
Abstract
A 12-year-old girl with known bilateral enlarged vestibular aqueducts presented with vertigo and sudden profound hearing loss in her only hearing ear after COVID-19 infection. The hearing remained unchanged after systemic steroids, prompting treatment with salvage intratympanic dexamethasone and hyperbaric oxygen therapy with improvement in her hearing. This case report highlights the success of hyperbaric oxygen therapy in treating sudden sensorineural hearing loss and aims to raise awareness on its role in treating sudden hearing loss in patients with enlarged vestibular aqueduct.
Introduction
We present the first reported use of hyperbaric oxygen therapy for sudden hearing loss in a child with enlarged vestibular aqueduct in Singapore.
Case report
A 12-year-old girl of Chinese ethnicity, with no perinatal risk factors for hearing loss and passed the newborn hearing screen at birth, was diagnosed at age five with profound right sudden sensorineural hearing loss (SNHL). At age seven, following an episode of left fluctuating hearing loss, computed tomography (CT) scan of the temporal bone was obtained and confirmed bilateral enlarged vestibular aqueducts. Figure 1 She was fitted with a left hearing aid. She had 3 further episodes of left fluctuating hearing loss and all the episodes recovered with oral steroids. CT temporal bone axial cuts: bilateral enlarged vestibular aqueduct (left), dysplastic modiolus with incomplete partition between apical and middle turns (right).
She has no other medical history and attends mainstream school. She has a male cousin with bilateral sensorineural hearing loss (SNHL) who underwent cochlear implantation. The cause of his hearing loss is unknown.
