
Abstract
Introduction
Primary care professionals (PCPs) acts as first encounters in various medical conditions. The awareness on the importance of early detection as well as management of childhood hearing loss (HL) is crucial as it imposed great impact on speech and language development.
Objectives
This study aimed to determine the knowledge, attitude and practice towards paediatric HL among PCPs.
Methodology
This was a cross sectional study involving PCPs by means of QR codes containing self-reported questionnaires using Google Form.
Results
120 out of 505 PCPs responded with the response rate of 23.8%. Majority of the PCPs showed substantial knowledge on risks factors related to childhood HL. Most of the PCPs believed that Newborn Hearing Screening (NHS) were important (90.8%) but only 12.5% had confidence to render the NHS results. 76.7% of PCPs revealed that they were not properly equipped with childhood HL during their medical training. PCPs showed preponderance towards online continuous medical education (CME) as medium of choice to improve awareness on childhood hearing loss.
Conclusion
Despite showing satisfactory knowledge and attitude towards paediatric HL among PCPs, the clinical practice on this matter is still lacking.
Introduction
Hearing loss (HL) is one of the commonest treatable disabilities among children. It is estimated that 1.1 in 1000 live births were diagnosed to have HL and it is more prevalent in high-risk babies which was reported to be 3 to 4 babies in 1000 live births. 1 Managing HL in children is considered a neurodevelopmental emergency. Children’s brain development is time-critical and thus, the brain needs optimal auditory and language stimulation within this term. Based on this fact, children with HL should receive intervention as early as possible before the neuroplasticity starts to develop. This is to ensure optimal speech and language acquisition on par with children with typical hearing and speech development. 2
In response to the nationwide newborn hearing screening (NHS), primary care professionals (PCPs) are expected to have a sufficient understanding of HL among children because they are the first point of contact for various medical conditions. Although NHS is not performed in primary care setting in this country, PCPs must be fluent in managing children with suspected HL during well-child visits in primary care centres. Prompt referral to Otorhinolaryngologists or audiologists is warranted to establish the hearing level so that early hearing intervention can be instituted. Joint Committee on Infant Hearing (JCIH) advocated the 1-3-6 rule, in which any children with congenital HL should be screened by 1 month old, followed by establishment of diagnosis of HL by 3 months old and receive intervention by 6 months old. 3
Time is a fundamental element in managing congenital HL before neuroplasticity starts to happen as a result of prolonged deprivation of sound stimulation. 4 In Malaysia, it had been reported that the mean age of diagnosis of hearing loss among children who received cochlear implantation was 24.3 months old. 5 Children with HL preferably receive hearing intervention by means of hearing aids or cochlear implants before the age of 2 years old because study has shown that the speech outcome was comparable to children with typical hearing. Whilst, HL children who get hearing intervention after 2 years old demonstrated unsatisfactory speech development when compared with their peers. 4
Delaying the intervention in HL poses a great impact on children’s speech development, academic achievement, and quality of life (QOL). The study by Goh et al found that every delay in cochlear implantation by 1 month, the chances for mainstream education reduced by 3.3%. 6 Similar study also reported that the development of verbal communication plummeted by 2.6% following a 1-month delay in cochlear implantation. Congruence to this fact, children with HL demonstrated lower QOL scores as compared to children with typical hearing. 7
This study aims to explore the knowledge, attitude and practice of childhood HL among PCPs. The findings of this study will contribute to realising the vision of the Ministry of Health Malaysia to ascertain HL in children as early as at birth.
Methodology
This was a cross-sectional survey among PCPs including family medicine specialists and medical officers in public primary care clinics in Johor state by means of convenience sampling. This study was conducted from October 2021 till April 2022. A total of 505 QR codes containing the online questionnaires using Google Form were posted to all primary care clinics in Johor state and the respondents were required to answer all questions. Only respondents who were fluent in English were invited to participate in this study. Upon consenting to participate in this study, the respondents were asked to click the “Agree’ button.
The questionnaires were adapted from previous literature. 8 The questionnaires were divided into 4 domains. The first domain enquired into respondents’ sociodemographic including gender, position, duration of practice in primary care settings, provenance and number of paediatric cases encountered in clinical practice for the past 1 year.
