomatic with no evidence of recurrence in 4 months. (a). Gross photograph of the pancreatic dermoid cyst. (b). H-EX10 Dermoid cyst lined by stratified squamous epithelium. (c). H-EX10 Sebaceous glands in the cyst wall. (d). H&E 10x Pancreatic tissue adjacent to fibrous stoma.
Discussion
Teratomas include tissue originating from all three germ layers and are classified as mature and immature based on the presence of immature neuroectodermal elements within the tumor. 4 Mature teratomas lack the aforementioned elements and are further categorized into cystic or solid. 1 Due to the predominance of ectodermal tissue differentiation, mature cystic teratomas are also known as dermoid cysts.
Teratomas are more common among pediatric patients. Common sites include the testes and ovaries. However, they may be encountered along the body midline following the route of germ cell migration during embryogenesis. 5 Therefore, mediastinum, retroperitoneum and the sacrococcygeal region are frequent presentation sites. 6
Pancreatic teratomas are quite rare with approximately 50 cases reported in the literature. 1 There is a slight male preponderance,1,6,7 occurring usually in the fourth decade of life, ranging from 4 months old to 74 years old.1,6 The size of the teratomas reported in the literature varies, from 2.2 cm to 25 cm with an average size of around 8 cm1. The location of the mass also varies, arising mostly from the body of the pancreas followed by the head and the tail.1,8 Although patients with pancreatic teratomas may be asymptomatic, they usually present with non-specific gastrointestinal symptoms. These include diffuse abdominal pain, dyspepsia, nausea, back pain or weight loss. 8 Pancreatitis due to a mature teratoma has been reported only once in the literature. 9 Upon physical examination, an abdominal palpable mass is the most common finding for enlarged dermoid cysts. 1 There are no specific laboratory examinations for mature cystic teratomas and tumor markers are generally within normal limits. However, CA 19–9 could be elevated, 8 complicating the differential diagnosis and raising the suspicion for malignancy.
Considering that symptoms, signs and laboratory tests are non-specific, imaging modalities may assist in the preoperative diagnosis. The radiological appearance of the cystic mass depends on its tissue contents such as proportion of fat and calcifications. CT scan is able to detect cystic fluid, fat or calcifications and MRI is efficient in distinguishing soft tissue lesions and intra-tumoral fat. 1 Nevertheless, imaging studies are still nonspecific for pancreatic teratomas, as pancreatic mucinous and cystic neoplasms have similar features. 8
Therefore, accurate pre-operative diagnosis of a dermoid cyst remains a challenge and multiple imaging modalities should be combined. Differential diagnosis would primarily include pseudocysts (their fluid is homogenous on CT and MRI scans), serous cystadenomas (they mostly present with multiple cystic lesions commonly in older women), mucinous cystadenomas (they pose a significant challenge), lymphoepithelial cysts and epidermoid cysts in intrapancreatic splenic tissue. 1
In our case accordingly, the patient presented with non-specific symptoms of abdominal pain, nausea and dyspepsia. However, she also presented with new onset of dyspnea and vomiting presumably because of the expansion of the mass to the mediastinum and its effects on the esophagus. Physical examination and laboratory tests were not diagnostic and imaging modalities were inconclusive. EUS-FNA was not performed because the size of the lesion as well as the symptoms of the patient presented a clear operative indication, and the possibility of malignancy or mucinous cystadenoma raised the risk of rupture and potential spread.
Treatment options for mature cystic teratomas include external and internal drainage, cyst excision or radical surgery. 6 External drainage has been abandoned due to high recurrence and complication rates, especially pancreatic fistula. 1 Evidence regarding internal drainage is also limited. Surgical excision is the preferred treatment of choice for all pancreatic teratomas nowadays, either cystectomy or more radical resections depending on the size of the lesion, its adhesions and its anatomic relations with other organs. 7 In our case the size of the cystic mature teratoma, its relation to the body and tail of the pancreas as well as the encasement of the splenic vessels, contributed to the decision for distal pancreatectomy along with splenectomy.
Conclusion
Mature cystic teratoma of the pancreas is a rare entity with scarce data among the literature. Preoperative diagnosis is challenging even though some imaging modalities may provide useful information. An elusive diagnosis, usually leads to the operative theatre where surgical resection takes place. Clinicians should be aware of this rare entity and include dermoid cysts in the differential diagnosis for cystic lesions of the pancreas.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability
The data that support the findings of this study are available on request from the corresponding author, Nikolaos Tasis, MD, MSc, Dimitsanas 1, Athens, Greece, 11522, ntasis@agsavvas-hosp.gr