
Abstract
Lymphoma of the urinary bladder is uncommon, and upper urinary tract obstruction due to lymphoma is rare. Herein, we report a case of malignant lymphoma of the bladder with bilateral hydronephrosis in a 67-year-old female who presented with oliguria. Ultrasonography and computed tomography demonstrated a thickened posterior bladder wall and bilateral hydronephrosis. Whole-body positron emission tomography–computed tomography revealed abnormal accumulation in the right iliac internal lymph nodes. Trans-urethral bladder biopsy led to a histopathological diagnosis of non-Hodgkin diffuse large B-cell malignant lymphoma of the bladder. After bilateral nephrostomy, the patient was treated with six cycles of combination chemotherapy including rituximab, cyclophosphamide, daunorubicin, vincristine, and prednisolone (R-CHOP) and two cycles of rituximab alone. Complete remission was maintained during the 3 years of follow-up.
Introduction
Lymphoma of the urinary bladder is rare and can occur in a primary, advanced, or secondary form. Although primary bladder lymphoma occurs in 0.2% of all bladder neoplasms and generally exhibits a silent course with good prognosis, advanced or secondary bladder lymphoma occurs in 1.8% of secondary tumors of the bladder with a poorer prognosis than that for primary bladder lymphoma. 1 The most common subtypes of primary bladder lymphoma are mucosa-associated lymphoid tissue (MALT) lymphoma and diffuse large B-cell lymphoma (DLBCL), and T-cell lymphoma involving the genitourinary tract is extremely rare.2–5 Upper urinary tract obstruction due to lymphoma is also rare. Here, we report a case of advanced, DLBCL of the bladder with bilateral hydronephrosis.
Case report
A 67-year-old female visited our hospital after having oliguria for 1 week without other symptoms. She had no history of tobacco use or other toxic exposures. She had hypertension and well-controlled diabetes. No fever or lymphadenopathy was found on physical examination. Routine hematological and biochemical tests revealed anemia (hemoglobin 10.1 g/dL), a high level of serum lactate dehydrogenase (307 U/L), and renal dysfunction (blood urea nitrogen 71.1 mg/dL and creatinine 9.8 mg/dL). Ultrasonography and computed tomography (CT) demonstrated an irregular thickening of the posterior wall of the bladder and bilateral hydronephrosis (Figure 1(a) and (b)). Growth of a non-papillary tumor in the posterior wall of the bladder was noted on cystoscopy. After percutaneous nephrostomy placement, transurethral biopsy of the bladder tumor was performed for histopathological diagnosis. The hematoxylin- and eosin-stained biopsy specimen presented diffuse heterotypic lymphocytes with irregularly shaped nuclei. The tumor cells were positive for the B-cell markers CD20 and LCA on immunohistochemistry (Figure 2). Additional immunohistochemical stains showed that the tumor cells were positive for CD10 and BCL6, but negative for MUM1. Based on these results, the patient was diagnosed with DLBCL of the bladder and classified as germinal center B-cell (GCB) subtype according to Hans algolism. 6 For further investigation, 18F-fluorodeoxyglucose-positron emission tomography (FDG-PET/CT) was performed, revealing abnormal accumulation in the right iliac internal lymph nodes (Figure 1(c)). No leukemia or lymphoma was found on bone marrow biopsy. These findings indicated that the patient had stage IV (Ann Arbor classification) advanced bladder lymphoma.
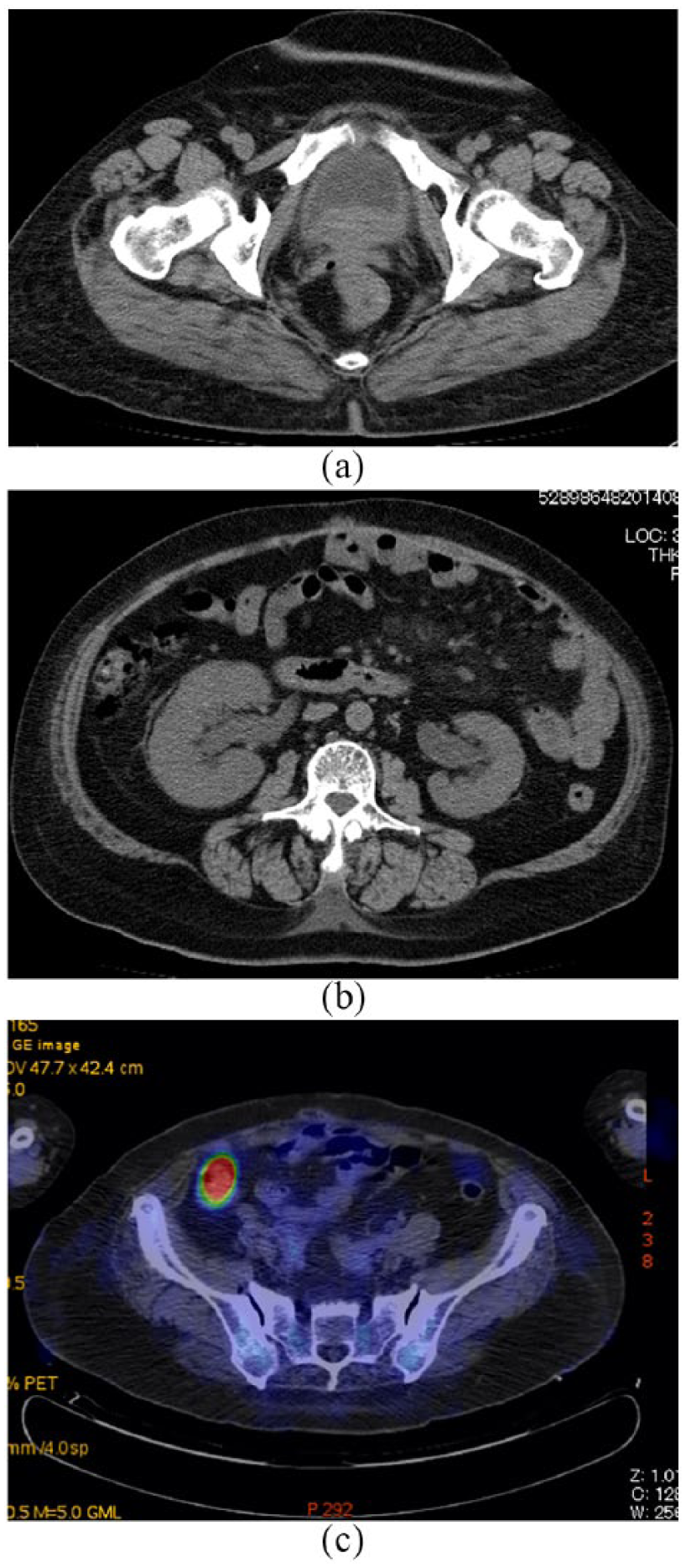
Computed tomography (CT) demonstrates irregular thickening of the posterior wall of the (a) bladder and (b) bilateral hydronephrosis. (c) FDG-PET/CT reveals abnormal accumulation in the right iliac internal lymph nodes.

