
Abstract
Research report: Introduction
According to the Centre for Disease Control and Prevention (CDC), effective hand hygiene is crucial in curbing the spread of infection in hospitals 1 . It has been well established that contaminated hands of healthcare workers are the main source of spread of nosocomial infection in hospitals1–4. Proper hand hygiene helps reduce the proliferation and spread of germs in healthcare settings. In line with this, the “bare below elbows” (BBE) policy was introduced in the United Kingdom (UK) in September 2007 to improve hand hygiene practices and hence reduce the spread of infection in healthcare settings. 2 The policy recommends that no long-sleeved clothing, jewelry or wristwatches should be worn when in direct contact with patients, apart from a simple wedding band.2,5,6
Despite the importance of hand hygiene in preventing hospital-acquired infections, there remains no global agreement on the effectiveness of the BBE concept.7,8 Additionally, there is no strong evidence that the BBE policy reduces nosocomial infections or improves hand cleanliness.8,9 The BBE policy has faced criticism for being seen as bureaucratic and impractical, with some calling it an “unnecessary bureaucracy 10 ” and “a cheap soundbite 11 ”. Several studies argue that the disadvantages of BBE, such as the inability to use a wristwatch, outweigh its intended benefits, particularly in clinical tasks like accurately measuring pulse and respiratory rates10,12. These have significant implications on patient care and safety. Additionally, BBE has posed challenges in accommodating cultural practices, leading to adjustments in some regions, including the UK and Singapore, to respect personal and cultural preferences without compromising infection control. 13
Should healthcare workers be allowed to wear wrist watches during patient care?
Smart watches have been gaining popularity in their ability to collect valuable health data of the user, and can potentially transform the way we receive alerts, conduct surveillance and communicate while at work. 14 Certain apps enable doctors to receive alerts via smartwatches to get immediate notification when the test results for their patients are released. However, current local infection control policies negate the use of smartwatches in healthcare settings due to concerns related to the heightened risk of infection transmission. The increased popularity of smart watches has led to a call to examine the impact the wristwatch may have on infection control practices.
The role of wristwatches in infection control practices remains inconclusive. Studies have not examined the impact of wristwatches in isolation from other accessories, making it unclear how wristwatches alone contribute to infection risks.8,12,15 While some research suggests wristwatches are linked to higher bacterial contamination on the wrist, this does not necessarily translate to increased hand contamination unless the watch is handled frequently.5,12 Furthermore, there is no definitive evidence that wrist contamination directly contributes to infection transmission, nor that washing wrists effectively reduces infection rates. 3
Methodological inconsistencies in hand hygiene research make it challenging to compare findings across studies. Various techniques, such as the glove-juice method to analyse bacteria counts, 10 swab sampling, 5 and agar plate incubation, 7 have been used to assess bacterial growth on hands and wrists. Other studies, like Szumska et al. (2022), analysed bacterial growth via observation. This variation limits the ability to draw definitive conclusions, highlighting the need for standardized methods in future research to accurately assess microbial contamination and its role in nosocomial infections.
A simulation study was conducted in two phases to evaluate whether wearing a wristwatch 1) hinders effective hand hygiene and 2) contributes to the spread of germs in the hospital. 30 healthcare workers working in an academic medical centre were recruited within a single day in June 2024 (The sample comprised seven doctors, five medical students, four research assistants and 14 registered nurses).
Participants were recruited via convenience sampling and the study was conducted within a simulation lab in the hospital. GloGerm lotion was used to mimic the presence and transmission of germs. (GloGerm lotion is commonly used in teaching to illustrate flaws in existing handwashing techniques.5,6 It simulates germ colonies on hands and light up under ultraviolet lighting. The watches used in the study were Apple watches with aluminium casing and single loop silicone bands. Preliminary tests were conducted in which GloGerm lotion was applied to the cases and straps and washed off with alcohol-based hand rub. Findings revealed that 1) Aluminium casing was able to withstand repeated exposure to alcohol-based disinfectants without any visible damage, 2) GloGerm was least adherent to the silicone band material as compared to the metal straps, and 3) a single loop band prevented GloGerm from dwelling within adjustment holes and overlapping regions on adjustable watch straps).
In the first phase of the study, participants were required to perform hand hygiene with and without a wristwatch. A member of the study team was assigned to apply GloGerm lotion on the hands of participants to ensure standardization of the amount of lotion applied and the area on which it was applied. The same team member also observed to ensure compliance to the seven steps of hand hygiene. UV images of both hands pre- and post- hand hygiene with alcohol handrub were taken, both in the presence and in the absence (control) of a wristwatch (refer to Figure 1). Hand hygiene simulation workflow.
In the second phase of the study, participants were required to test the spread of germs from one “dirty” mannequin to another mannequin in the presence of a wristwatch, in adherence to the World Health Organization’s (WHO) moments of hand hygiene.