The second domain explored the knowledge of PCPs regarding risk factors of permanent childhood HL. Five items indicated correct responses which are meningitis, history of cytomegalovirus, congenital syphilis, family history of hearing loss and more than 48 hours in the neonatal intensive care unit. Whilst, the other 5 items were incorrect responses included congenital heart disease, hypotonia, mother greater than 40 years old, cleft palate and frequent colds.
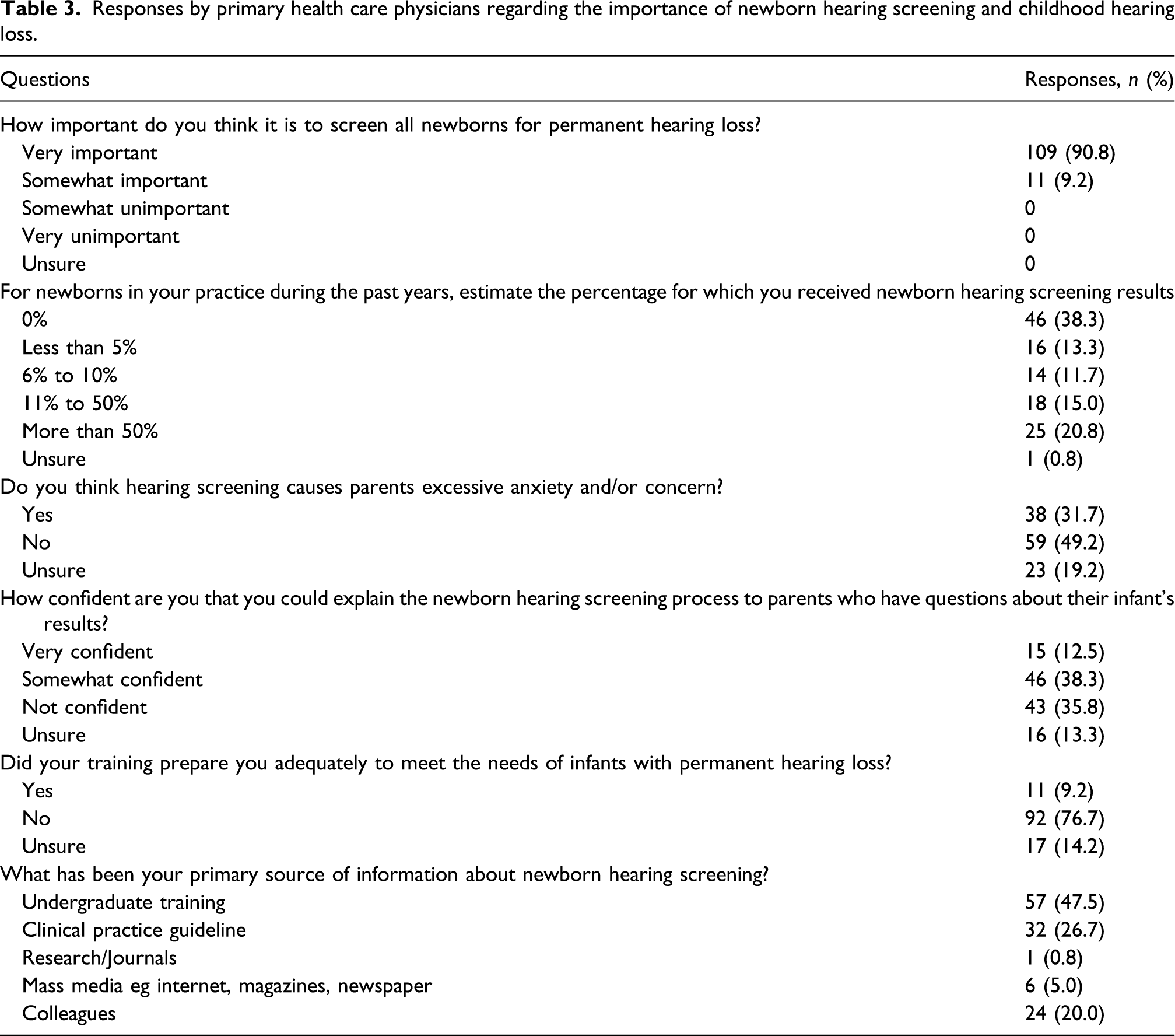
The third domain further scrutinised the understanding towards NHS and childhood hearing loss among PCPs. The items comprised of 6 questions on the importance of NHS, the percentage of NHS results received by PCPs during their practice, parents anxiety towards NHS, the PCP’s confidence in explaining the NHS results to the parents, adequacy of medical training with regards to paediatric hearing loss and primary source of information about NHS.
