
Abstract
Background
Patients with kidney failure face increased health risks during early haemodialysis due to physical and emotional challenges. Most patients begin haemodialysis using catheters, which increases mortality and complication risks. This study evaluates the impact of multidisciplinary clinics on vascular access and patient outcomes on haemodialysis.
Objectives
To compare the influence of multidisciplinary clinics with conventional clinics on the utilisation of definitive vascular access for haemodialysis.
Methods
This is a single-centre, retrospective cohort study included 145 patients newly started on haemodialysis. Patients were evaluated over a 12-month follow-up period (July 2018 to December 2020). The primary outcome was definitive vascular access for haemodialysis. Secondary outcomes included the frequencies of catheter-related bloodstream infections, intensive care unit admissions, and recurrent hospitalizations.
Results
The study analysed 53 and 92 participants in the multidisciplinary clinics and conventional groups, respectively. Although only 10% of patients started haemodialysis with definitive access, the multidisciplinary clinics group exhibited significantly higher utilisation of definitive vascular access after 6 months (OR = 2.44, 95% CI 1.16-5.26, p = .039). The multidisciplinary clinics group had lower risks of intensive care unit admission (OR 0.92, 95% CI 1.03-1.15, p = .026) and recurrent hospitalization (OR 0.13, 95% CI 2.06-26.68, p = .001). Although not statistically significant (OR 0.34, 95% CI 0.47-18.46, p = .709), the multidisciplinary clinics group had a lower incidence of catheter-related infections.
Conclusions
Multidisciplinary care significantly increases the use of definitive vascular access, reduces intensive care unit admissions, and hospitalization rates, demonstrating the effectiveness of comprehensive, coordinated care in managing patients on haemodialysis.
Introduction
Chronic diseases including chronic kidney disease (CKD), are becoming increasingly prevalent globally. 1 From 1990 to 2016, the burden of CKD has increased significantly, leading to a near-doubling of CKD-related deaths. 2 Despite medical advancements, the mortality rates of end-stage kidney disease (ESKD) remain higher than those of other major healthcare conditions. 3
The United States Renal Data System (USRDS) has shown that 80% of patients with ESKD in the United States start haemodialysis using catheters. 4 Echoing this trend, data from Singapore also show that only 28.5% of patients begin dialysis with an arteriovenous fistula. 5 This is concerning, as not using arteriovenous access within 6 months is linked to a 53% higher mortality rate. 6 Additionally, haemodialysis catheters carry a higher risk of bloodstream infections, which can lead to sepsis and intensive care needs, as well as a higher risk of catheter malfunctions requiring repeated hospitalization.7,8 Patients with ESKD face challenges beyond the physical aspects, including financial and emotional difficulties.9,10 Comprehensive care is crucial; however, the conventional single-nephrologist care approach may overlook these broader impacts and may leave patients unprepared for dialysis. To address this issue, our hospital has established a multidisciplinary clinic (MDC) involving nephrologists, renal coordinators, and social workers to provide holistic care.
This study aimed to evaluate the impact of the MDC on the use of definitive vascular access and related outcomes in patients undergoing haemodialysis, hypothesizing that the MDC approach would result in higher utilisation of arteriovenous fistulas or grafts, and lower rates of catheter-related bloodstream infections, ICU admissions, and recurrent hospitalizations compared to conventional care. The findings are expected to demonstrate the benefits of comprehensive, coordinated care provided by the MDC model for patients with end-stage kidney disease.
Definitive vascular access is defined as the use of an arteriovenous fistula (AVF) or arteriovenous graft (AVG) for at least three haemodialysis sessions, preferred for haemodialysis due to their durability and lower complication rates compared to central venous catheters.
Material and methods
Study design
This study is a single-centre, retrospective cohort analysis conducted at a regional hospital in Singapore. Its reporting format adheres to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. The study received approval from the Institutional Review Board (Ref: 2020/2041). Informed consent was not sought for the present study as retrospective data used was de-identified and anonymised before analysis was performed. The waiver was granted as no direct patient interventions were conducted outside routine care.
Participants
Data were collected from patients who began haemodialysis between July 2018 and December 2020. All participants were monitored for at least 12 months after starting dialysis.
Inclusion criteria
The study enrolled adult patients with advanced chronic kidney disease (CKD) stage 5, characterized by an estimated glomerular filtration rate (eGFR) of less than 15 mL/min/1.73 m2. Eligibility was determined by clinical progression and the expectation of dialysis initiation within 1 year, guided by factors such as worsening uraemic symptoms, biochemical trends, and nephrology evaluations.
