
Abstract
Background
Juvenile idiopathic arthritis (JIA) is one of the most common childhood-onset rheumatic diseases in Asia. Given the chronic nature of JIA and the need to minimise long-term damage, polypharmacy is often required to quickly achieve and maintain remission. Furthermore, non-adherence to treatment can delay disease resolution and lead to poor outcomes. Reported reasons for non-adherence include inadequate understanding of the disease course and experiencing adverse effects of treatment, which may be addressed by an educational intervention.
Objectives
We aim to describe the development, implementation, and evaluation of a clinical pharmacist-led education program for JIA patients.
Methods
Newly diagnosed JIA patients and their caregivers with newly prescribed medications were enrolled into the pharmacist-led educational program. This was conducted using standardized education materials. Primary outcome was caregivers’ JIA knowledge pre and post counselling. Other outcomes were caregivers’ satisfaction, time spent and cost savings by patients.
Results
Fourteen responses were collected. Caregivers’ JIA knowledge score improved significantly from a median score of 5 (range 3-10) pre-counselling to 10 (range 6-10) post-counselling (p = 0.006). The service was well-received by caregivers (median satisfaction score of 32 (range 20-35)). Manpower costs for training and for the pharmacist to provide the service was 0.5 full-time employee. Each patient who underwent the pharmacist-led counselling potentially saved S$54-92. The pharmacist also contributed to education and research on rheumatology topics.
Conclusion
Pharmacist counselling improved caregivers’ JIA knowledge and potentially saved costs for JIA patients. Pediatric rheumatology centres should consider the inclusion of a clinical pharmacist in their team.
Introduction
Juvenile idiopathic arthritis (JIA) is a heterogenous group of inflammatory joint diseases of unknown cause that has onset before 16 years of age. 1 Worldwide, JIA affects approximately two million children aged below 16 years, with Asia having the highest estimated numbers of JIA. 2 A previous study conducted in Asia reported JIA as the most common condition seen in pediatric rheumatology clinics in Israel and India. 3 Within Southeast Asia, JIA was the most common disease in pediatric rheumatology centres in Thailand and Malaysia then followed by the Philippines and Singapore. 4
Untreated JIA may lead to complications like permanent joint damage, the persistence of disease into adult years and be associated with lowered health-related quality of life. Hence, treatment of JIA with polypharmacy is often required to quickly achieve and maintain disease remission. 1 Non-adherence to treatment negatively impacts prognosis, delays resolution of the disease and increases the rate of complications in JIA.5,6 However, approximately 38% of JIA patients were reported to be non-adherent to medications in a Thai cohort of pediatric rheumatology patients. 7 Possible explanations for non-adherence included fear about the side effects of prescribed medications and misunderstanding the importance of treatment and progression of the condition.5–8 Furthermore, Teh et al. reported that despite 79% of JIA patients achieving clinically inactive disease within 2 years, only 25% successfully weaned off all medications for a minimum of 1 year. 9 Thus, given the prolonged treatment course, there is a need to ensure treatment adherence. This can be done by empowering patients and caregivers with the essential information regarding JIA and its management.
Clinical pharmacists have been making a significant impact in the care of patients with chronic diseases. Specific to pediatrics with chronic diseases, clinical pharmacists’ educational interventions have been shown to improve pediatric patients’ asthma control, 10 as well as patients’ and caregivers’ knowledge on epilepsy 11 and atopic dermatitis. 12 However, to date, no studies have evaluated the role of clinical pharmacists in pediatric rheumatology care.
In rheumatology conditions, many patients require chronic polypharmacy 1 or frequent medication changes. As such, the clinical pharmacist is well-positioned to take up the task for medication-related education and follow up. In contrast, the rheumatology nurse helps to manage and redirect medical enquiries to the rheumatologists or medication-related enquiries to the clinical pharmacist, manage appointments or blood tests for patients, and update patients on blood test results. This teamwork allows for effective patient management while optimizing each healthcare provider’s role in the multidisciplinary team.
Aim
Therefore, we aim to describe our experience with a clinical pharmacist in the multidisciplinary pediatric rheumatology ambulatory clinic, as well as the implementation of a novel clinical pharmacist-led educational counselling for all newly diagnosed JIA patients and their families in our institution.