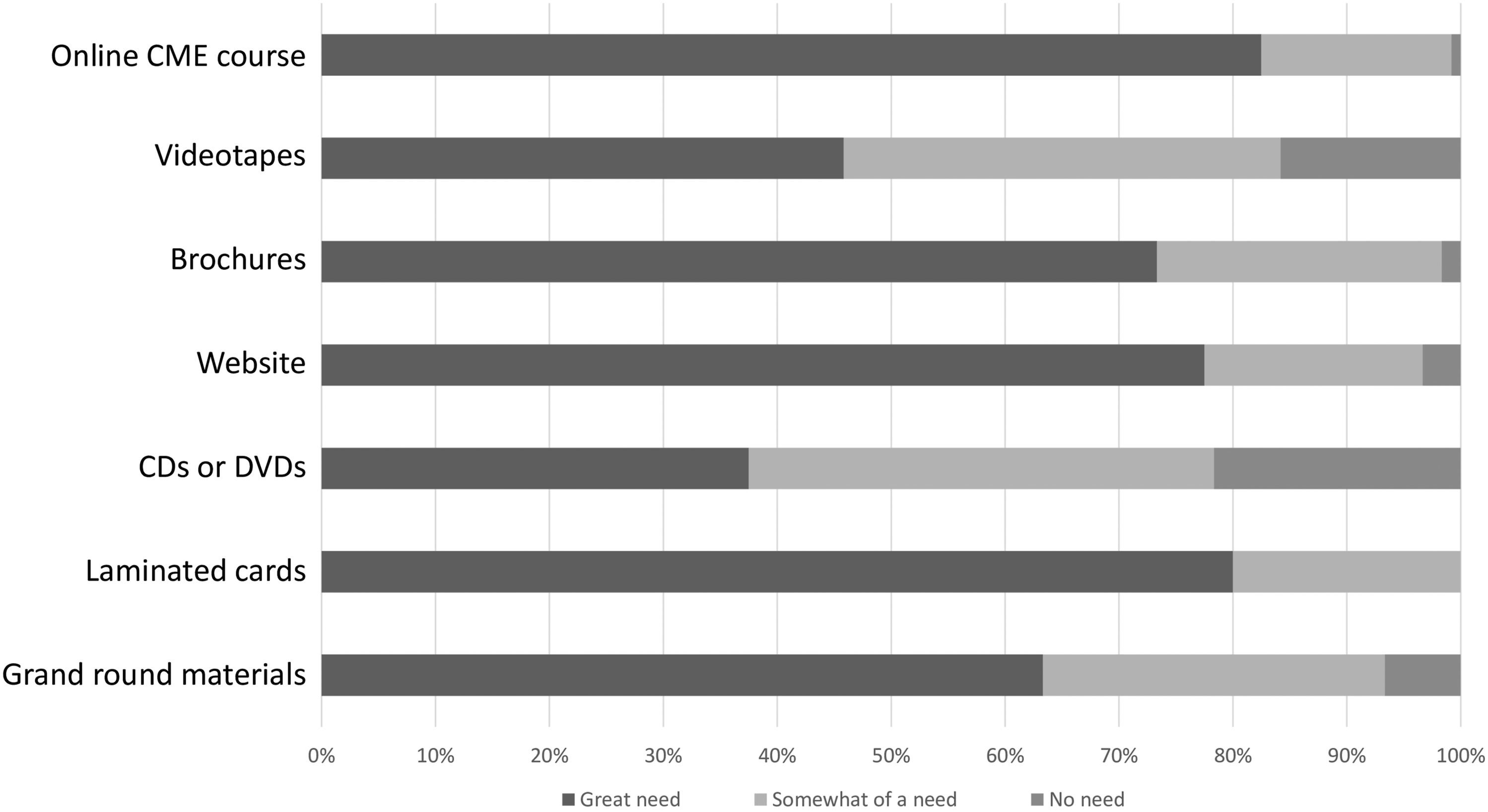
The last domain focuses on the clinical practice related to different types of information associated with permanent hearing loss that PCPs should perceive. All the items were rated as ‘great need’, ‘somewhat of a need’ and ‘no need’. In addition, various materials preferred by PCPs that can serve as tools for educating the patients were also reported. The data was entered in an Excel spreadsheet. Descriptive analysis was applied whereby the data were presented as the frequency of responses and percentage.
