
Abstract
We report a case of prostate carcinoma with wide nuclear expression for p63. These cases are rare and show atypical cytoplasmic/membrane expression of Ck5/6, alpha-methylacyl coenzyme A racemase and high-molecular-weight cytokeratin. It is rare to find this type of carcinoma with negativity for Ck5/6. We would like to present this case to avoid a diagnostic pitfall and with review of literature to understand the origin of this rare subtype.
Introduction
The glandular tissue of the prostate includes secretory cells on the side facing the glandular cavity and basal cells on the basal side. Prostatic adenocarcinoma presents typically as acinar adenocarcinoma with luminal phenotype which expresses androgen receptor and low molecular weight cytokeratin (Ck8/18), while the basal cell markers (P63, Ck5/6 and high molecular weight cytokeratin) are not expressed. 1 On the other hand, there is proliferation of the basal cells, which varies from hyperplasia to carcinoma of the basal cells, which is extremely rare. 2 It is characterized morphologically by the presence of nestes and small cysts, as seen in adenoid-cystic carcinoma, which is considered to be the most important differential diagnosis. 3 This is in contrast to a rare group of unusual prostatic adenocarcinoma which presents nuclear p63 expression without basal distribution and morphology. 4 This rare group originates from secretory luminal cells with abnormal positivity of p63. In about 36% of reported cases, there was weak positivity for Ck5/6. 1 We report this case to avoid misinterpretation and diagnostic pitfall.
Case report
Patient presentation/ history: A 67 years old patient presented with PSA level in serum (2.47 ng/ml (<3.7)). No history of other tumors.
Clinical examination and diagnostic investigations: These were done to exclude any other body tumors and to exclude the possibility of metastasis from other organs. There were hard foci in the left side of the prostate.
Method of diagnosis: A standard method to take slender (Core) biospies from the anatomical parts of the prostate was done. The Core biopsies are histologically proceeded with standard methods and stained with hematoxylin and Eosin (H&E) as well as with PAS (periodic acid-Schiff). After careful microscopic examination and the investigation of the serial sections as well as the conventional (H&E) and special stains (PAS), we have found in six core biopsies (6/12) an infiltration by small irregular pleomorphic cells and small acini that are formed by cubical cells with large nuclei and prominent nucleoli. The special stain (PAS) showed an intracytoplasmic mucin production.
There was morphologicaly no doubt about an infiltration with acinar adenocarcinoma of the prostate (Figures 1) but to be sure of the diagnosis, we have investigated the cores immunohistochemically against p63, alpha-methylacyl coenzyme A racemase and Ck5/6. Our immunohistochemical stains were done as standard description from DaKo.

Small irregular pleomorphic cells and small acini that are formed by cubical cells with large nuclei and prominent nucleoli.
Surprisingly, the tumor cells expressed nuclear positivity for p63 (Figure 2) and showed cytoplasmic reactivity for alpha-methylacyl coenzyme A racemase (Figure 3). Ck5/6 was not expressed (Figure 4). Little is known about this rare type. Finally, we could exclude infiltrating urothelial carcinoma by the lack expression of GATA-3 (Figure 5). To ensure the diagnosis, we have stained the tumor cells with androgen receptor (Figure 6) and this was positive. There is no positivity for p53. To get a suggestion for immunotherapy, we have stained the tumor with PDL-1 but this was negative and there is also negativity for ALK-1.

p63.
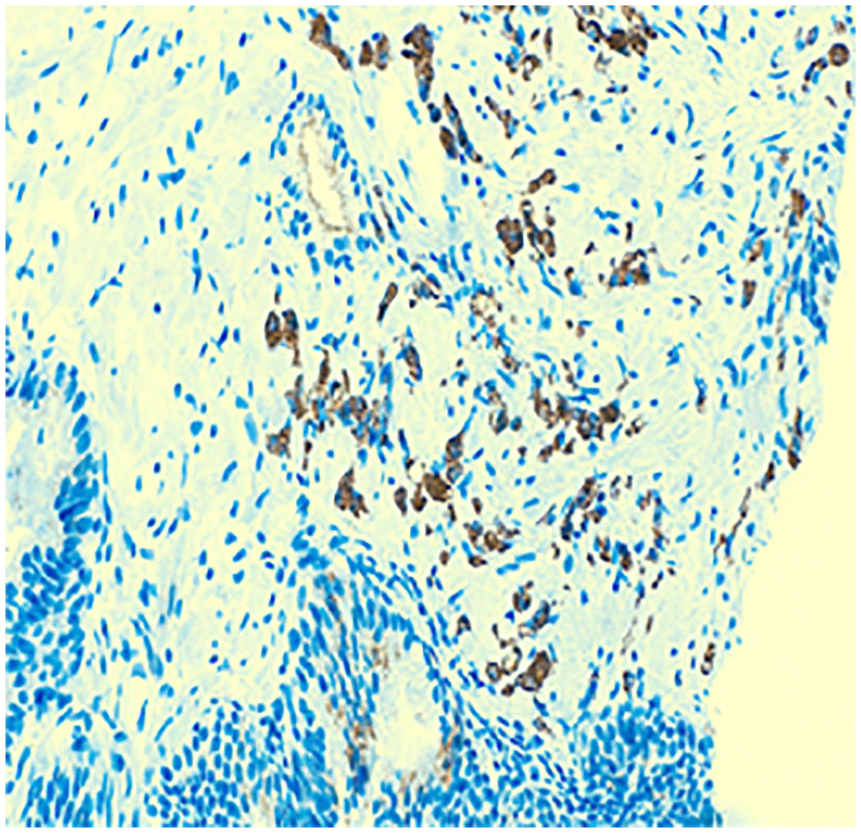
P504s.