Ethics approval
This study was exempted from review by the institutional review board as an educational intervention.
Methods
Setting
The pediatric rheumatology ambulatory clinic in our pediatric tertiary centre sees about 110 patients weekly. The clinical pharmacist attends the outpatient clinic for one full day and offers specialized counselling services for patients and caregivers on this day. The pharmacist also offers counselling on an additional half day per week. This works out to 0.3 full-time equivalent (FTE). One FTE is 42 working hours per week in the local context. Each full counselling session lasts approximately 1 hour and while a drug-only counselling session lasts about 30 to 40 minutes.
Training of the clinical pharmacist
Training for the clinical pharmacist included self-reading of relevant treatment guidelines and clinical studies, which was done partly during or after office hours. This was followed by guided, planned discussions with the trained rheumatology pharmacist. Subsequently, on-the-job training was commenced with once weekly in-clinic attachment with the rheumatologists. After approximately 3 months of clinic attachment, the pharmacist was assessed for independently conducting the full counselling, which takes about 1 hour. The total training duration lasted approximately five to 6 months before the pharmacist was able to sit in the clinic and perform full counselling independently. A total of 0.2 FTE was required for this standard training period, with extensions allowed as deemed necessary.
Materials
Standardized contents for the full counselling session covered information about the pathophysiology of JIA, diagnosis, JIA subtypes, complications, prognosis, pharmacological and non-pharmacological management of JIA in layman’s terms. This was adapted from the information in English and Mandarin provided by Pediatric Rheumatology International Trials Organisation (PRINTO),13,14 with updated information from research from Southeast Asia.3,4 Additionally, we included medication monographs compiled by the pharmacists which also included management of common minor adverse effects, and when to seek medical advice for rarer but potentially dangerous adverse effects. The contents of both languages were reviewed and edited by the rheumatology team before publication. This material was given to patients and their families at the end of the counselling in the form of a booklet in Mandarin or English. If required, the pharmacist will give a complimentary follow-up phone call to caregivers about 2 weeks after new medications are started, or to follow up on adherence and safety concerns of the medications. Telephone follow-up may be requested by the rheumatologists, nurses or parents. The pharmacist also followed up with non-adherent patients, patients who had newly started medications and parents who may have had further questions after the initial counselling sessions.
Two sets of self-administered questionnaires (Supplement File) were used to evaluate the knowledge of caregivers after attending the full counselling. The questionnaire set A was assembled and reviewed by the rheumatologists, specialty nurses and the pharmacist. This knowledge questionnaire consisted of information discussed in the content of counselling and common misunderstandings on the condition based on questions frequently asked by caregivers. Responses were “True”, “False” or “Not sure”. Questionnaire Set B had the same questions as Set A, but with a different sequence to assess post-counselling knowledge. Correct responses scored one point, incorrect responses scored −1 point, while “not sure” responses scored zero points. These scores were then summed to give a final score; hence possible score range was −10 to 10 for both sets. Set B also included a short survey on patient satisfaction with the service, adapted from previously published studies evaluating pharmacist-led services,11,12 with scores ranging from five to 35. Both sets also contained a last question, “How confident are you to manage your child’s condition?” to assess the caregiver’s confidence in managing the condition. The questionnaires were written in layman’s terms and were piloted in five caregivers and patients, which were not used in the final analysis. Minor editing was performed before administering the questionnaire to the rest of the caregivers and patients.
