
Abstract
A 28-year-old man presented with central exertional pleuritic chest pain, associated with dyspnoea and reduced effort tolerance on the background of 1-week of upper respiratory tract infection like symptoms with recent overseas travel to Southeast Asia. Physical examination was unremarkable. Electrocardiogram showed sinus rhythm. Raised high-sensitivity troponin-T levels were noted. Transthoracic echocardiogram demonstrated normal ejection fraction and no regional wall motion abnormalities. Computer tomography (CT) coronary angiogram did not show obstructive coronary artery disease or structural abnormalities. The patient subsequently developed diarrhoea and abdominal discomfort localised to the right iliac fossa. Given this, intraabdominal imaging was performed and revealed features of ileocolitis. Stool Polymerase Chain Reaction testing detected Enteropathic Escherichia Coli. As no cause for raised troponins was found, a cardiac MRI was performed. On late gadolinium enhancement (LGE) imaging, there was subtle basal to mid septal midwall and inferolateral subepicardial uptake. LGE pattern and tissue characterisation parameters suggested recent episode of mild myocarditis. He was treated with a course of intravenous antibiotics with improvement of symptoms. Repeat cardiac MRI also demonstrated interval improvement 1 month after the acute event with only residual subtle subepicardial enhancement in the basal inferolateral wall.
Introduction
Myocarditis is an inflammatory disease process of the heart resulting from infections, immune system activation, or drug exposure. Among infective causes, Escherichia Coli (E. Coli) is rarely isolated as the cause of myocarditis and the source of E. Coli is commonly from the urinary tract. Here we present the first known case of E. Coli induced myocarditis in a premorbidly healthy young man.
Case report
A 28-year-old man presented to the emergency department with a 4-day history of central exertional pleuritic chest pain, associated with dyspnoea and reduced effort tolerance.
This was on the background of 1-week of upper respiratory tract infection like symptoms with recent overseas travel to Borneo in Southeast Asia. He had no past medical history of ischaemic heart disease (IHD) or family history of IHD or sudden cardiac death.
Physical examination revealed regular and dual heart sounds, lungs were clear to auscultation and there was no pedal oedema.
Electrocardiogram showed sinus rhythm.
As raised high-sensitivity troponin-T levels (68 > 60>45) were noted, the patient was admitted to the cardiology team and underwent further work-up. Transthoracic echocardiogram demonstrated no structural heart abnormalities with normal ejection fraction and no regional wall motion abnormalities. Computer tomography (CT) coronary angiogram did not show any obstructive coronary artery disease or structural abnormalities.
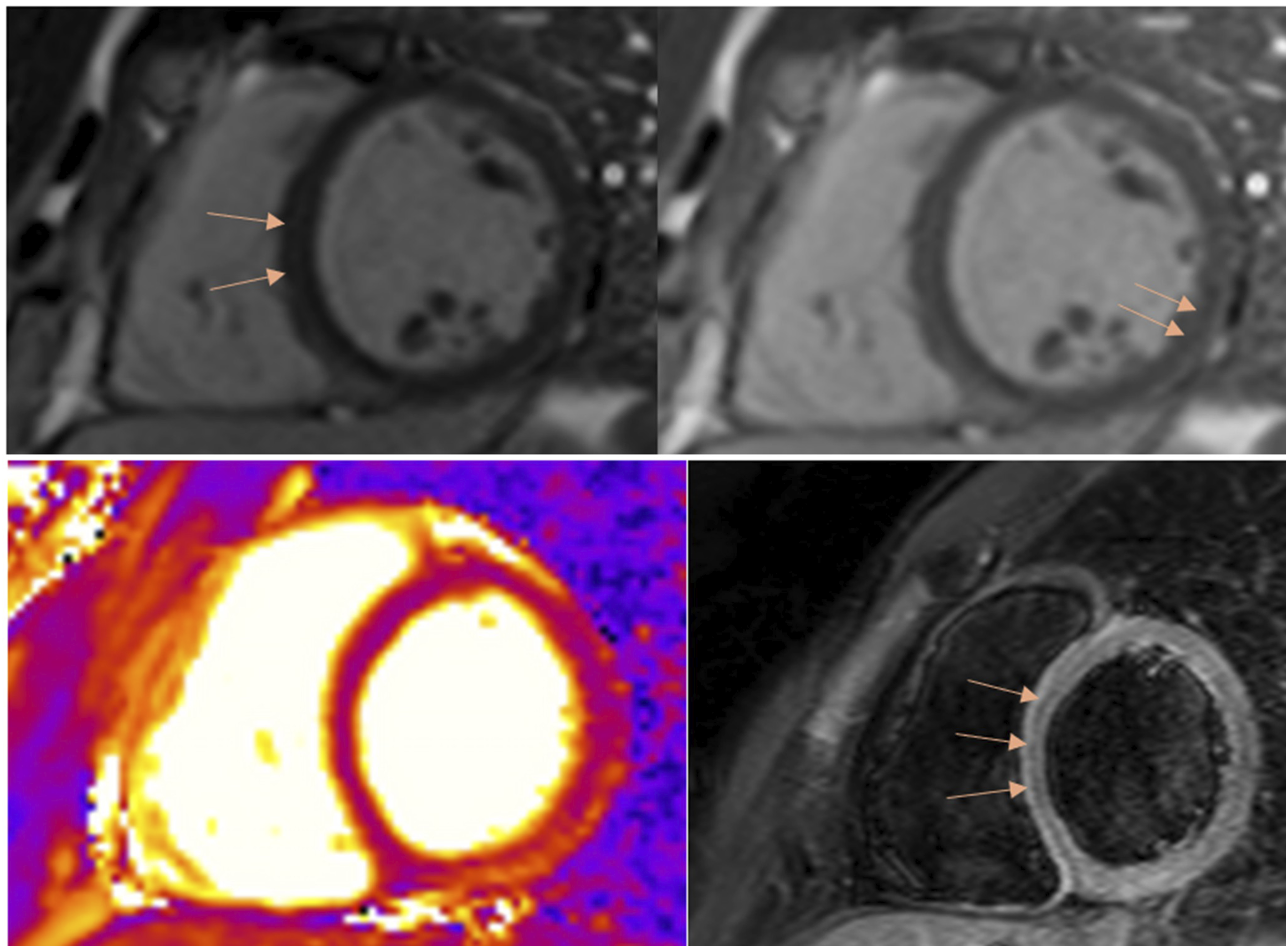
During the course of his admission, the patient developed diarrhoea and abdominal discomfort localised to the right iliac fossa. Given this, intraabdominal imaging was performed and revealed features of ileocolitis (Figure 1); he does not have any history of inflammatory bowel disease. Considering his significant travel history in Southeast Asia, peripheral blood films and cholera PCR were sent, which were negative. Respiratory polymerase chain reaction (PCR) test was also negative. While blood cultures and stool cultures were unyielding, stool PCR detected Enteropathic E. coli. Cardiac magnetic resonance (CMR) imaging was subsequently performed. On late gadolinium enhancement (LGE) imaging, there was subtle basal to mid septal midwall (Figure 2(a)) and inferolateral subepicardial uptake (Figure 2(b)). Global high T2 intensity signal on T2-weighted images (Figure 2(c)) and hyperintense myocardium on turbo inversion recovery magnitude (TIRM) sequences (Figure 2(d)), were also demonstrated, suggestive of ongoing myocardial oedema. The LGE pattern and tissue characterisation parameters suggest a recent episode of mild myocarditis.
