
Abstract
Epithelioid sarcoma (ES) was first described by Enzinger in 1970. It is a rare variant of soft tissue sarcoma with a 5-year overall survival (OS) rate of 50%. Here, we reported a case of epithelioid sarcoma in the parapharyngeal space of an adult, resulting in a favorable prognosis after chemotherapy and radiation therapy. A 34-year-old female who complained of pharynx pain and discomfort was suspected of having a tumor in the right parapharyngeal space by CT scan. Excision biopsy suggested epithelioid sarcoma. Clinical and radiological studies did not reveal tumor distant metastasis in the patient. After excisional biopsy, the patient underwent chemotherapy and external beam radiation treatment. She has remained alive for 2 years and 7 months without recurrence since her last treatment. In this paper, we also provide a detailed review of the role of radiotherapy in the treatment of epithelioid sarcoma in previously reported cases.
Introduction
Epithelioid sarcoma (ES) is a rare high-grade malignancy that arises from soft tissue, characterized by a distinct clinicopathologic entity and first described by Enzinger. 1 ES accounts for less than 1% of all soft tissue sarcomas. 2 It is typically divided into two distinct types, the distal type and the proximal type. 3 The distal type usually occurs in the distal extremities of young patients. It usually manifests as a single painless and slow-growing firm nodule located in the dermis, subcutaneous tissue, or deep soft tissue. Ulceration, hemorrhage, and necrosis can be seen on the surface of the nodule. 2 In contrast, the proximal type is more common in elderly patients. It presents as a deep soft tissue mass with a large volume. 4 The size of the nodule can reach up to 20 cm in diameter, mainly located in the pelvis, perineum, genitals, etc. Epithelioid sarcoma is an aggressive malignant soft tissue tumor with a high recurrence rate, high incidence of the presence of positive regional nodes and distance metastases. It is reported that about 15%–75% local recurrence and 30%–50% distant metastasis rates, usually to regional lymph nodes and lungs.5–11
Benign and malignant tumors can occur in any structure in the parapharyngeal space. However, this tumor is exceedingly rare.12–14 To date, there are no previously reported cases of ES of the parapharyngeal space to our knowledge. Here we present a unique case of a patient with primary parapharyngeal space ES who underwent incisional biopsy followed by neoadjuvant chemotherapy, radical external beam radiation treatment, and adjuvant chemotherapy.
Case report
A 34-year-old female with a previous history of pharynx pain and discomfort presented to her otolaryngologist in June 2017. On examination, she was found to have a protrusion of the right tonsillar fossa. There was no lymphadenopathy or other abnormality on physical examination. An MRI of the pharyngeal showed a 4.5 cm × 3.0 cm × 2.0 cm soft tissue lesion in the right parapharyngeal space adjoining the carotid sheath (Figure 1). There is no thickening of the adjacent muscle or inflammation. The soft tissue lesion was close to the right carotid artery; therefore, it is hard to completely excised. This patient then underwent an open biopsy, and the specimen was sent for pathologic evaluation. The pathology was initially read as positive for undifferentiated carcinoma (Figure 2). The specimen was then sent for outside consultation, and the diagnosis was edited to epithelioid sarcoma. Immunohistochemical stains revealed the tumor to be CD34, EMA, vimentin, P16, Ki-67 positive; AE1/AE3, INI-1, INI-1, Syn, ERG, SOX-10, CK, CK5, CK7, S-100, P40, SALL4, HMB45, Desmin, MyoD1 negative.