Flow of the study
This was a single-arm pre-post educational intervention study. After the pediatric rheumatologist’s assessment, all newly diagnosed JIA patients with their caregivers were referred to a separate consult room to undergo full counselling conducted in English or Mandarin. Caregivers finished the self-administered Set A. After completing this questionnaire, the pharmacist proceeded with the session. Caregivers and patients were allowed to clarify any doubts during this session. After the counselling session, caregivers and patients completed Set B (Figure 1). The clinical pharmacist did not review the pre-counselling questionnaires before the educational intervention to prevent any bias. The pharmacist will review the post-counselling questionnaire after the counselling and reinforce important information to caregivers before letting them leave the clinic. No identifiable patient information was collected. Workflow for the study.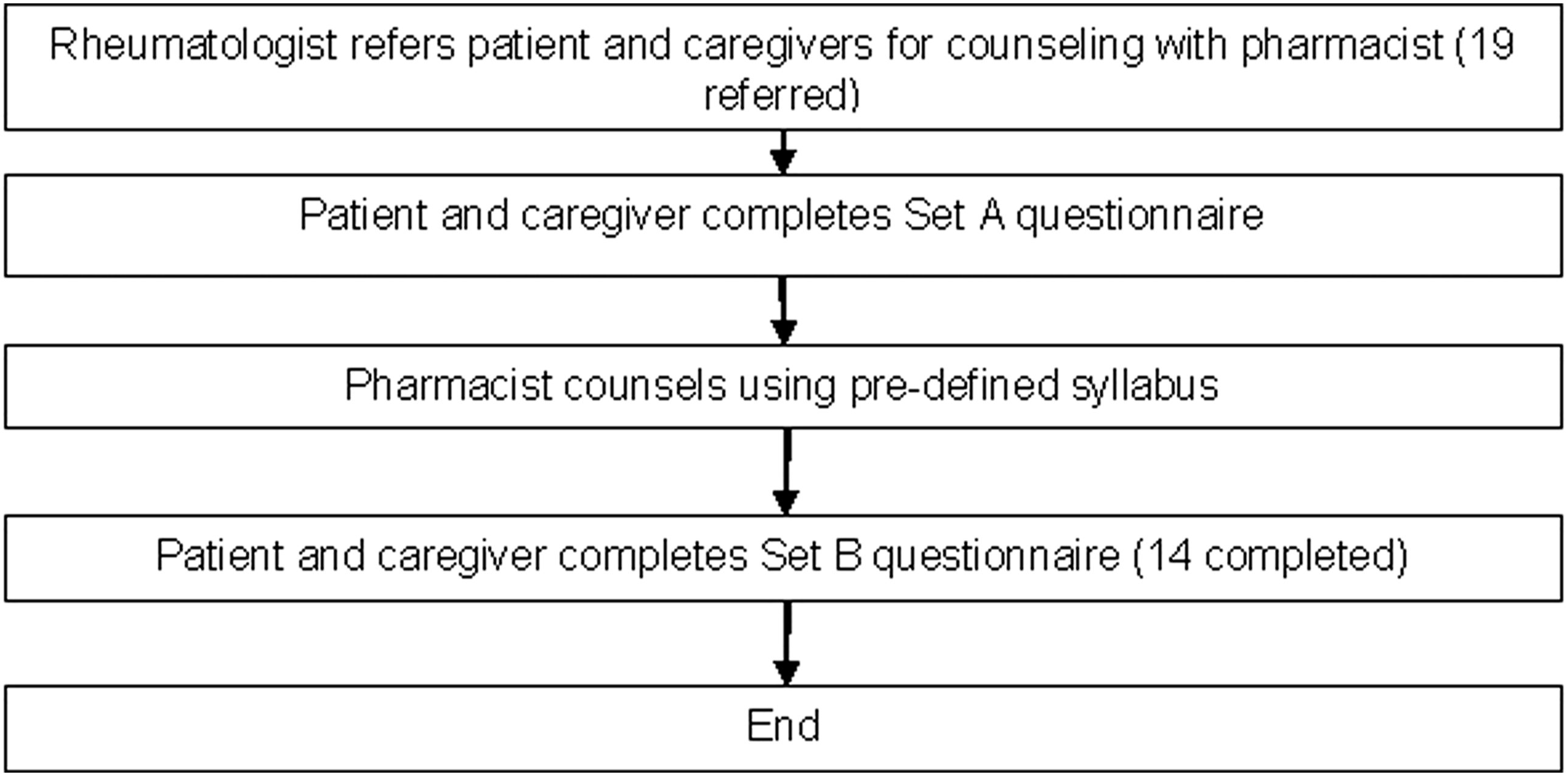
Inclusion and exclusion criteria
All newly diagnosed JIA patients’ main caregivers with newly prescribed medications who underwent full sessions were included. They must be literate in English or Mandarin. Caregivers who declined participation were excluded from the study but still underwent counselling.
