
Abstract
Malignant melanoma of the lacrimal sac is an exceptionally rare tumor with a poor prognosis. We report two cases of malignant melanoma of the lacrimal sac: a 73 year-old female treated with primary surgical resection and a 75 year-old male treated with surgical resection, adjuvant proton beam radiotherapy, and adjuvant immunotherapy. We discuss the role of post-operative proton beam therapy and recent advancements in immunotherapy. These cases highlight the importance of early diagnosis and multi-modality treatment in this aggressive malignancy.
Introduction
Malignant melanoma of the lacrimal sac is a rare cancer, with fewer than 50 cases reported in the literature. Its etiologic and pathologic origins are not well understood, as melanocytes are not native to the lacrimal sac epithelium. Currently, malignant melanoma of the lacrimal sac is thought to be derived from the neural crest or melanocyte migration from the conjunctival sac during embryologic development. 1 It has an insidious onset, often mimicking chronic dacryocystitis, leading to misdiagnosis and delayed treatment. Thus, it is typically more aggressive than its cutaneous counterpart. 1 The rich vascular supply of lacrimal structures, low host reaction, and risk for tumor seeding during excision have been cited as contributing factors towards the poor prognosis of lacrimal sac melanoma. 2 Due to the rarity of this tumor, there are currently no consensus guidelines and treatment is based on case reports. In a review of 30 patients by Subramaniam et al., 3 29 were treated with surgery through wide local excision or dacryocystorhinostomy, with 11 of these followed by adjuvant radiotherapy (ART). Here, we report two cases of malignant melanoma of the lacrimal sac treated at our institution, including one with proton beam radiotherapy, and review the published literature of lacrimal sac melanoma treated with ART.
Case reports
Case 1
A 73 year-old Caucasian woman presented to the clinic with fullness in the left medial canthal region. She had a history of congenital melanosis which was actively monitored and had been previously treated with cryotherapy. A biopsy of the left medial canthus 3 months later confirmed a diagnosis of malignant melanoma. MRI of the head and orbits revealed a 1 cm × 1 cm enhancing lesion extending from the medial canthus of the left orbit posteriorly into the left postseptal space, medially into the anterior left ethmoid air cells, and inferiorly into the superior margin of the left nasolacrimal duct. A month later, she underwent a subtotal exenteration of the left orbit, left superficial parotidectomy, left selective neck dissection areas I and II, and left medial maxillectomy. All margins were negative for tumor. She did not receive ART or systemic therapy. She remained disease-free until her death 4 years later of a thoracic aneurysm unrelated to the malignant melanoma.
Case 2
A 75 year-old Asian man presented with a 1 year history of right lower eyelid bump accompanied by intermittent epiphora and bloody drainage of the right eye. An MRI of the orbit revealed dilation of the right lacrimal sac. Two months later, he underwent a right dacryocystorhinostomy, with positive margins. Pathology confirmed malignant melanoma and immunohistochemical stains showed strong positivity with SOX-10, with focal positive staining for melan-A and S100. Post-resection PET/CT revealed mildly increased uptake in the right nasolacrimal duct nonspecific for inflammation or residual disease; no distant metastases were noted.
He underwent oncologic resection 4 months later. Pathology demonstrated malignant melanoma with ulceration of the right inferior meatus under the bulb of Hasner, 1 mm in depth. Margins were negative for malignancy. He underwent additional resection of right periorbital soft tissue to ensure complete resection of tumor-seeded areas with all specimens negative for melanoma.
Given the high-risk features including this particular subtype and the presence of ulceration, adjuvant proton beam radiotherapy and concurrent immunotherapy were recommended. The patient received 200 mg of IV pembrolizumab every 3 weeks. After receiving 3780 cGy of out of a planned course of 5940 cGy in 180 cGy fractions with proton beam radiotherapy (Figure 1), the patient was found to have innumerable small, low-attenuation masses in the liver, concerning for metastatic disease; biopsy of a liver mass confirmed metastatic melanoma. Upon histologic confirmation of metastasis, radiotherapy was discontinued. Treatment toxicities included CTCAE v4.03 4 grade 1 dry mouth, fatigue, edema, and grade 2 conjunctivitis, dry eye, and radiation dermatitis. Following five cycles of pembrolizumab, the patient developed progressive disease in the liver as well as in the pelvis, lumbar spine, and thoracic spine. Two months later, the patient was started on dual immunotherapy with ipilimumab (1 mg/kg) and nivolumab (3 mg/kg); he completed one cycle before it was held for evaluation of pulmonary infiltrate due to concern for autoimmune pneumonitis.