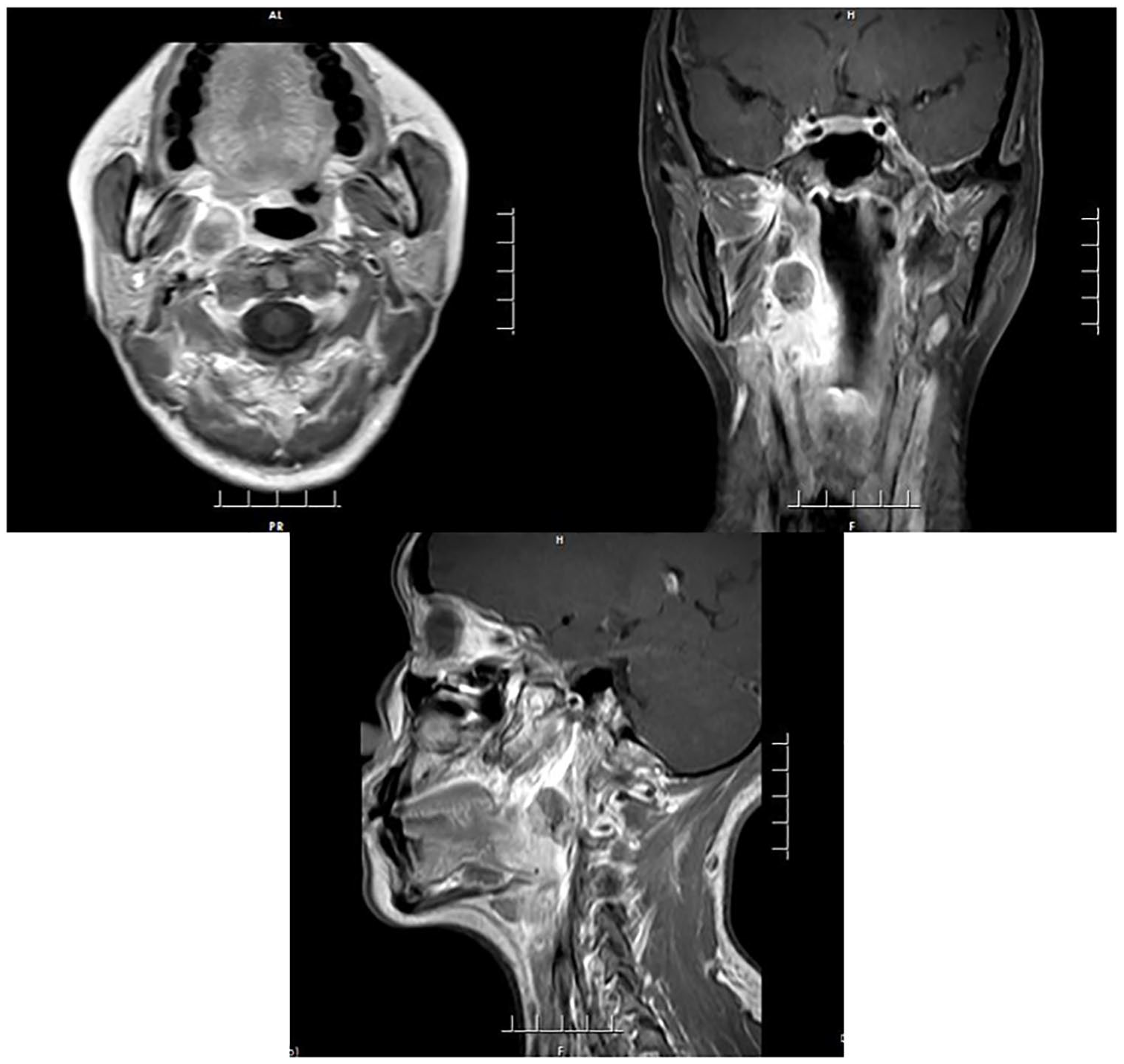
Pre-treatment MR showed a right parapharyngeal space tumor.

The histopathological examination: The tumor cells grow infiltratingly and are irregularly nested or scattered. Most of the tumor cells are spindle-shaped. (HE stained).
To complete her staging workup, Computed tomography of the head and neck showed no evidence of abnormal lymph nodes. The patient also had a PET-CT that showed no evidence of metastatic disease in the chest, abdomen, or pelvis. Thus, the disease was localized to the right parapharyngeal space.
The tumor was deemed unresectable, therefore she received three cycles of chemotherapy with Ifosfamide 1500 mg/m2 and Epirubicin 60 mg/m2 given every three weeks from August 2017 to October 2017. Restaging MRI scan of the head and neck showed a decreasing size of the right parapharyngeal space tumor (Figure 3). Due to the partial response of the disease, radical radiation therapy was recommended for the patient. From October 2017 to December 2017, she received intensity-modulated radiotherapy to the residual tumor and the lymph node area to a total dose of 74 Gy in 37 fractions and 50 Gy in 25 fractions respectively (Figure 4). During the 8-week radiation therapy, she received concurrent chemotherapy of Ifosfamide 1500 mg/m2 given every three weeks. She tolerated her concurrent chemo-radiotherapy well with moderate toxicity, including pharynx pain and myelosuppression. The tumor was not detectable after concurrent chemo-radiotherapy. A follow up restaging MRI scan of the head and neck showed a complete response of the right parapharyngeal space tumor (Figure 5). The CT scan of the chest, abdomen, and pelvis showed no evidence of metastatic disease. Then adjuvant chemotherapy was recommended. From January 2018 to April 2018, she received other four cycles of chemotherapy with Ifosfamide and Epirubicin given every three weeks.