Exclusion criteria
This study excluded patients who opted for conservative management or peritoneal dialysis as their primary modality, those who underwent kidney transplantation during the study period, and individuals who switched dialysis modalities from haemodialysis to peritoneal dialysis. Additionally, patients with incomplete clinical records (more than 50% missing data related to study outcomes), those lost to follow-up, or those with insufficient follow-up duration of less than 12 months were excluded.
Referral protocol
Referrals to the multidisciplinary clinic (MDC) were based on the treating nephrologist’s assessment of clinical factors, including eGFR trends and patient symptoms. Priority was given to patients expected to commence dialysis within a year to facilitate timely planning and creation of vascular access.
Intervention group
The MDC consists of nephrologists, renal coordinators, and medical social workers, and includes low-clearance clinics and transitional care clinics. Patients referred to the MDC attended the low-clearance clinics before dialysis initiation and the transitional care clinics within the first month after starting dialysis. The MDC model focuses on early intervention, continuous monitoring, patient education, and holistic support, with particular attention to establish a definitive vascular access for haemodialysis, aiming to reduce complications and hospitalizations.
Comparator group
Patients who declined MDC care continued follow-ups with their primary nephrologist in conventional clinics, typically with visits every 2-3 months.
Outcome measures and definitions
The study assessed the type of vascular access used and other secondary morbidity outcomes, such as CRBSI, ICU admissions, and recurrent hospitalizations. Definitive dialysis access was defined as using an AVF or AVG for at least three haemodialysis sessions. CRBSI was diagnosed in accordance with the KDOQI 2019 guidelines, which stipulate the necessity of a positive peripheral blood culture in the absence of other infection sources, along with a matching positive culture from the catheter hub or tip. 11 Hospital admissions were tracked via national electronic health records during the 12-month follow-up, with recurrent admissions defined as more than three within this period.
Data collection
Baseline demographic data were collected during initial nephrology visits at either the MDC or conventional clinic. Subsequent visits included retrospective gathering of clinical characteristics, biochemical data, and morbidity outcomes. Missing information was retrieved from the dialysis centre. The type of haemodialysis access was determined from clinical notes or dialysis flow sheets, considering using AVF/AVG if three successful cannulations occurred. Data were extracted from electronic health records using clipboard mapping and validated by two independent researchers, resolving discrepancies by consensus. Missing data (about 5%) were addressed using multiple imputation techniques. Sensitivity analyses compared imputed data with complete case analyses. To minimize selection bias, all eligible patients during the study period were included, regardless of clinical status. Information bias was mitigated by standardizing data extraction and using validated entry forms, reducing potential recall bias by relying on electronic health records.
Statistical analysis
Descriptive statistics are presented as counts (n) and percentages (%) or mean ± standard deviation (SD). Continuous variables were analyzed using Student’s t test for parametric data and the Mann-Whitney U test for non-parametric data. Fisher’s exact test was used for categorical events with fewer than five observations, while the chi-squared test was applied for other categorical variables. Statistical significance was set at p < .05. Binary logistic regression modelling identified potential independent predictors influencing the use of AVF/AVG at 6 months. All analyses were performed using IBM SPSS Statistics, version 27.0.
Confounding variables
The analysis adjusted for several confounders, including age, gender, ethnicity, comorbidities (diabetes, hypertension, obesity, cancer, ischaemic heart disease, and primary renal disease), and laboratory parameters (haemoglobin, calcium, phosphate, and albumin levels). These variables were selected based on their potential influence on vascular access outcomes and patient morbidity, as identified in previous major studies on haemodialysis vascular access.6,7 However, unmeasured factors such as socioeconomic status was acknowledged as limitations and could not be included in the analysis due to the retrospective nature of the study.
