
Abstract
A 32-year-old man with vague abdominal pain was found to have enlarged para-aortic and mediastinal lymph nodes on computed tomography. He was diagnosed with retroperitoneal mixed germ cell tumor as confirmed on percutaneous biopsy. At the time of diagnosis, lactic dehydrogenase, human beta-chorionic gonadotropin, and alpha-fetoprotein were elevated. He completed four cycles of platinum-based chemotherapy with excellent response and no clinical disease progression. Three years later, he presented to the Urology clinic with a right testicular mass. His tumor markers remained negative. He was taken for a right radical orchiectomy with the pathology resulting in pure seminoma (pT1Nx).
Introduction
Approximately 3%–7% of germ cell tumors are of extragonadal origin. 1 Despite treatment and remission of extagonadal germ cell tumor, long-term surveillance is prudent given the risk of delayed testicular tumor.
Case report
A 32-year-old man presented with abdominal pain and was found to have enlarged para-aortic and mediastinal lymph nodes on computed tomography of the abdomen and pelvis (CT A/P). A retroperitoneal biopsy of the lymph nodes was consistent with mixed germ cell tumor. At the time of diagnosis, lactic dehydrogenase, human beta-chorionic gonadotropin, and alpha-fetoprotein were all significantly elevated. Testicular ultrasound and testicular exam were both normal at the time. He received four courses of chemotherapy (etoposide and cisplatin) with excellent response and no clinical disease progression. Three years later, he developed a 6-cm right testicular mass concerning for malignancy. His tumor markers remained negative. A scrotal ultrasound confirmed a 6-cm right testicular mass (Figure 1). A right radical orchiectomy was performed and histology revealed seminoma with negative margins (pT1Nx). The gross pathology is shown in Figure 2. A staging CT A/P revealed a concomitant new 3-cm right retroperitoneal mass and other enlarged para-aortic lymph nodes (Stage IIB). Biopsy of this mass confirmed metastatic pure seminoma for which he underwent 3500 cGy to area of gross disease and 2500 cGy to para-aortic and right iliac nodes. At 1-year follow-up, imaging demonstrates remission of retroperitoneal malignancy.

Representative sonographic image shows intratesticular 6 cm mass.
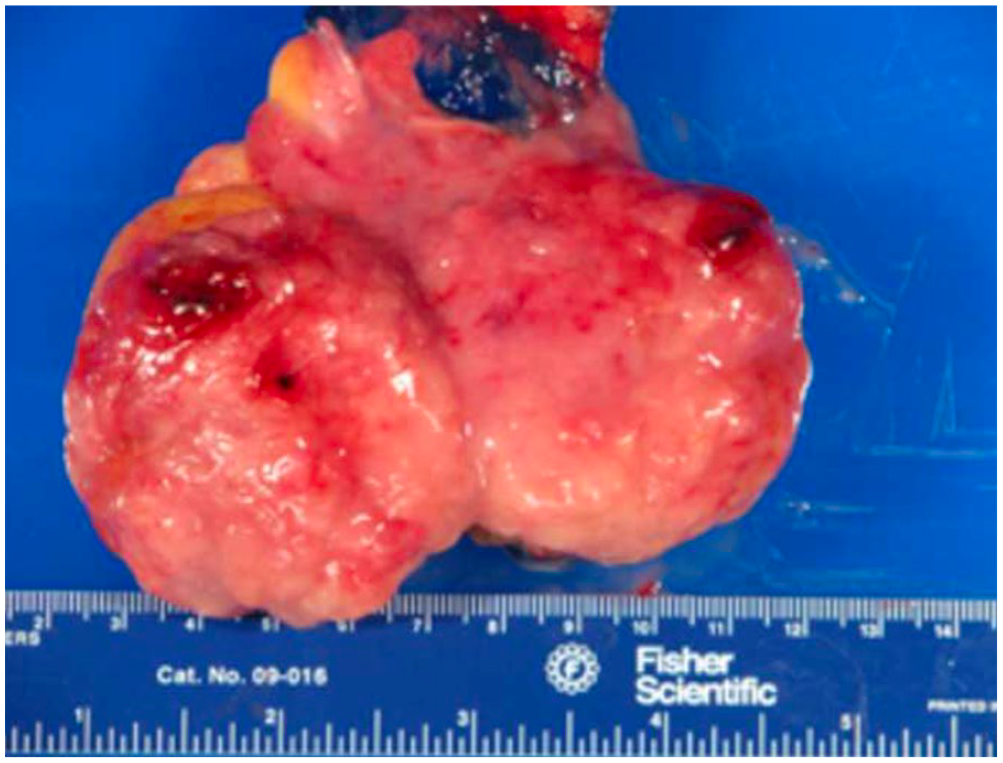
Gross pathology of right testicular seminoma.
Discussion
Long-term outcome of metachronous testicular tumor (MTT) after treatment of extragonadal germ cell tumor (EGCT) is quite limited due to the rarity of the disease. Furthermore, there is no consensus on a surveillance protocol for MTT given the infrequency of this phenomenon. Gonzalez Quintela et al. 2 reported the first case of MTT 7 years out after treatment and remission of the primary extragonadal germ cell tumor. Several case reports have shown that the median time of delayed presentation of MTT can range between 14 and 102 months with an average of 60 months after treatment of EGCT.1,3–8 There is often histological disagreement between EGCT and MTT as EGCT tend to be non-seminomatous, while MTT tend to be more seminomatous in nature.1,6
MTT can occur after treatment and remission of EGCT. Despite immediate surveillance ultrasound and tumor markers being normal, the onset of a testicular mass can be abrupt, thus highlighting the importance of long-term testicular surveillance. Patients should be encouraged to perform frequent testicular self-examinations. Long-term follow-up with a Urologist is prudent for thorough physical examination, measurement of tumor markers, and ultrasound surveillance of the testicles. Based on reports of MTT, we recommend that follow-up should be extended beyond 8 years.
Footnotes
Author contributions
All authors have contributed to the production of this case report.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.