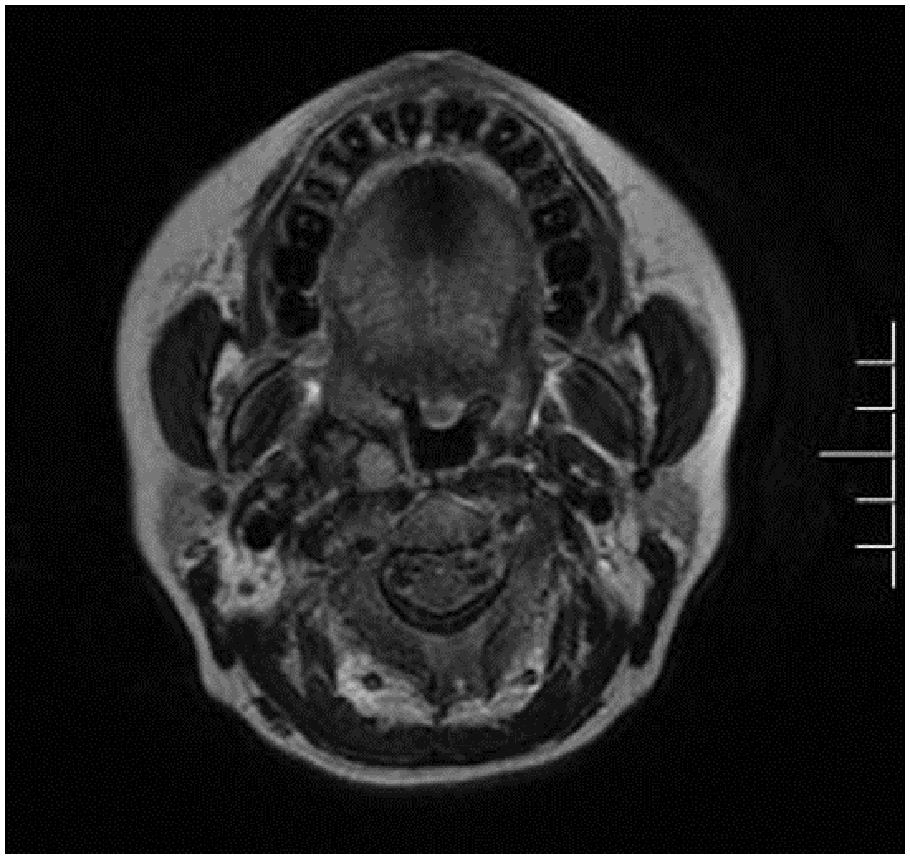
MR after neoadjuvant chemotherapy showed a partial response of the right parapharyngeal space tumor.

Axial CT, sagittal CT and coronal CT showing isodose lines for the right parapharyngeal space radiation treatment fields.

Post-treatment MR showed a completed response of the right parapharyngeal space tumor.
The patient has recovered well from her prior treatment course. She is now 40 months out of her diagnosis.
Discussion
Primary parapharyngeal space sarcoma is rare in among all malignant neoplasm. 15 Parapharyngeal space tumors account for only 0.5% of head and neck tumors. 16 Clinically, surgical resection is usually used for the treatment of parapharyngeal space tumors. The anatomical structure of the parapharyngeal space is complex, with abundant blood vessels and nerves. Pathological diagnosis is often lacking before surgery, and clinical diagnosis and treatment is difficult.16–18
Epithelioid sarcoma is a rare neoplasm of unclear origin, first well-characterized by Enzinger. 1 With further research, Guillou et al. 19 had defined proximal epithelioid sarcoma (PES) in 1997 according to the different occurrence site and found that the proximal type and the distal type (also known as the classic type) exhibit great differences in histological characteristics and biological behavior. Epithelioid sarcoma is recognized in less than 1% of soft tissue sarcoma patients. 2 Distal epithelioid sarcoma is the canonical subtype of the disease, usually occurs in young and middle-aged adults aged 10–35 years. The most common localization is in the extremities, especially the hands or forearms, followed by the knee joints, lower limbs, buttocks, and feet. 3 While proximal type is more common in the middle-aged and elderly population with a median age of 40 years when diagnosed. Proximal subtype developed mostly in the pelvis, genitals, and perineum.20–22 Besides, few cases reported that the neoplasm localized in the small intestine, parotid gland, palate, or orbit.23–26
In recent decades, most of the literature related to ES are case reports while only a few large-scale cases analysis. Because of its low incidence and the lack of understanding by clinicians and pathologists, misdiagnosis and mistreatment are quite common in clinical practice.
