
Abstract
Hamartoma of lung is a common tumor, majority of which are small and incidentally discovered during plain chest radiography. Our case is a 30-year-old gentleman with an extremely uncommon presentation of a common tumor, that is, a giant hamartoma of lung presenting as massive hemoptysis and intractable cough. To the best of our knowledge, such occurrence of giant pulmonary hamartoma is very uncommon and its presentation with massive hemoptysis is even more uncommon. Less than 20 cases of giant hamartoma of lung have been reported in the English literature so far.
Keywords
Introduction
Pulmonary hamartoma is a benign mesenchymal neoplasm, which is composed of a mixture of all of the normal components of lung with disorganized pattern of distribution. 1 Hamartoma in lung can be parenchymal or endobronchial with an incidence of about 0.025%–0.32%. 2 This tumor is the most common benign tumor in lung, and it is mostly small with a size of less than 2 cm, most commonly asymptomatic and incidentally found tumor. 2 Pulmonary hamartoma with large size is rare, and to the best of our knowledge, less than 20 cases of giant hamartoma have been reported in the English literature so far.
Herein, we report our experience with a huge hamartoma in lung presented with massive hemoptysis and intractable cough.
Case report
A 30-year-old man presented with acute cough and massive hemoptysis. Physical examination showed decreased breathing sound in right hemithorax. Laboratory tests showed microcytic hypochromatic anemia (Hb = 9.9 g/dL); otherwise, all other chemical and hematologic tests were normal.
Emergency computed tomography (CT) scan has been performed, which showed a huge mass in the hilum of right lung with extension to middle and superior lobe and adhesion to right pulmonary artery. The mass showed multiple areas of amorphous calcification associated with pressure effect on lower and middle bronchus (Figure 1).
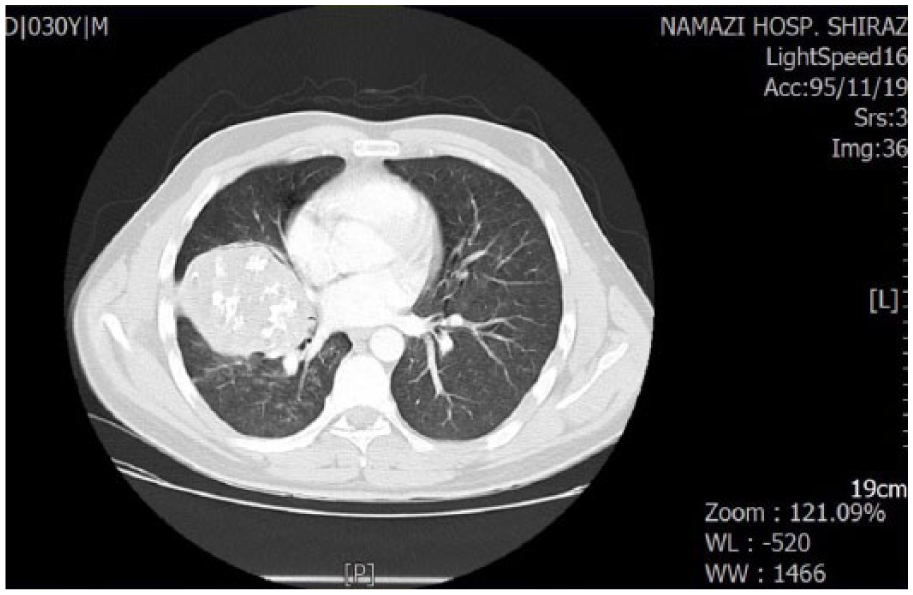
CT scan of the lung shows a huge intrapulmonary mass with calcification.
The patient underwent surgery to excise the mass, because no conservative therapy could stop the hemoptysis and cough.
During operation, the mass was found in the major fissure and hilum of right lung with adhesion to right pulmonary artery and superior pulmonary vein. Right posterolateral thoracotomy, pneumolysis, and right pneumonectomy were performed. Adhesion to vessels was successfully released. There has also been mediastinal lymphadenopathy, so lymph node dissection was also performed.
The surgical specimen received in the pathology department showed a mass with creamy-white color and gritty consistency, measuring 10 cm in diameter with pressure effect on the main bronchus (Figure 2).

Gross of the pneumonectomy specimen shows a round white and cartilaginous tissue.
Sections from the tumor showed mostly benign cartilage, fibroblastic matrix, foci of ossification, as well as small cystic spaces lined by respiratory epithelium. No atypia or mitosis was present (Figure 3(a) and (b)).

Microscopic sections of intrapulmonary mass showing mostly cartilage, fibroblastic background, and bronchial epithelial lining (H&E, ×100): a) Sections from intra-pulmonary mass show bronchial epithelial cells in the right corner and mature cartilage in the left corner; b) Sections from intra-pulmonary mass show bronchial epithelial cells in the right and mature cartilage in the left.
After surgery, the patient had an uneventful postoperative period. Hemoptysis and cough were stopped and the patient discharged in good condition. Now after 1 year, he is well and free of any complications.
Discussion
Hamartoma is the most common benign tumor of the lung. It is composed of a mixture of normal components of lung, that is, bronchial epithelium, cartilage, and mesenchymal connective and fibroblastic tissue. 1 This tumor is commonly presented as an incidental coin-like lesion in the plain chest X-ray with a size of less than 2 cm. 2 It means that majority of pulmonary hamartomas are asymptomatic small masses in the lung parenchyma. 3 There are very rare case reports of hamartomas in the lung with a size more than 8 cm. Majority of the hamartomas originate from periphery of lung within the parenchyma, therefore even these huge and giant hamartomas are most commonly asymptomatic.4,5 Very rarely, a hamartoma in lung can be presented with symptoms such as hemoptysis, cough, or chest pain. Those presenting with the above-mentioned symptoms are either endobronchial or are so huge that have pressure effect on adjacent parenchyma of lung, bronchus, or major vessels. The occurrence of these problems in pulmonary hamartoma is extremely rare and very uncommonly reported in the English literature. Table 1 shows the details of the characteristics in the 18 reported giant hamartomas (>8 cm) since 15 years ago.1–14,19 The best method of preoperative diagnosis is CT scan, and the final diagnosis is based on histopathologic findings. 11 The presence of calcification in a well-defined pulmonary mass without invasion is highly in favor of pulmonary hamartoma, as this tumor is the most common benign tumor of the lung. 6
The details of the 17 previously reported cases of hamartomas in the lung with the size of more than 8 cm.

NR: not reported.
Simple excision is the method of choice for the treatment of hamartomas; however, for very large giant tumors, especially when located around the hilum, pneumonectomy is the only choice. 12 There are also case reports of laser-assisted ablation of tumor. 5 With the various treatments, all of the cases of giant hamartoma of lung have been reported to have a very good prognosis with uneventful postoperative period. No recurrence has been reported.
Our patient is a 30-year-old man presented with massive hemoptysis and intractable cough because of pressure effect on the main bronchus and pulmonary vessels, discovered to have a large 10 cm pulmonary hamartoma. All of these findings are very rare in a benign tumor in lung.
Footnotes
Acknowledgements
All authors contributed equally to the manuscript.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the Ethical Committee of Shiraz University of Medical Sciences.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written and verbal informed consent for patient information and images to be published was provided by the patient.