Measurements and statistics
The primary outcome was the change in caregivers’ knowledge in JIA post-pharmacist counselling. Secondary outcomes were the satisfaction of caregivers, time spent on the service, and cost savings to patients. For the primary outcome, pre- and post-counselling knowledge scores were non-parametric and compared using Wilcoxon signed-rank test, and α < 0.05 was considered statistically significant. For the secondary outcomes, caregiver satisfaction score and the time taken for each session were recorded. Median scores and range were recorded for all scores. Moreover, total time spent by the pharmacist for the service was noted. Cost savings by the patients were also noted. Calculations were done with Excel (Microsoft Corporation 2024).
Cost savings estimation
Patient cost savings were estimated by comparing current practice, where patients requiring additional education receive extended rheumatologist consultations (costing 50-100% more than standard 10-15 min non-subsidized appointments), with pharmacist-led counselling sessions. Cost savings equalled the difference between extended rheumatologist consultation fees and pharmacist counselling fees, assuming pharmacist counselling could effectively replace additional rheumatologist’s time for patient education.
Results
Knowledge and patient satisfaction
Summary of results for specialized pharmacist counselling for juvenile idiopathic arthrithis (JIA), N = 14.

*statistically significant (p = 0.006).
Caregivers with correct responses for the individual knowledge questions.

Note. The above table only shows the number of correct responses. In the manuscript, each correct response scored one-point, incorrect response scored −1 point. “Not sure” scored zero points. The sum of the scores was used for analysis.
Median overall satisfaction score was 32 (range 20-35). The two top-rated aspects were “2. How well does the pharmacist explain how your child’s medication works” and “5. How useful was the information presented by the pharmacist”, which both had a median score of 5 (range 3-5). The lowest rated was “6. How will you rate your knowledge on JIA after the counselling” with a median score of 4 (range 3-5).
Total time spent by the pharmacist on the service
Breakdown of all counselling done by the clinical pharmacist.

Abbreviations. JIA: Juvenile idiopathic arthritis, cSLE: Childhood systemic lupus erythematosus, CNO: Chronic non-bacterial osteomyelitis, UCTD: Undifferentiated connective tissue disease, MTX: Methotrexate, SSZ: Sulfasalazine, HcQ: Hydroxychloroquine, CPM: Cyclophosphamide, AZA: Azathioprine, MMF: Mycophenoloate mofetil, ACEi: Angiotensin converting enzyme inhibitor.
Cost savings for patients for the service
The average rheumatologist’s cost for a usual follow-up non-subsidized consultation is S$147 for a 10 to 15-min consultation slot. If the consultation time is extended, then the patients will incur additional costs of 50 to 100% of the consultation cost, i.e. S$73 to 147 (USD55-110). The pharmacist counselling service was complimentary during the start-up phase. Subsequently, patients were charged S$55 (USD41) for full JIA counselling and S$19 (USD14) for drug-only counselling. There were no additional charges if telephone follow-up by the pharmacist was deemed necessary. For full counselling on JIA, assuming a 100% additional charge for the rheumatologist’s consultation was added, then each pharmacist’s full counselling session would have saved the patient S$92 (USD69). For drug-only counselling, assuming a 50% additional charge for the rheumatologist’s consultation, then each pharmacist’s session would have saved the patient S$54 (USD41).