For the treatment of epithelioid sarcoma, radical excision is the preferred choice. 2 It is currently believed that compared with limb salvage surgery, amputation surgery cannot improve the patient’s prognosis. If the local tumor cannot be removed entirely, the recurrence rate and mortality will increase.2,27 Therefore, radical surgery and perioperative radiotherapy or chemotherapy are still the treatment standards for ES patients. 3
Radiotherapy is rarely used clinically and its application in ES treatment is still controversial. The potential benefit of radiation therapy alone or combined with chemotherapy is not well defined. Compared with other soft tissue sarcomas, ES is generally considered to be insensitive to radiotherapy. There are limited data on radical radiotherapy or perioperative radiotherapy for ES. Radiotherapy is often used as an adjuvant to surgery. Callister et al. 28 reported 24 non-metastatic ES patients, the largest number of cases so far, with perioperative radiotherapy and surgical treatment. Only three patients received neoadjuvant radiotherapy to a total dose of 46.4Gy. The rest of the patients received postoperative radiotherapy, with a median total dose of 64.5Gy. Disappointingly, seven patients (29%) experienced local treatment failure. Compared with other soft tissue sarcomas with a local control rate of more than 80%, this result does not seem satisfactory.
Another study published by Wolf et al. 29 reported similar findings. Between 1990 and 2003, 11 patients (nine men and two women) with epithelioid sarcoma were included in their study. Primary treatment consisted of surgery in all 11 patients. None underwent neoadjuvant radiotherapy. Nine patients underwent postsurgical radiotherapy, seven patients after their initial surgical excision, and two patients after excision of local recurrences. Among the seven patients with primary ES who received adjuvant radiotherapy after initial surgical excision, five of them (71%) had local recurrence. In addition, the paper concluded adjuvant radiotherapy and chemotherapy did not affect disease-free survival.
A study published by Shim and Suit 30 showed the potential benefits of perioperative radiotherapy and radical radiotherapy in the treatment of ES. The authors treated eight patients (four men and four women) with ES. Five patients received postoperative radiotherapy followed by surgery for primary or recurrent tumor (three patients had primary tumors and two patients had recurrent disease) without a history of radiotherapy. One patient received neoadjuvant radiotherapy. Among the above six patients, only one had local recurrence. The remaining two patients received radical radiotherapy without surgery. One patient’s primary tumor was about 22 cm in size and died of persistent local disease and distant metastasis at 6 months. Another patient with a forearm recurrence achieved sustained local control. However, this patient developed distant metastases eventually.
Like radiotherapy, chemotherapy is also used as an adjuvant to surgery. Perioperative chemotherapy of ES is reported in some published studies. It is mainly used for large-sized and high-grade tumors, with or without complete resection and/or metastasis.9,31 Anthracycline-based combination regimens (doxorubicin or epirubicin with ifosfamide or dacarbazine) have been used for patients with advanced, unresectable, or metastatic disease. 32
Currently, there are extremely limited case reports on the treatment of ES patients with radiotherapy and chemotherapy alone or combined. While neoadjuvant or adjuvant radiotherapy and chemotherapy in soft tissue sarcomas are highly reported, their roles in ES management are worthy to investigate extensively. In our present case, the neoplasm localized in the right parapharyngeal space infiltrated with blood vessels, the disease area was considered unresectable. Therefore, we performed radiotherapy and chemotherapy for this patient, and this combination therapy turned out to be effective and tolerated. The patient gained excellent long-term local control and disease-free survival. Our clinical experience shows that concurrent radio-chemotherapy may be a viable radical treatment option for unresectable ES. The effectiveness of radiotherapy was demonstrated in this case. There should be more studies to confirm the sensitivity of ES to radiotherapy and chemotherapy.
Footnotes
Authors contribution
Yun-Tian Li: Drafting the paper. Wen-Guang Luo: Treatment of the patient. Hong-Yan Zhang: Editing the paper.
Declaration conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval to report this case was obtained from * Anhui Provincial Hospital Medical Research Ethics Committee *.
Informed consent
Informed consent for patient information to be published in this article was not obtained because a waiver of informed consent had been obtained from * Anhui Provincial Hospital Medical Research Ethics Committee *.