After COVID-19 infection, she developed vertigo associated with a fourth episode of sudden profound hearing loss in her only hearing ear. Otoscopic examination was unremarkable. Audiogram performed showed bilateral profound hearing loss. Despite hearing aid adjustments, the hearing was not serviceable. She was admitted for further management and started on intravenous dexamethasone at 0.1/mg/kg thrice a day, which was subsequently changed to a tailing dose of oral prednisolone – 1 mg/kg/day for seven days, followed by 0.5 mg/kg/day for three days and 0.25 mg/kg/day for three days. Repeated hearing assessment after completing the course of systemic steroids showed no improvement in hearing.
The patient underwent salvage treatment with concurrent left intra tympanic (IT) dexamethasone injection and hyperbaric oxygen therapy (HBOT) after the course of systemic steroids. She received six IT dexamethasone injections over a course of two weeks as well as fifteen sessions of HBOT at the Hyperbaric & Diving Medicine Centre of a tertiary institution. Treatment was conducted at pressures of 2 atmosphere absolute (ATA). Each session involved achieving pressure of 2 ATA over 10 minutes on air, followed by 90 minutes of oxygen at 2 ATA (with a 5-minute air break in between), then decompression to sea level on oxygen over 10 minutes Figure 2. HBOT regime.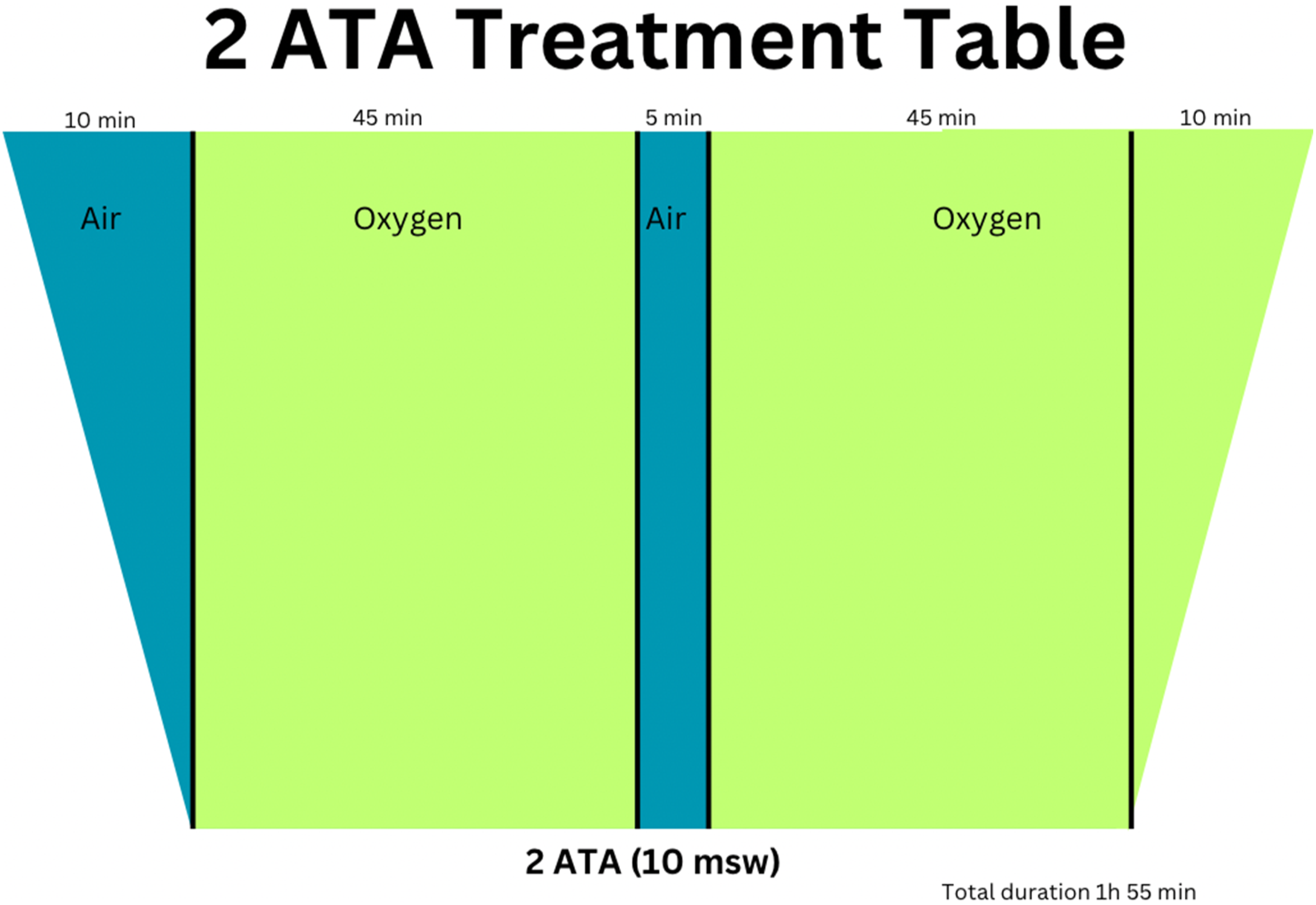
Hearing Thresholds before, during and after the hearing loss episode.


Left Hearing thresholds at baseline (solid line), following sudden hearing loss (dotted line) and after completion of salvage therapy (dashed line).