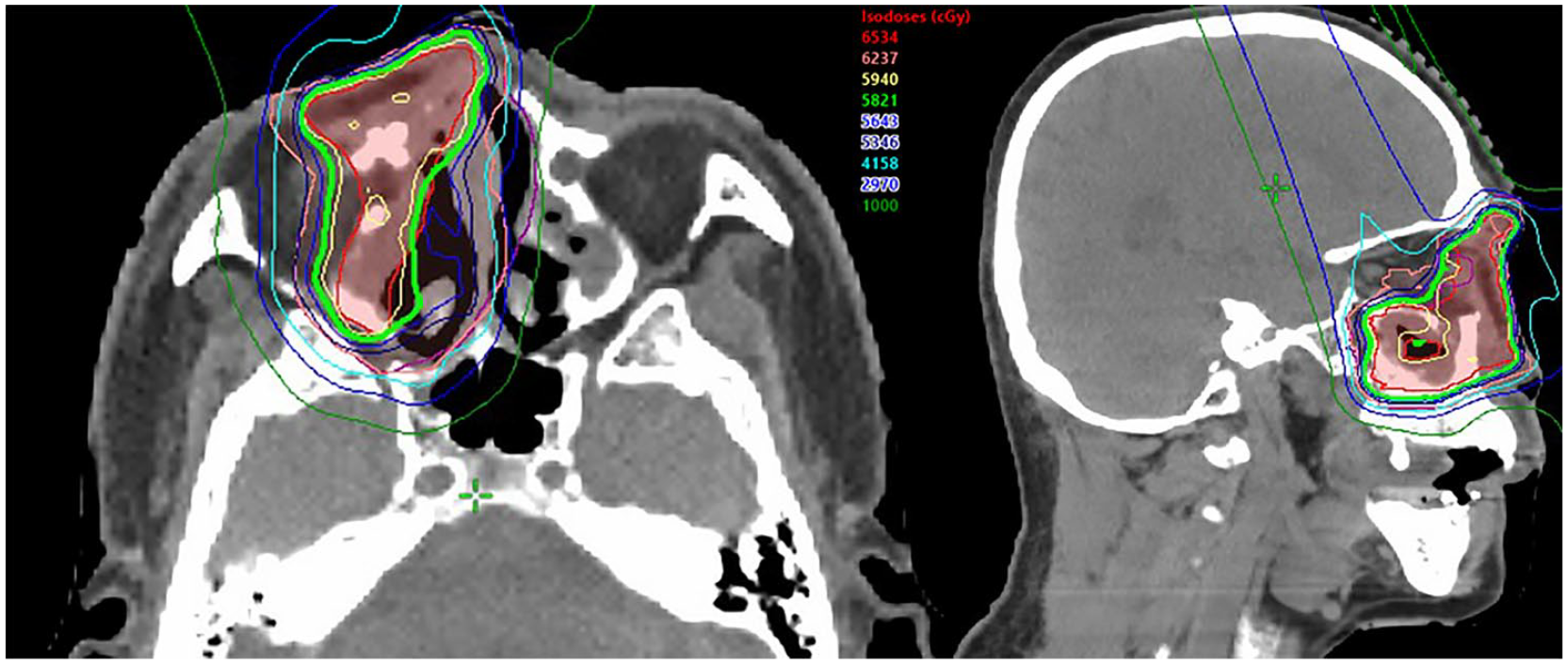
An axial (left) and sagittal (right) dose distribution of the proton beam radiotherapy plan.
Discussion
These two cases highlight the heterogenous natural history typically seen in malignant mucosal melanoma. While our first case illustrates the importance of early detection in achieving local control and overall outcome, our second case demonstrates the insidious character of this disease leading to rapid progression of distant metastases.
In malignant melanoma of the lacrimal sac, delayed diagnosis can be due to nonspecific signs and symptoms which can mimic other common conditions, such as chronic dacryocystitis. 5 McGrath and O’Hagan 6 report that out of 20 cases, the most common symptoms at presentation are bloody discharge/tears (44%), palpable mass (42%), and epiphora (38%). In the first case, vigilant workup following detection of a palpable mass led to early diagnosis and treatment, resulting in prolonged disease control. However, in the second case, the patient did not seek medical attention due to relatively benign and nonspecific symptoms and developed rapidly progressive metastatic disease. As early diagnosis and intervention are important predictors of survival, as illustrated by Case 1, we encourage providers to consider malignant melanoma of the lacrimal sac in patients who present with these symptoms.3,7
En bloc resection of the lacrimal drainage apparatus and the surrounding parenchyma has been included in various treatment strategies to achieve local tumor control and enhanced patient survival and was utilized in both of our cases. 7 The role of ART in lacrimal sac melanoma remains unclear due to the rarity of this disease. 3 Approximately 17 cases of malignant melanoma of the lacrimal sac treated with ART have been reported in the literature (Table 18–16). Our first patient did not undergo ART and remained disease-free, while our second patient was found to have distant metastases during ART.