1
GloGerm was applied by a member of the study team on the arm of a mannequin to enquire standardization of the amount of GloGerm applied on the “dirty” mannequin. Participants were required to touch the “dirty” mannequin, perform hand hygiene with alcohol handrub (Moment 4: After touching a patient), before touching the “clean” mannequin. UV images of the participants hands pre- and post- touching the “dirty” mannequin, after hand hygiene, and the “clean” mannequin after being touched were taken (refer to Figure 2). Germ transfer simulation workflow.
Visual analysis of the UV images were analysed by two reviewers from the study team and presented in Figure 3. Visual analysis is a common method of analysis used in previous studies to evaluate the spread of germs and/or in the evaluation of the effectiveness of hand hygiene.
8
Both reviewers independently evaluated the images and subsequently discussed any discrepancies. No disagreements were observed between the reviewers in their analyses. Hand hygiene and germ transfer simulation.
Results of hand hygiene and germ transfer simulation.
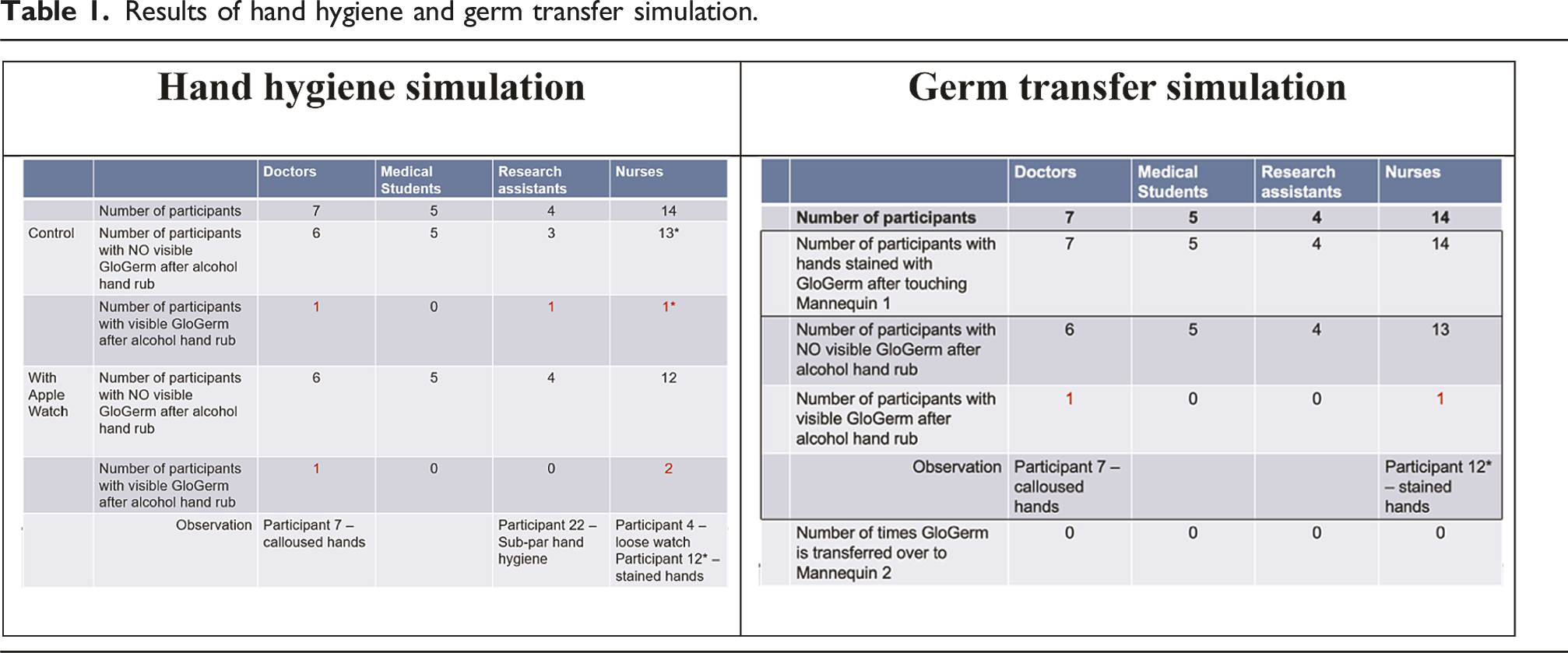
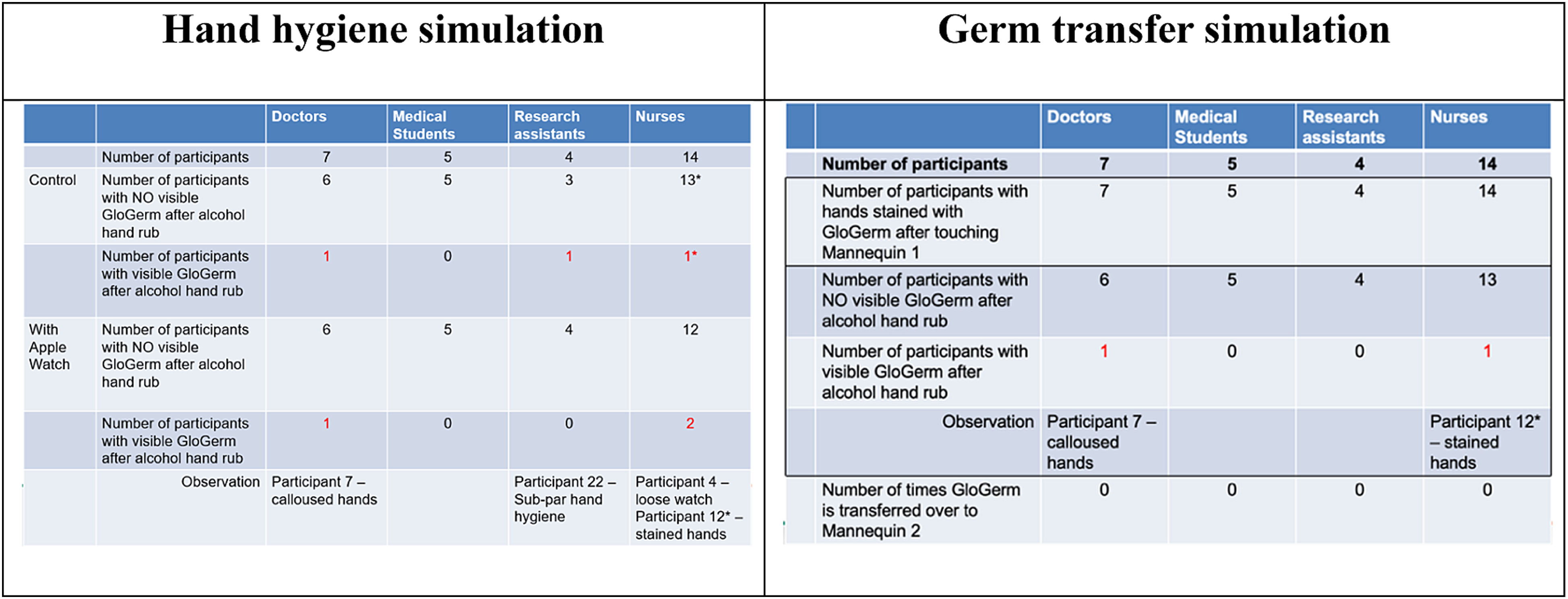
Reasons for the visible “germs” among the three participants post-hand hygiene can be attributed to calloused hands (Participant 7), wearing a watch that was too loose (Participant 4), and having “stained” hands (Participant 12). To elaborate, GloGerm solution adhered to the crevices of the callouses of the hands of Participant seven and could not be removed despite adequate hand hygiene. Participant four had small wrists and the watch was observed to turn around the wrist and move up and down – this posed as a difficulty for the participant to perform effective hand hygiene. Participant 12 had hands that were stained with turmeric oil which “lit up” under UV light – thus, it provided an inaccurate depiction of the presence of “germs” pre- and post- hand hygiene.
There were no visible signs of transfer of germs from the “dirty” mannequin to another with proper hand hygiene. While hands were observed to be visibly soiled after touching the dirty mannequin, there was none to minimal germ light up on the hands after hand hygiene moment 4. No significant signs of any germ transfer were seen in the UV images taken thereafter. Similarly, “false” light up of GloGerm were seen in Participants 7 and 12 which would be attributed to the same reasons above (Table 1).