1
Initial CT abdomen pelvis showing mural thickening of ascending colon, caecum and terminal ileum suggestive of ileocolitis. Initial CMR showing septal midwall LGE uptake (a) and inferolateral subepicardial LGE uptake (b) on LGE SAX PSIR. Global high T2 intensity signal (c) and hyperintense myocardium on TIRM (d) suggestive of ongoing myocardial oedema.
He was treated with a course of intravenous antibiotics with improvement of symptoms, with interval intraabdominal imaging corroborating this with resolution of ileum thickening (Supplemental materials). Repeat CMR imaging also demonstrated interval improvement 1 month after the acute event with only residual subtle subepicardial enhancement in the basal inferolateral wall (Figure 3). Repeat CMR showing improvement of inferolateral subepicardial LGE uptake on LGE SAX PSIR (left) and normalisation of T2 values suggesting no significant myocardial oedema (right).
Discussion
In a premorbidly healthy young male patient with chest pain and reduced effort tolerance associated with an infective prodrome, myocarditis is an important consideration particularly in the context of elevated troponins. 2 Patients with myocarditis may develop serious complications such as heart failure, conduction abnormalities and arrhythmias, 3 thus early diagnosis is pertinent in management. Unlike previous case reports of E. coli myocarditis associated with urinary tract infections, we report the first case of E. coli myocarditis associated with ileocolitis.
Endocardial biopsy was previously the gold standard to diagnose myocarditis but it is not routinely performed in clinical practice due to its invasiveness and limited sensitivity. 4 With the introduction of CMR imaging, the diagnostic methods of myocarditis have broadened.4,5 According to the 2018 Lake Louise Criteria, diagnosis of myocarditis with CMR imaging is made if at least one T1-based criterion (increased myocardial T1 relaxation times, increased extracellular volume fraction, positive LGE) and one T2-based criterion (increased myocardial T2 relaxation times, visible myocardial oedema, increased T2 signal intensity ratio) are met.4,6 This is consistent with the findings in our patient. Additionally, apart from the non-invasive nature of CMR imaging, its findings also confer prognostic significance, with the presence of LGE being an independent predictor of adverse cardiovascular outcomes.1,7
Consistent with other accounts of E. coli induced myocarditis, 8 the myocardial inflammation is likely directly related to the pathogenicity of the E. coli pathotypes. 9 The exact mechanism for E. coli myocarditis remains uncertain but is postulated to involve bacterial invasion, production of toxins and releasing outer membrane vesicles which induce an inflammatory response through triggering cytokine release. 10 As the frequency of bacterial (and E. coli) myocarditis is low, there are no specific guidelines for this group of patients and management follows that of non-bacterial myocarditis. Pillars of management include supportive treatment of arrhythmias or heart failure, aetiology-targeted therapy and in certain cases, immunomodulatory or immunosuppressive therapy2,4 with follow-up to ensure resolution of the disease due to high rates of relapse. 4
Conclusion
Given the uncommon complication of myocarditis in the setting of a bacterial infection, it is prudent for clinicians to have a high clinical index of suspicion.
Supplemental Material
Supplemental Material - A curious case of Escherichia coli induced myocarditis
Supplemental Material for A curious case of Escherichia coli induced myocarditis by Shyn Yi Tan, Samuel Ji Quan Koh, Laura Chan, Jun Hua Chong, Swee Yaw Tan in Proceedings of Singapore Healthcare
Footnotes
Consent to participate
Written informed consent was obtained from the patient for their anonymised information to be published in this case report, including accompanying images.
Author contributions
TSY and SK wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.