Review of cases of malignant melanoma of the lacrimal sac treated with adjuvant radiotherapy.
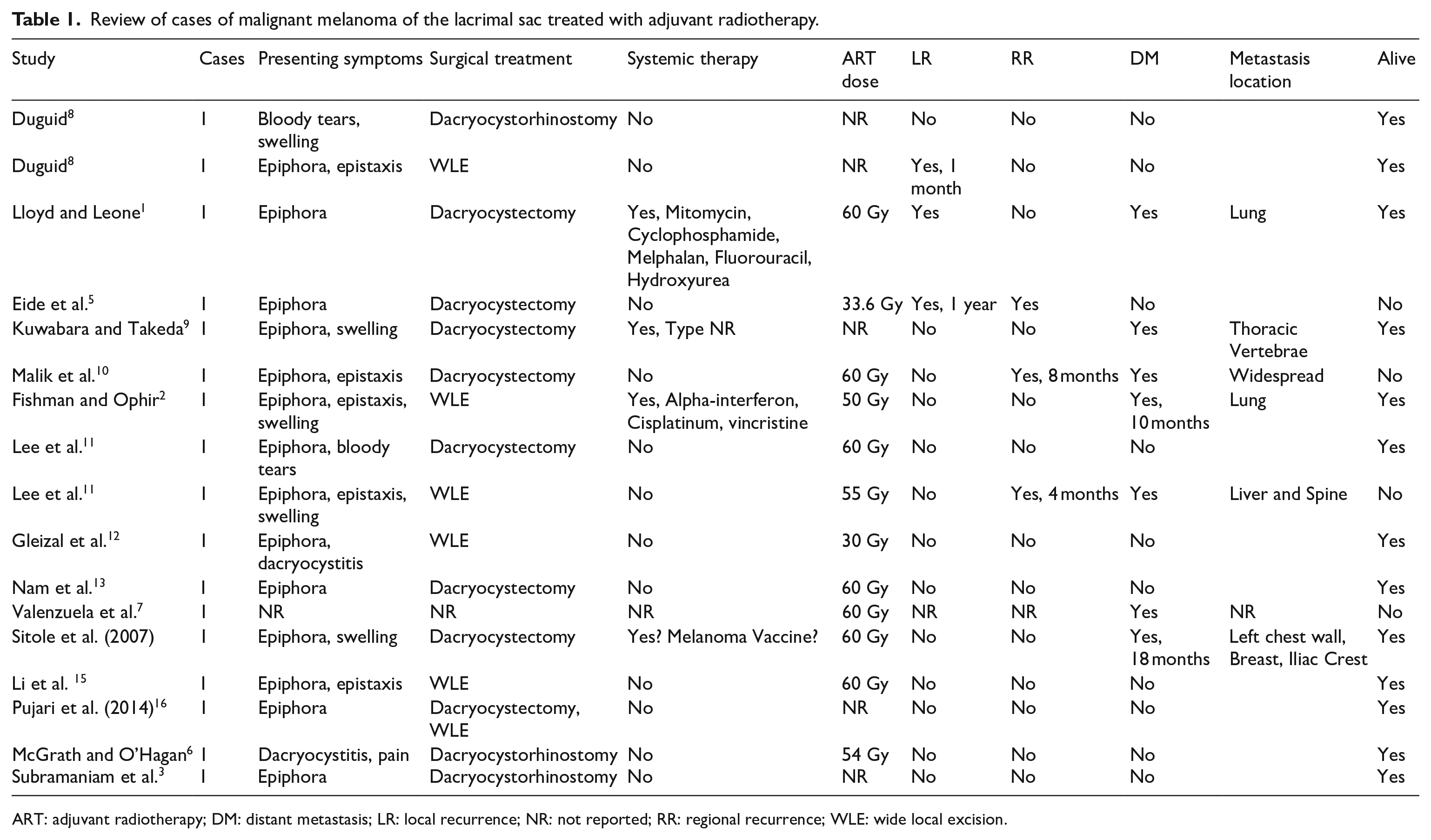
ART: adjuvant radiotherapy; DM: distant metastasis; LR: local recurrence; NR: not reported; RR: regional recurrence; WLE: wide local excision.