Discussion and conclusion
Findings from the study suggest that wearing a wristwatch may not affect the effectiveness of hand hygiene and neither does it significantly contribute to the spread of germs. A good watch fit and strict adherence to hand hygiene practices can help mitigate infection control risks associated with the presence of a wristwatch. 12
A well-fitted watch prevents it from sliding freely on the wearer’s wrist or forearm, enabling effective cleaning of the hands and wrists in accordance with the seven steps of hand hygiene. 12 Moreover, consistent adherence to hand hygiene protocols can greatly diminish the risk of germ transmission in healthcare settings by ensuring that hands are thoroughly cleaned at key moments, effectively interrupting the spread of pathogens 1 . Evidence shows that when participants consistently followed the hand hygiene protocol—specifically, Moment 4: using hand rub after patient contact—the bacterial load on their hands was significantly reduced, thereby limiting germ transfer to a clean mannequin (refer to Steps C and D in Figure 2).
To conclude, the presence of a wristwatch does not appear to affect the effectiveness of hand hygiene or contribute to the spread of germs. The study’s findings indicate that compliance with proper hand hygiene practices plays a more crucial role in preventing the spread of infection than the mere presence of a wristwatch. The impact of wearing wristwatches can be mitigated by placing a greater emphasis on comprehensive hand hygiene education. Hospitals could revisit existing policy and guidelines to allow healthcare workers to wear wristwatches during patient care, and henceforth leverage on the benefits associated with the introduction of smart watches into patient care. To draw definitive conclusions and provide a more reliable evaluation of this phenomenon, a larger-scale study should be conducted.
Footnotes
Acknowledgements
We would like to thank Apple Singapore for provision of the watches and straps for the simulation study, as well as all our participants for their involvement in the study.
Ethical considerations
This study does not fall within the definition of research under SingHealth Centralised Institutional Review Board (CIRB) and was conducted as part of service evaluation. Therefore, ethics approval and participant consent was not required for this simulation study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.