
Abstract
The incidence of malignant tumors diagnosed during pregnancy is increasing, often ascribed to the recently recognized trend that many women are postponing childbirth. Although early diagnosis is optimal for both mothers and fetuses, the diagnosis of malignant tumors during pregnancy is often delayed until an advanced stage, because generalized symptoms of pregnancy and malignancy may overlap, such as shortness of breath, chest or abdominal discomfort. The study patient was 21 years old, and 31 weeks-pregnant when she was diagnosed with primary tracheal adenoid cystic carcinoma (ACC). The patient initially presented with dyspnea and decreased blood oxygen saturation and underwent a cesarean section on the first night of hospitalization, resulting from fetal distress. This case report intended to investigate potential barriers to the timely diagnosis of tracheal ACC and consider optimal management strategies when it is diagnosed during pregnancy.
Introduction
Adenoid cystic carcinoma (ACC) is a rare cancer that most often occurs in the salivary glands. Considering head and neck ACC, the age-adjusted incidence rate is 4.5 cases per 100,000 individuals, with a slight female predominance (59%).1,2 This cancer can also arise in other locations, including the breast, skin, respiratory system, and reproductive organs. 3 Tracheal ACCs are typically slow-growing, and the patient may remain asymptomatic in the absence of airway obstruction. Because wheezing and exertional dyspnea are often initial manifestations, ACC is often initially misdiagnosed as asthma, COPD, or pneumonia. 4 Surgical resection, ideally with negative margins, often with additional adjuvant postoperative radiotherapy, is usually recommended for ACC. The overall survival at 5-year is approximately 30%, 50% when confined to intraluminal growth, but reduced to 18% with extratracheal extension. 5
Case report
The patient was a 21-year-old non-smoking female, G1P0, who had a 31-week-intrauterine single pregnancy. She initially presented to her local hospital 3 months previously with cough, expectoration, shortness of breath, and fever. Specifically, her dyspnea occurred with activity but was relieved after resting. She was diagnosed with asthma, for which she was treated, then discharged when the cough and dyspnea were relieved. Subsequently, she continued to develop cough and dyspnea with activity, but was asymptomatic at rest—a potential tipoff of partial but high-grade tracheobronchial obstruction. Otherwise, the patient had no other medical problems.
She again was hospitalized for dyspnea, 4 days before our evaluation. Her symptoms persisted despite asthma treatment, so she was transferred by ambulance to our respiratory intensive care unit. Because she remained hypoxic despite pressurized oxygen by mask, she was endotracheally intubated and mechanically ventilated. Although the patient’s oxygen saturation returned to normal, her airway pressure with mechanical ventilation exceeded 40 cm H20. She underwent urgent bronchoscopy, and an irregular tracheal tumor, with 80% obstruction of the lumen, was identified about 2 cm proximal to the tracheal bifurcation. The endotracheal tube was passed over the tracheal tumor with bronchoscopic guidance, completely relieving the airway resistance. Concurrently, however, fetal heart monitoring showed fetal distress, and rapid joint consultation of respiratory medicine, anesthesiology, and obstetrics concluded emergency caesarean section should proceed as soon as possible. Following brief communication with the family and signed informed consent of the patient, she was immediately sent to the operating room. Anesthesia was induced with propofol 2 mg/kg, remifentanil 4 ng/kg TCI, cisatracurium 0.2 mg/kg, and maintained with 2% sevoflurane + remifentanil 4 ng/kg TCI (Bis: 40–60). Four minutes after induction of anesthesia, a 1500-g premature infant was delivered by cesarean section. The 1-min Apgar score of the newborn was 6 (1 point reduction each for skin color, respiration, muscle tension, and heart rate), 8 with pressurized oxygen at 5 min (1 point reduction for respiration and skin color), and 9 with continuous oxygen at 10 min (1 point reduction for respiration). On hospital day 37, the infant was discharged, weighing 2410 g, and no developmental problems were observed at 1 year of age.
CT scan of the mother 2 days after cesarean section showed no abnormalities except thickening of the tracheal wall (Figure 1(a) and (b)). The endotracheal tube was carefully withdrawn under fiberoptic bronchoscopic control to ensure a patent airway, and tumor biopsy was obtained for pathological examination (Figure 1(e) and (f)). The histopathological results, including immunohistochemistry, confirmed the tumor was malignant (Figure 1(h)), specifically an adenoid cystic carcinoma (Figure 1(i)). CT reexamination after removal of the endotracheal tube clearly demonstrated the tracheal malignancy (Figure 1(c) and (d)). Seven days following cesarean section, the patient underwent tracheal resection and reconstruction (Figure 1(g)), from which she recovered and was discharged. One year after tumor resection, the patient had no evidence of recurrence on follow-up CT scans. Diagnostic workup, bronchoscopy, the resected specimen from the operation, histology.