This study has been approved by the Medical Research and Ethics Committee (MREC), Ministry of Health Malaysia (NMRR-21-1253-59,900).
Results
The demographic data of primary care physicians.

Total number of responses from 120 Primary health care physicians on risk factors for childhood hearing loss.
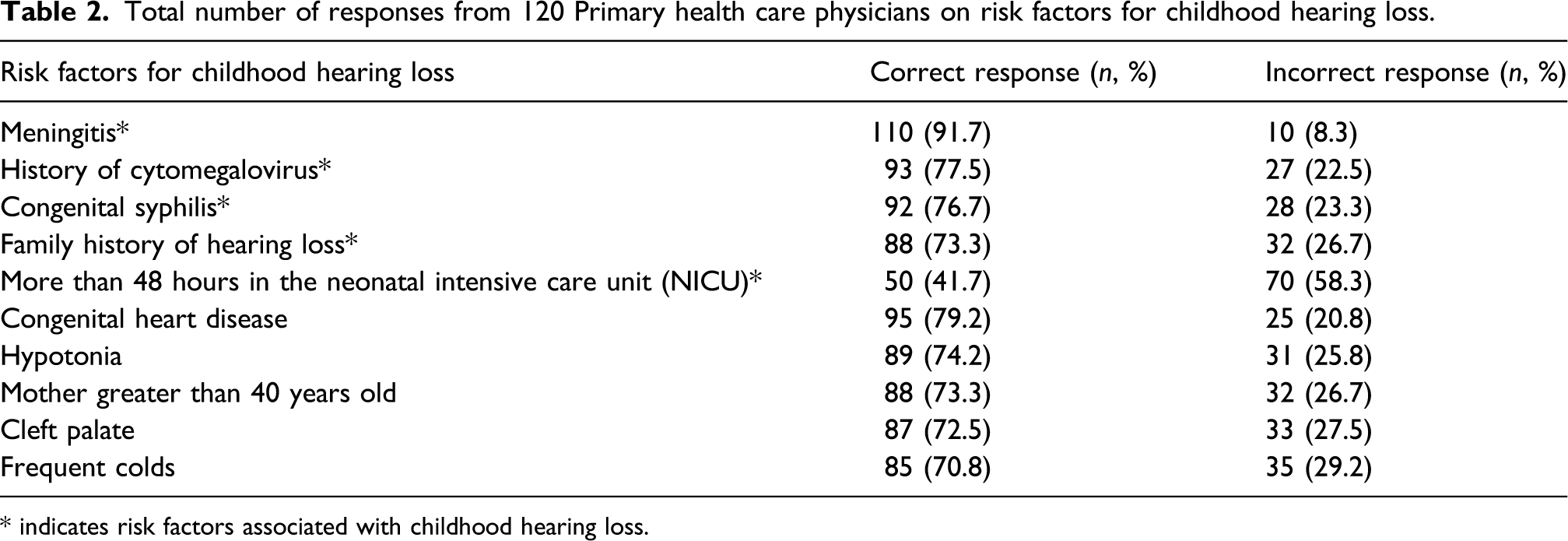
* indicates risk factors associated with childhood hearing loss.
Responses by primary health care physicians regarding the importance of newborn hearing screening and childhood hearing loss.
The majority of the PCPs believed that there was a ‘great need’ for them to comprehend various information regarding HL including genetics, hearing devices, educating patients, intervention options and hearing screening methods and protocol as depicted in Figure 1. To a lesser extent, some of them reported that there was ‘somewhat of need’ and ‘no need’ for this information. With regards to the dissemination of the materials for patient education, the respondents recommended online continuous medical education (CME) courses, laminated cards and websites as the main tools to be used as illustrated in Figure 2. Responses obtained from primary care professionals on different types of information with regard to childhood hearing loss. Types of materials preferred by primary care physicians to be used in patient education.