Other contributions by the clinical pharmacist
From September 2019 through to October 2024, the pharmacist performed 797 interventions or enquiries. This was provided to the multidisciplinary healthcare team, patients, families, and medical students. These interventions include enquiries over email, texts and calls and include both inpatients and ambulatory patients. Most of the interventions were drug information (382, 47.9%), followed by dosing (219, 27.5%). Drug information included costs, drug identity, pharmacology, pharmacokinetics, administration, drug availability, and formulation. Others included: medication history, safety and adverse effects of medications, drug interactions, omissions and duplicate drug therapy. A full breakdown of interventions is shown in Figure 2. Breakdown of interventions by the pharmacist (%).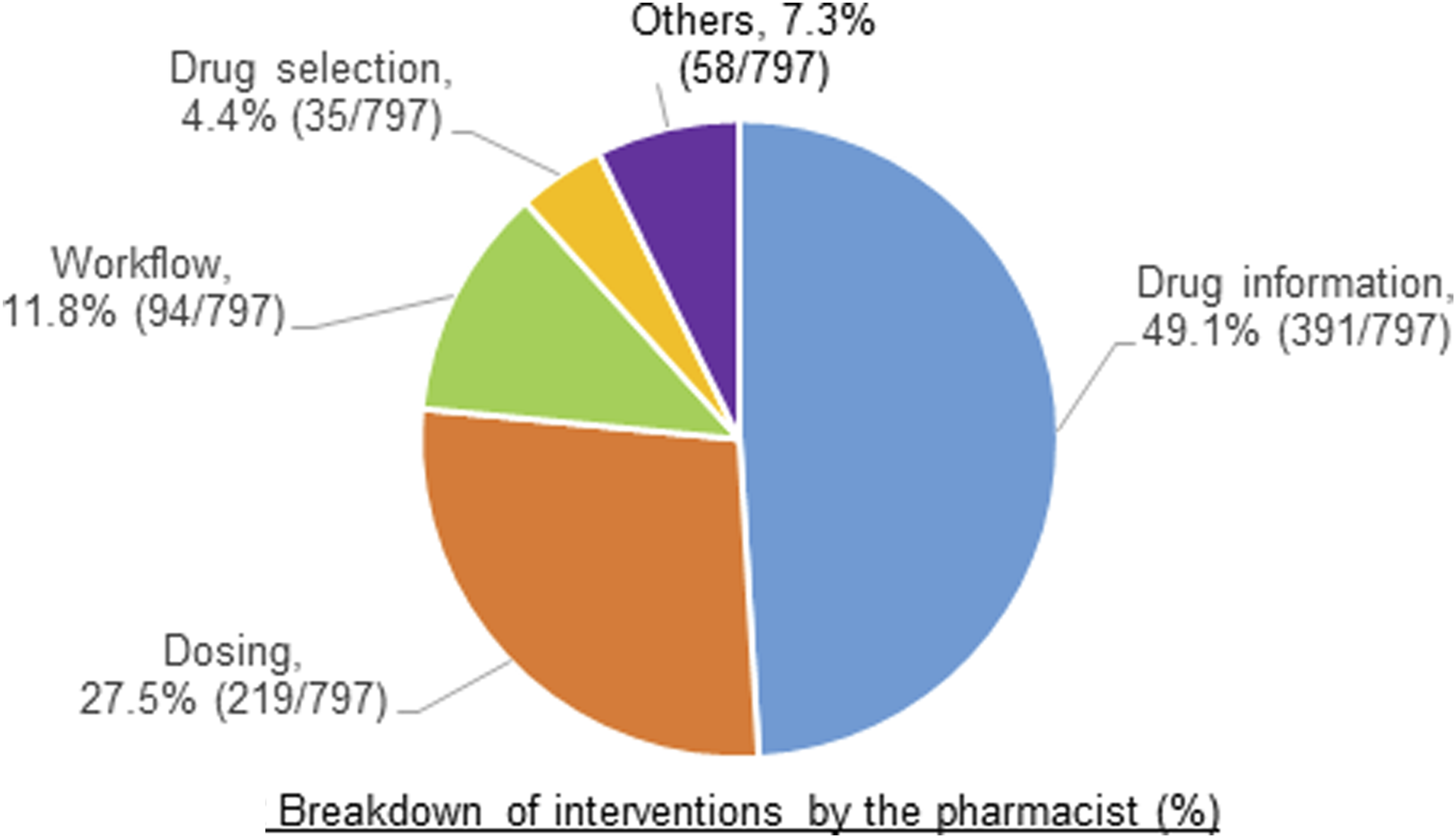
The pharmacist also conducted two education sessions for the multidisciplinary team and one session for the hospital nurses. Furthermore, in terms of research, the pharmacist led and completed two studies with the rheumatology team. As a result of these, two abstracts15,16 were presented at international rheumatology conferences. In addition, the pharmacist helped to include three drugs in the hospital formulary, improving the ease of patient access to these drugs.
Discussion
Treatment adherence is of utmost importance to achieve and maintain remission in JIA.5,6 A previous systematic review reported that education interventions had the most evidence to enhance medication adherence among adult rheumatology patients, including those with rheumatoid arthritis, and SLE. 17 In that review, the educational program for patients and caregivers, including those led by pharmacists, resulted in significant improvement in treatment adherence.