Discussion
Enlarged vestibular aqueduct (EVA) is the most common radiographic abnormality identified in paediatric hearing loss. 1 First described by Valvassori in 1978, it is associated with congenital or childhood-onset hearing loss. EVA can be either an isolated finding or coexist alongside other inner ear malformations. 2 Its prevalence has been reported to be as high as 32% in hearing-impaired children. 3
The clinical presentation of EVA is highly variable. Children may present with varying degrees of auditory and vestibular symptoms. 4 A minority remain asymptomatic and are picked up incidentally. 5 Hearing loss in EVA can occur suddenly or in a stable progressive fashion. 6 Acute deterioration of hearing has been described after minor head injury, barotrauma, common cold, longtime exposure to sunshine and extreme exercise. 7 By itself, EVA is reported to carry a 39.6% risk of progressive hearing deterioration. 8 Various theories regarding the pathophysiology of hearing loss in EVA have been proposed to date with no clear consensus. 9 Interestingly, the radiologically identified side of EVA may not correspond with the side of hearing loss. 5 Hence, the structural abnormality in itself may not be the sole pathogenic factor and instead be a reflection of pathology at a molecular level. 9
Common treatment options for hearing loss in EVA include the use of hearing aids, with a view to cochlear implantation if hearing is no longer serviceable. Steroid therapy can be given in episodes of acute hearing deterioration, 10 similar to its use in idiopathic sudden sensorineural hearing loss (SSNHL). 11
HBOT has been reported to be effective in the treatment of sudden sensorineural hearing loss in EVA albeit mainly case reports and series in published literature. In those cases, HBOT was typically prescribed as salvage therapy after failure of medical therapy. During HBOT, patients are placed in a pressurized chamber where they breathe 100% oxygen at pressures greater than 1 ATA. 11 The first reported case of successful HBOT treatment of SSNHL in patients with EVA was in 1999 by Nakashima et al. 12 The authors postulated that the decrease in cerebrospinal fluid (CSF) pressure during HBOT would address the transmission of high CSF pressure from the intracranium to the inner ear via the endolymphatic duct and sac. Additionally, the increased partial pressure of oxygen from HBOT allows greater oxygen delivery to the cochlear, 11 a structure with a tenuous blood supply. This hyperoxaemia can address cochlear ischaemia, which the authors felt were probable in EVA.
In 2011, the Undersea and Hyperbaric Medical Society (UHMS) recognised sudden sensorineural hearing loss as an indication for HBOT, and recommends starting HBOT within 2 weeks of symptom onset. In the setting of idiopathic SSNHL, the combination of HBOT with steroids may be chosen as initial or salvage therapy. 11 Recently published in 2023, Alde et al’s study of 49 subjects suggests that starting HBOT within three days of symptom onset enhances recovery. 13
Presently, there are no prospective or large-scale studies to evaluate HBOT for EVA related SSNHL. Similar to prior case reports, our patient received salvage HBOT when there was no hearing improvement with initial medical therapy. More studies are required to evaluate the optimal time from symptom onset to HBOT commencement. It is also unclear if HBOT should be administered alone, or in combination with steroids. Nakashima 12 and Furuhashi 14 et al investigated HBOT as a single treatment modality. Shilton 15 et al and our practice advocate for concurrent HBOT and steroid treatment. This is in keeping with the clinical practice guideline for idiopathic SSNHL which recommends that HBOT, if offered, should be administered in combination with steroid therapy. 11 To date, there is insufficient evidence to determine which approach is superior for treatment of EVA related SSNHL.
HBOT is not without its risks. General complications include barotrauma to the ears, sinuses and lung. In the paediatric age group, barotrauma of the middle ear is of particular significance due to eustachian tube dysfunction contributed by the shorter and more horizontal nature of the eustachian tube, more prominent adenoids and frequent upper respiratory tract infections. The patient presented by Shilton et al 15 was unable to complete the full course of HBOT in view of ear pain from depressurisation of the chamber. However, in a suitable patient, HBOT could reverse hearing loss and have a positive impact on his/her lifestyle.
In our local population, traditionally, HBOT is prescribed mainly for decompression illness. With increasing understanding and awareness of the mechanism of action of HBOT, the list of approved indications for HBOT has expanded. More physicians are now referring patients with poorly healing wounds for HBOT. A small proportion of ENT surgeons refer patients with SSNHL for HBOT but typically as salvage therapy. This report aims to raise awareness of the efficacy of HBOT in SSNHL in patients with EVA. While this is a minority of patients with SSNHL, there is significant plough back in terms of improvement to quality of life and learning for younger patients.
Conclusion
This case adds on to the existing data on use of HBOT for sudden hearing loss in patients with EVA. Further studies are warranted to evaluate its use. We hope to highlight the potential of HBOT as a treatment option in medically refractory cases, which may halt progression to non-serviceable hearing necessitating cochlear implantation.
Footnotes
Author contributions
GLM wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Data Availability Statement
Data sharing is not applicable to this article as no datasets were generated or analysed during the current study.