Discussion
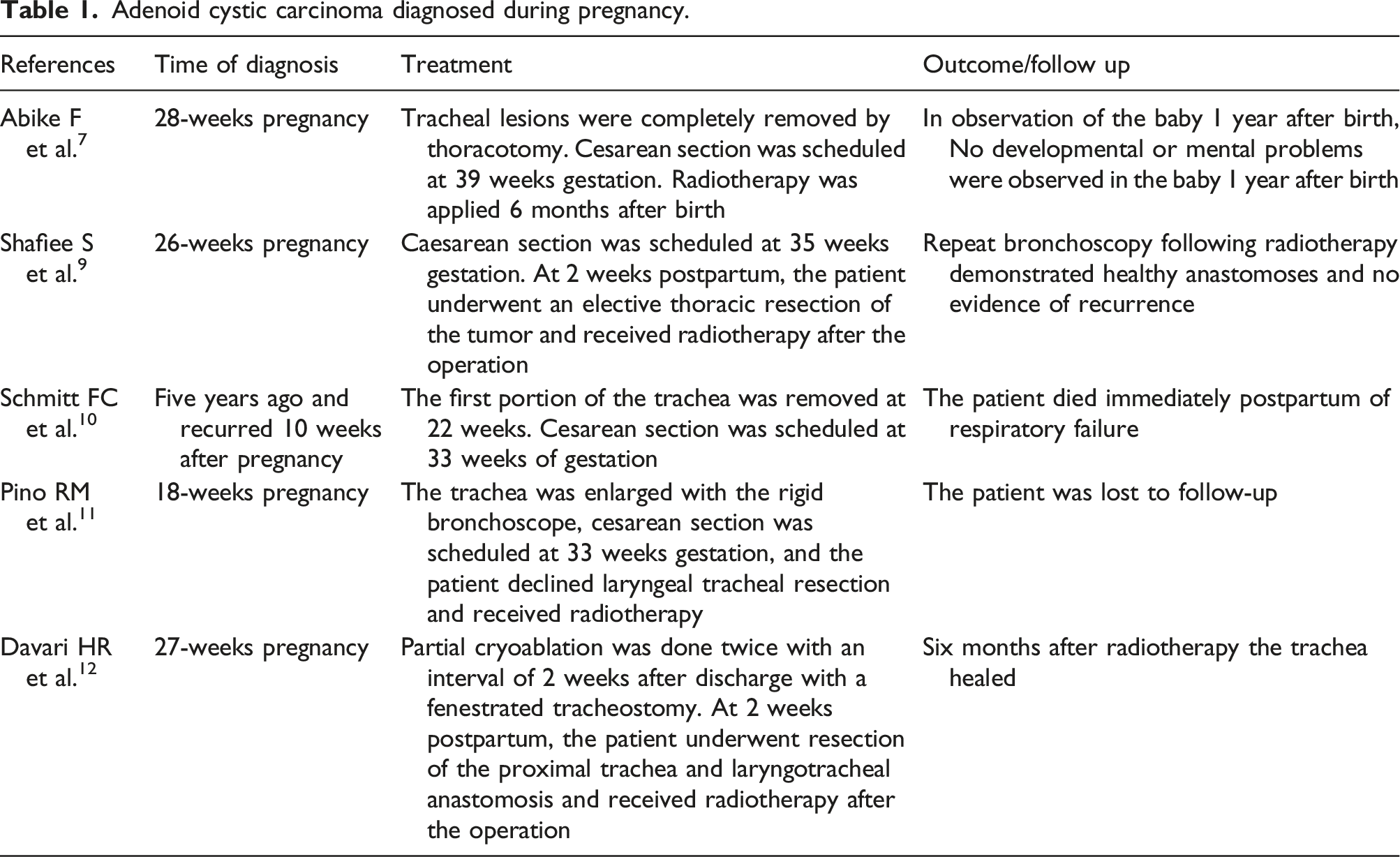
Adenoid cystic carcinoma diagnosed during pregnancy.
Although ACC is typically a low-grade malignancy, its frequent early perineural infiltration, as well as extension along the vasculature, can result in local recurrence and distant metastases. The best opportunity for achieving a long-term cure is complete surgical resection of the tumor, often supplemented by postoperative adjuvant therapy. 5 The treatment of endobronchial ACC during pregnancy becomes complicated because of the wishes of patients and their families, gestational age, local laws, religious beliefs, and medical level.
Endobronchial ACC diagnosed during pregnancy is rare, limited to case reports in the literature. Patients with pregnancy complicated by the presence of a tracheal tumor can be treated safely with surgical resection during the second trimester of pregnancy. Patients with either a slowly progressing tumor or women who are unwilling to undergo surgery in mid-pregnancy can be further evaluated to assess the degree of airway obstruction, potentially to undergo local measures to alleviate or reduce obstruction such as laser ablation, tracheal stent or other minimally invasive surgery, or accelerate fetal maturation. For patients in late pregnancy, the timing of surgery would need to carefully account for the degree of airway obstruction, tumor progression and fetal conditions. The risks of tracheobronchial obstruction can be life-threatening, compounded by risks to the fetus of imaging and operative interventions. This demands the input and cooperation of a multidisciplinary team of experts to comprehensively assess and balance maternal risks and fetal safety, and formulate optimal management strategies with participation of the patient and family.
Footnotes
Acknowledgements
We thank all co-authors for support from data collecting to revising manuscript.
Author contributions
Yongguo Xie wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Guangxi Medical and health Key cultivation discipline construction project.
Ethical approval
Ethical approval to report this case was obtained from The Second Affiliated Hospital of Guangxi Medical University Ethical Review Committee, Grant Number: 2021-KY(0328).
Informed consent
Written informed consent was obtained from a legally authorized representative for anonymised patient information to be published in this article.
Data availability
The data that support the findings of this study are available from the corresponding author, upon reasonable request.