Specific to JIA patients, Kirchner et al. identified that medication side effect was a top reason for non-adherence in a cohort of JIA patients. 8 Moreover, in another JIA cohort, issues with medications, such as unawareness of the importance of medications, side effects and difficulty in taking medications, were the top reported reasons for medication non-compliance. 7 Side effects of medications were also reported as one of the main barriers to treatment adherence in a multicentre study in the United States for JIA patients. 5 Len et al. also reported that the fear of adverse reactions of treatment, and knowledge gap in JIA disease mechanisms may negatively affect treatment adherence. 6 These studies highlighted why patient education is of utmost importance and why our materials emphasized disease explanation and medications with specific common side effects and corresponding management tips. This also stresses how clinical pharmacists are in a unique position to educate patients and caregivers to self-manage common self-limited medication side effects and when to seek medical advice for more concerning side effects. To improve patients’ accessibility to clinical pharmacy services, the clinical pharmacist also provided a direct contact number for patients and caregivers to ask medication-related questions via calls or text. It was interesting to note that despite improvement in caregivers’ knowledge, the change in caregivers’ confidence to manage JIA was not statistically significant. However, it was suggestive of a trend towards improved caregiver confidence post-counselling. If more caregivers were recruited, perhaps the improvement in confidence could be demonstrated.
In pediatric healthcare, parents are primarily the decision-makers. Previous studies have reported that low parental health literacy could have a negative impact on pediatric health. Health literacy in turn, can be influenced by cultural differences, societal norms and literacy itself. 18 In our study, most (10/14) of the surveyed caregivers were Chinese, and most (9/14) had tertiary education. However, due to the limited number of participants, we could not describe the influence of culture and education on the knowledge scores. This is important in the local multicultural context. This should be investigated in future studies to include more participants of various races and education levels.
Through the counselling, we also identified the most common misconceptions that caregivers have about JIA with regards to eye-screening, if there was a need to take medications lifelong, and the difference between adult-onset arthritis and JIA. First, although JIA-associated uveitis was rare in Asians (2.8%) compared with European (9.0-19.1%) and North American cohorts (11.3%), 19 the onset is insidious and potentially dangerous; hence, we still advise all JIA patients to undergo routine eye screening. Second, the caregivers in our study appear to lack knowledge of the duration of medications for JIA. Withdrawing medications in JIA patients with clinically inactive disease will help to reduce cost and reduce side effects of treatment, 20 hence we will encourage caregivers to initiate this discussion when the child is in remission. Third, JIA patients are unique from adult rheumatoid arthritis patients, even when JIA patients transition to adult care. This was evident from the higher proportion of biologic use in the adult JIA groups versus the non-JIA patients.21,22 Adult JIA patients also had lower disease activity and higher remission rates versus adult non-JIA patients. 21 Hence, it was important to highlight the differences in prognosis and management in JIA versus adult non-JIA patients to caregivers. These findings have been incorporated into subsequent counselling sessions.
There were potential cost savings for patients from the pharmacist-led counselling. Each session with the pharmacist resulted in median cost savings of S$54-92 from potential long consultation charges with the rheumatologists. This was consistent with a systematic review, where pharmacist-led services like adherence interventions, medication review, and services focusing on warfarin and type 2 diabetes management are cost-effective. 23
Manpower costs for training the clinical pharmacist required 0.2 FTE, and subsequently, the service required 0.3 FTE. This allows existing manpower to be utilized before requesting additional headcount if there is a need to expand the pharmacists’ services. Hence, this should be feasible to implement using existing headcounts. The service was sustained with permanent rostering of the clinical pharmacist to manage the service. Potential barrier to scalability includes stress to increase costs for pharmacists’ services amidst rising healthcare costs and the availability of trained clinical pharmacists.