CK5/6.
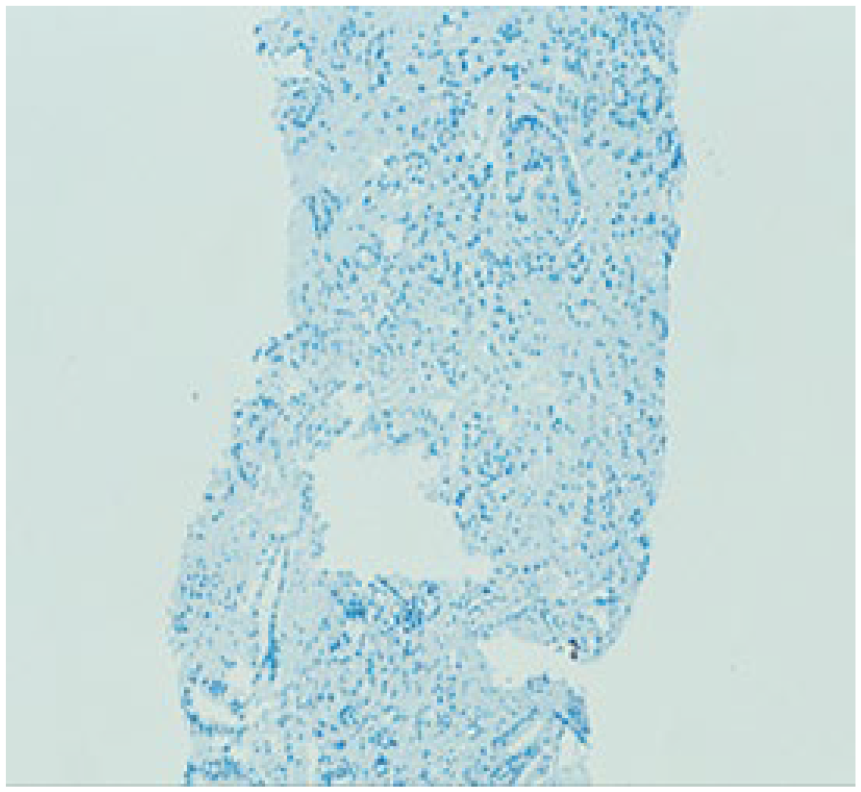
GATA-3.

Androgen R.
The standard Treatment in this case was prostatectomy and follow-up.
Discussion
We present here a rare case of prostate carcinoma with abnormal expression of p63 which is described in some literature to be found in the basal subtype of prostate carcinoma with coexpression of Ck5/6. However in our case, there is no co-expression of Ck 5/6.
Usual prostatic adenocarcinomas have a luminal-type immunoprofile, lacking basal markers such as p63 and high molecular weight cytokeratins, and diffusely expressing low molecular weight cytokeratins.
Fonseca-Alves et al. 5 have discussed the unusal type of prostate adenocarcinoma with positivity for p63 but they have described the coexpression of Ck5/6 and emphasized that the tumors of the prostate with p63-positivity have had a higher Ck5/6 expression level compared to p63 negative tumors. In our case, we are trying to emphasize that there is another subtype with no expression of Ck5/6.
In a previous work of Hsueh-Li Tan et al., 1 they have described also the p63 positive adenocarcinoma of the prostate with co-expression of Ck5/6 in about 36% of cases but they did not focus on the negativity of Ck5/6 and they have not discussed the reason.
Ali and Epstein (2008) have reported another subtype of prostate cancer with positivity for p63 but with morphological proliferation of basal cells in nests and small cysts, like seen in adenoid-cystic carcinoma. In our case, there is no morphological similarity with the basal cell carcinoma and there are no features like adenoid cystic carcinoma.
It was suggested by Hsueh-Li Tan e al. 1 that p63-expressing carcinoma may be molecularly different from the usual adenocarcinomas in part because they originate from a rare basal tumor initiating cell population, which has undergone partial, but incomplete differentiation towards a luminal phenotype. In the recent version of WHO, 6 this type of carcinoma was shortly described with the hypothesis that there is different molecular pathway by the work of Giannico et al. 8 (2013). In this version of WHO, 6 there were no specific guidlines for the therapy, however the suggestion was that it is another molecular pathway of this subtype. In Rosai and Ackermans’s surgical pathology, 7 there is the same suggestion, that this rare type of prostatic adenocarcinoma has distinct molecular changes but there is no guidlines for therapy and there is no background or aspects of the prognosis.
Until now, this rare type of prostatic adenocarcinoma is still not really understood and our intention in this work is to focus on this subtype. Wide deeper molecular studies should be done to understand the pathway and the correct origin of these cells. Long follow-up of these cases should be done to understand the prognosis and to make a narrow comparison with the conventional acinar adenocarcinoma of the prostate. When we make both, we will be able to decide the type of therapy.
Footnotes
Acknowledgements
We thank Miss Sandra Minns (CT, IAC – Institute for Pathology and cytology-Schuettorf) for proofreading the manuscript.
Authors’ note
We would publish this interesting case to support the diagnosis and to avoid misinterpretations.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The Institution does not require ethical approval for reporting this individual case as it is anonymized. The authors have the verbal approval from the urologist and the urologist has had the verbal approval from the patient.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.