Additionally, due to the proximity of critical intraorbital and intracranial structures, radiotherapy of the lacrimal sac region remains a challenge due to potential high-grade toxicities. 6 For this reason, proton beam radiotherapy was utilized in our second patient as it allows for improved dose conformality. Since the radiotherapy course was not completed in our second case, it is difficult to evaluate the safety and efficacy of adjuvant radiotherapy in this setting. However, there is evidence that proton beam therapy leads to significantly higher 5-year survival and locoregional control for malignant tumors of the nasal cavity. 17 Given the proximity of the lacrimal sac to the nasal cavity, this site may benefit from further exploration into the usage of highly conformal radiotherapy techniques in disease management.
Based on the current literature, the local recurrence rate for malignant melanomas of the lacrimal sac treated with ART is approximately 17.65% (Table 1). Additionally, the rate of distant metastasis for melanomas of the lacrimal sac treated with ART is approximately 41.18% (Table 1). Although long-term outcomes cannot currently be assessed, the propensity for metastasis is demonstrated in our second case.
Currently, adjuvant systemic therapy for mucosal melanomas is largely based on experience with cutaneous melanomas. Recent advances in the development of immune checkpoint inhibitors show potential in improving prognosis and survival for patients with cutaneous melanomas. Patients with high-risk, resected cutaneous stage III melanoma have a significantly longer recurrence-free survival with adjuvant pembrolizumab when compared to placebo. 18 CheckMate 238 evaluated the efficacy of nivolumab versus ipilimumab for 238 patients with resected IIIB/C or IV cutaneous melanoma; the three-year progression-free survival was 58% versus 45% with nivolumab versus ipilimumab, respectively (p < 0.0001). 19 Limited data exists for patients with high risk stage II melanoma, leaving the role of adjuvant therapy undefined.
Immunotherapy plays a significant role in treatment of metastatic melanoma. Combination therapy with nivolumab and ipilimumab in metastatic cutaneous melanoma has demonstrated prolonged long-term overall survival. The 5-year OS for patients treated with both nivolumab and ipilimumab was 52% compared to 44% for nivolumab only and 26% for ipilimumab only. 20 In a subgroup analysis of KEYNOTE-001, −002 and −006, 84 patients with advanced mucosal melanoma were treated with pembrolizumab demonstrated an objective response rate (ORR) of 19% with a 27.6 month median duration of response regardless of prior ipilmumab. 21 Although the ORR was reduced in patients with mucosal versus cutaneous melanoma (ORR 19% vs 33%), pembrolizumab may provide clinical benefit for patients with metastatic or advanced mucosal melanomas. Given the rapid development of metastasis in our second patient, starting immunotherapy immediately after resection may have been a consideration; however autoimmune pneumonitis was a treatment-limiting toxicity. Combined therapy with ipilimumab and nivolumab should be considered due to the highly aggressive nature of lacrimal sac melanoma, and further studies are needed to define the role of immunotherapy in these patients.
Ultimately, early diagnosis and treatment remains a crucial predictor of improved survival for patients diagnosed with lacrimal sac melanoma. This is demonstrated in our first case where close surveillance of melanosis led to prompt diagnosis and treatment of our patient’s malignant lacrimal sac melanoma, allowing for prolonged survival and a lack of local or distant recurrence. The role of radiotherapy remains controversial; however, it may positively contribute to local disease control. Proton beam therapy allows for more precise targeting of malignant tissue, as seen in our second patient. The interval discovery of distant metastasis in our second case demonstrates the aggressive nature of the disease and prompts future examination into the role of early systemic therapy.
Conclusion
Overall prognosis of malignant melanoma of the lacrimal sac largely depends on early detection and aggressive treatment. Surgery is considered standard of care in the management of this disease; the role of ART is unclear. Given the location of the tumor, proton beam therapy is an attractive conformal radiotherapy option. Immunotherapy is a promising systemic therapy option.
Footnotes
Contributorship
NY and TC researched literature and conceived the study. TC wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Ethical approval
Ethical approval to report this case series was obtained from the Mayo Clinic IRB.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent for patient information to be published in this article was not obtained because research was conducted with deidentified information and approved by the Mayo Clinic IRB.