Discussion
This study demonstrated that approximately four-fifths of the respondents had no experience in managing children with permanent HL during the past 1-year of their practice. These findings were congruent with a study by Sydlowski et al in which HL was less prioritised by PCPs in their clinical practice as compared to other major medical issues such as Diabetes mellitus, hypertension, respiratory illness or mental problems. 9 In another study by Cohen et al, 40% of the PCPs admitted that HL assessment was not routinely explored during clinical practice due to time limitations. 10 One local study also replicated a similar finding. 11
As a prime point of contact, most of the children will be seen by PCPs in well-child clinics. In the Malaysian context, the UNHS program has been initiated in most of the tertiary public and private hospitals. As part of the integrated system, the results of NHS have been incorporated in the Babies and Children Health Record Book whereby the PCPs have direct access to NHS results. Although the majority of the PCPs (90.83%) acknowledged that NHS is very important, a small numbers of them (12.50%) commented to be very confident in interpreting NHS results to parents, tailoring to the scarcity in managing HL among children in primary care facilities. Many studies shared similar observations.9,11–13 Children who failed initial newborn hearing screening are supposed to have another hearing tests to confirm the diagnosis. However some of them did not come for the subsequent hearing testing and such cases can be picked up by PCPs during well-child visit in primary care in order to facilitate the referral to Otorhinolaryngologists or Audiologists.
Pertaining to the training received by PCPs, the majority (76.67%) responded that current medical training insufficiently equips them with adequate knowledge of HL among children. This finding was also observed by other studies.12,13 Most of the PCPs agreed that undergraduate training served as an essential platform in cultivating the knowledge of HL as well as the importance of NHS. Therefore, it should be emphasized to all clinical schools to incorporate teaching on HL during undergraduate teaching to prepare all medical doctors for managing such cases during their clinical practice later on. Better knowledge will facilitate the individuals to have positive attitudes and unequivocal responsibilities in any job assignment.
Literature mentioned that PCPs demonstrated a lack of understanding of treatment options for HL in which they were unaware of the usage of hearing aids in amplifying the sound.11,13 However, based on our findings, the majority of PCPs gave affirmative feedback on NHS, early intervention options, acquiring information on HL and hearing intervention. They acknowledged that all PCPs should gain such information with regard to permanent HL in childhood. In this modern technologies era, most PCPs believe that online CMEs is the most preferred platform for delivering teaching as it is cost-effective and time-consuming. In addition, the majority of them still preferred laminated cards, websites and brochures as mediums for disseminating the information on HL in order to educate the patients. Less popular materials for delivering the information are CDs, DVDs and videotapes.
In general, the findings in this study are important because PCPs serve as initial encounters whenever patients require medical attention. Therefore, the best way to tackle HL issues is to educate the PCPs. 10 Not only this approach will capture the prevalence of childhood HL, but it will also facilitate early referral to the Otorhinolaryngologists and Audiologists in the tertiary hospitals. PCPs have vast responsibilities in managing various medical conditions, thus it is prudent to create a more standardised way of detecting HL during well-child clinics. Furthermore, PCPs should listen to any complaint brought up by the parents. Literature have shown that parents have the highest index of suspicion about their children’s HL. 2 Therefore, all PCPs should take this matter vigilantly whenever the parents express their concerns regarding suspicion of HL or delayed speech.
There are a few limitations that need to be considered in this study. One of the limitations is recall bias attributed to the self-reported online questionnaires. The application of QR code in answering the questionnaire might contribute the low response rate. In addition, the feedback might be influenced by external factors such as the opinions of others. Majority of the respondents are medical officers with half of them only had experienced in primary care centres for less than 5 years. This study was conducted among PCPs in Johor state, it might not be representative of nationwide views. A study with involvement of a larger scale at the multi-state level is recommended in the future.
Conclusion
Despite acknowledging the importance of HL, the awareness and practice levels are still unsatisfactory among PCPs. This study highlighted the need for a paradigm shift in improving HL management at primary care facilities in Malaysia. Continuous collaborations between PCPs and Otorhinolaryngologists as well as Audiologists are highly warranted. Finally, empowering resourceful information on permanent childhood HL to all PCPs is essential.
Footnotes
Acknowledgements
The authors would like to thank the Director General of Health Malaysia for the permission to publish this paper. We thank all Primary Care Professionals in Johor state who involved in completing the questionnaires.
Ethical consideration
This study has been approved by the Medical Research and Ethics Committee (MREC), Ministry of Health Malaysia (NMRR-21-1253-59900).
Author contributions
• KM: Conceptualization, Writing – original draft
• TMITK: Conceptualization, Writing – review & editing
• SMM: Data curation, Writing – review & editing
• LHM: Methodology
• MAAL: Methodology
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data are available upon request.