Limitations
As this was a single-arm study with no comparator, possible confounders like caregiver motivation, prior knowledge from other sources may have influenced the results. More motivated caregivers may have opted into the counselling and influenced the results. Furthermore, although we showed improvement in caregivers’ JIA knowledge post-counselling, the effect on clinical outcomes and adherence was not documented in this educational intervention study. However, in a systematic review that included pediatric studies, pharmacist-led education improved knowledge and consequently treatment adherence. 24 Therefore, we believe that by empowering caregivers with JIA knowledge, they could better co-manage this chronic condition with improved treatment adherence. Furthermore, we piloted the JIA knowledge questionnaire, which was pre-tested but was not formally validated. The sample size appeared small due to reduced physical appointments during the COVID period from 2020-2021, which limits the generalizability of the results. However, we believe that the positive effect of the pharmacist’s counselling on caregivers’ knowledge will be similar. Also, cost savings are hypothetical and not formally measured with an actual cost-effectiveness analysis.
Possible limitations and benefits from the perspective of the clinical pharmacist
Benefits from the clinical pharmacist’s perspective include having to hear from the patients and their families about their concerns about treatment directly from them, which they might be afraid to highlight to the rheumatologists or nurses. This helps the clinical pharmacists to improve communication with the patient and family and aids in rapport building to improve treatment adherence. Furthermore, having this service helps to elevate the position of pharmacists in another subspecialty in pediatric care. A possible limitation is that the time spent in the clinic is too short to cover all rheumatologists’ appointments, which affects the uptake of the pharmacist’s services.
Future plans and research
The clinical pharmacist currently spends about 0.3 FTE in the ambulatory clinic and has already expanded the counselling to other rheumatology conditions. Other than outpatient enquiries, the pharmacist also received enquiries about inpatients admitted for rheumatology conditions. In the future, the FTE should be increased to at least 0.5 FTE to allow the pharmacist to offer counselling service to more patients on more days of the week. Furthermore, the increased FTE will allow the pharmacist to routinely join the rheumatology team to review inpatients and extend the counselling service to inpatients and their families too. Given the extended time in clinic, the pharmacist will also be able to review treatment safety and adherence before the rheumatologists’ consultations. The clinical pharmacist could also perform interventions to improve patient care and contribute to the education of the rheumatology team.
We recommend that future studies should be planned to include medication adherence and clinical outcomes that result from the clinical pharmacist’s educational interventions. A formal economic evaluation should also be conducted to evaluate the value of a clinical pharmacist in the rheumatology team.
Conclusions
The inclusion of the clinical pharmacist in the pediatric multidisciplinary rheumatology team had a positive impact in many areas. The pharmacist-led education session significantly improved caregivers’ knowledge in the management of JIA and was well-received by caregivers. The service also helped to potentially reduce significant costs to patients from prolonged rheumatologists’ consultations. The pharmacist also provided interventions, education to the medical team and contributed to research. Initial implementation required only 0.3 FTE. Pharmacists should be incorporated into multidisciplinary rheumatology teams in other centres.
Supplemental Material
Supplemental Material - Impact of a clinical pharmacist-led educational intervention on caregiver knowledge in a paediatric ambulatory rheumatology clinic
Supplemental Material for Impact of a clinical pharmacist-led educational intervention on caregiver knowledge in a paediatric ambulatory rheumatology clinic by Chunliang Chen, Kai Liang Teh, Sook Fun Hoh, Xiaocong Gao, Lena Das, Thaschawee Arkachaisri in Proceedings of Singapore Healthcare.
Footnotes
Author note
This study was accepted by EULAR 2024 and published as an abstract in part in Annals of Rheumatic Diseases.
Acknowledgements
We would like to thank pharmacists Ms Kelly Chong and Mr Enoch Loy during their stint in the service. We would also like to thank pharmacists Ms Ng Ai Shing and Mr Hie Szu Liang for helping to work out the manpower hours, and assistance in setting up the pharmacist-led service. We are also thankful for the clinic nurses and administrative staff of specialist outpatient clinic T for the support to the rheumatology team.
Ethical considerations
Ethical approval for this study was waived by SingHealth Centralised Institutional Review Board because it was a service evaluation (2020/2898). This study was completed in accordance with the Helsinki Declaration.
Consent to participate
Informed consent was not sought for the present study because the study was exempted from review.
Authors contributions
CC, TKL and TA researched literature and conceived the study. CC, TKL, HSF, GX, LD, TA were involved in questionnaire & protocol development. CC was involved in gaining ethical approval, patient recruitment and data analysis. CC wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analysed during the current study are available from the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.