Histopathological findings: (a) medium (magnification 100×) and (b) high power (magnification 400×) images of hematoxylin and eosin staining show infiltration of the bladder wall by diffuse heteromorphic lymphocytes with irregularly shaped nuclei. Tumor cells are positive for the B-cell markers (c) CD20 and (d) LCA (magnification 100×).
After the patient returned to the normal renal function, the patient underwent six 5-day cycles of R-CHOP (rituximab 350 mg/m2, cyclophosphamide-750 mg/m2, doxorubicin 50 mg/m2, vincristine 1.4 mg/m2, and prednisone 70 mg/day) every 3 weeks, followed by two cycles of rituximab alone. The lesions in the bladder, right internal lymph nodes, and bilateral hydronephrosis had completely regressed without nephrostomy stents at the end of treatment. Subsequent follow-up evaluation, including cystoscopy and CT of the abdomen and pelvis, was performed at 3-month intervals for 3 years. Recurrence was not noted on any of these follow-up examinations.
Discussion
Bladder lymphomas are divided into three clinical groups: primary bladder lymphoma in which patients have disease localized to the bladder, advanced bladder lymphoma in which the bladder was involved as the first site of more advanced lymphoma, and secondary bladder lymphoma in which patients had a history of malignant lymphoma before the development of bladder involvement. 3 Primary bladder lymphomas are rare, but advanced or secondary bladder lymphomas have been reported in 10%–20% of patients with systemic disease. 4 Kempton et al. 5 reported that in a series of 36 cases, 17% of bladder lymphomas were primary lymphoma, 47% were in a non-localized form, and 36% were secondary lymphoma in a series of 36 cases. The most common subtypes of bladder lymphoma are MALT lymphoma and DLBCL.4,5 Low-grade MALT lymphomas are more common in primary bladder lymphoma than high-grade DLBCL are in advanced or secondary bladder lymphoma. In previous reports, bladder lymphoma patients presented with visible hematuria, dysuria, urinary frequency, nocturia, and abdominal pain or back pain. 7 Our patient presented with oliguria due to post-renal failure caused by bilateral ureteral obstruction, which is uncommon for bladder lymphoma. Patients with advanced bladder lymphoma have a higher frequency of ureteral obstruction than patients with primary bladder lymphoma. 5 Six cases, including our case, of advanced bladder lymphoma associated with bilateral hydronephrosis have been reported; however, the main symptom of oliguria in our case was not observed in other seven cases.8–12
A definitive diagnosis of primary or advanced bladder lymphoma requires tissue biopsy and subsequent immunohistochemistry, in which CD20 is positive and cytokeratin is negative, because the clinical and radiological features of this tumor are similar to those of urothelial carcinomas of the bladder. The diagnosis of secondary bladder lymphoma was not difficult based on the clinical history and immunohistochemical staining for CD20. Immunohistochemical and radiographic examinations in the present case confirmed an advanced DLBCL.
Although the optimal treatment for primary bladder lymphoma remains unknown because of the rarity of the disease, the systemic nature of advanced or secondary bladder lymphoma warrants a systemic approach to treatment. Diseases with aggressive phenotypes, like DLBCL, are best managed with chemotherapy using R-CHOP regimes. The present case was successfully treated with R-CHOP chemotherapy.
Conclusion
We reported a case of advanced DLBCL of the bladder with bilateral hydronephrosis that was successfully treated by chemotherapy.
Footnotes
Authors’ contribution
YK wrote the first draft of the manuscript. All authors reviewed and edited the manuscript, and approved the final version of the manuscript.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The Kurume University Ethical Committee approved this case report.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.