Results
Study summary
From July 2018 to December 2020, 212 patients progressed to ESKD. Of these, 164 chose haemodialysis, 21 opted for peritoneal dialysis, one received a kidney transplant, 18 chose conservative management, and eight were lost to follow-up. Of the 21 patients who selected peritoneal dialysis, 11 initially started with short-term haemodialysis before transitioning to long-term peritoneal dialysis. In the conservative care group, five patients eventually converted to dialysis as they were mostly hemodynamically unstable to continue without it. Among the 164 haemodialysis patients, 14 passed away, with none of the deaths attributed to catheter-related infections. Due to more than 50% of missing clinical data, three patients from the MDC and two from the conventional clinic were excluded from the analysis, resulting in a final cohort of 145 patients. The details of patient selection are shown in Figure 1. Flowchart for patient selection for multidisciplinary clinic versus conventional solo nephrologist clinic.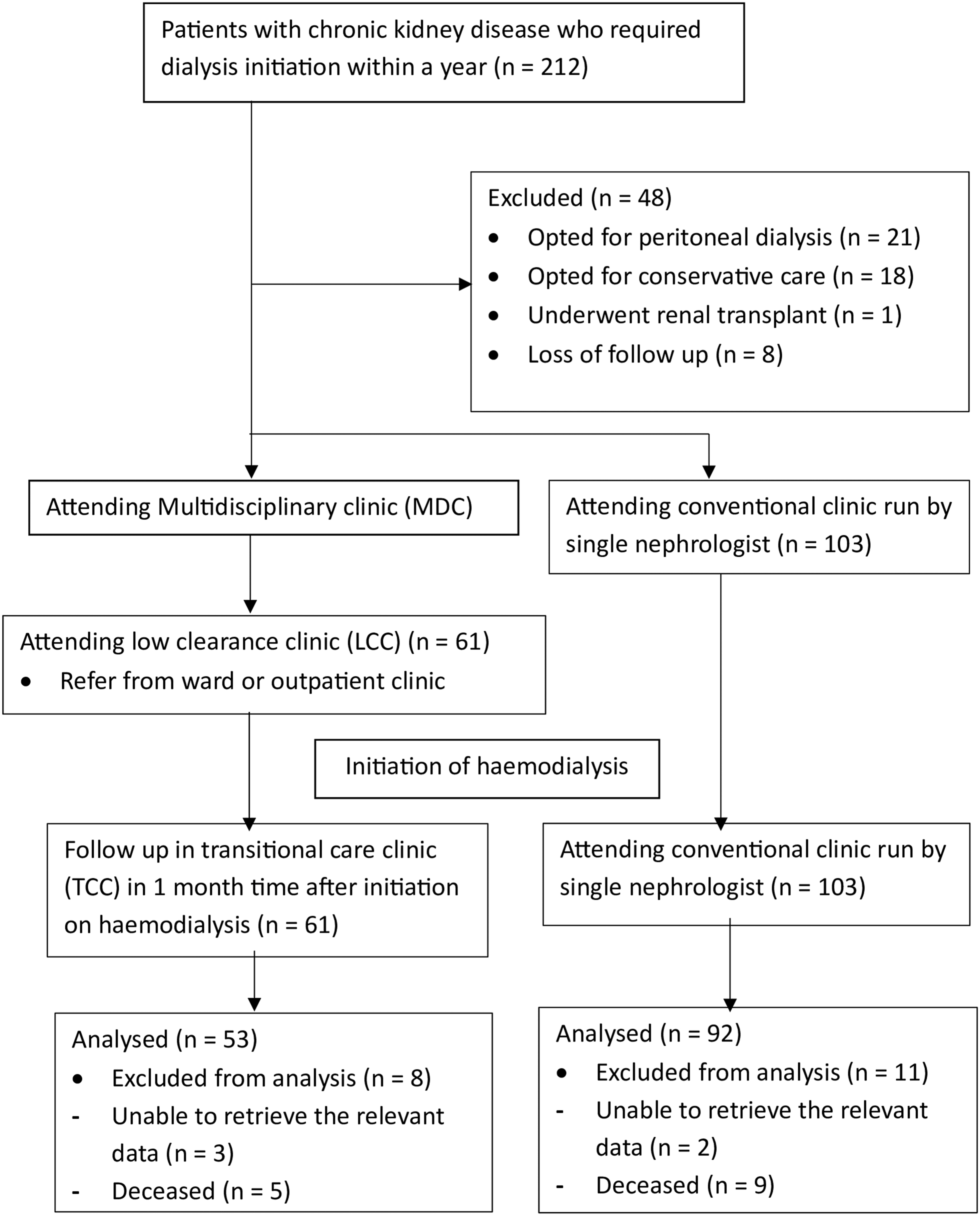
Baseline demographics
Demographic of haemodialysis patients at dialysis initiation.

a: All values are presented as numbers (%) or mean ± standard deviation (SD).
b: MDC = multidisciplinary clinic.
The mean age at dialysis initiation was similar between MDC and conventional clinic patients, as were serum albumin levels, body mass index, and haemoglobin levels.
Primary outcomes of definitive dialysis access at 6 months post dialysis
Figure 2 illustrates the utilisation of definitive dialysis access at dialysis initiation and 6 months post-initiation. Initially, the use of definitive access, such as AVF or AVG, was similar between the two groups. However, at the 6-month follow-up, a higher proportion of patients in the MDC cohort achieved definitive vascular access compared to those receiving conventional care. Primary outcome on haemodialysis access.
A logistic regression model was used to conduct a multivariate analysis incorporating age, gender, ethnicity, comorbidities (diabetes, hypertension, obesity, cancer, ischaemic heart disease, primary renal disease), and laboratory parameters (haemoglobin, calcium, phosphate, albumin levels). The analysis indicated that the MDC intervention was a significant predictor of improved definitive dialysis access use within 6 months of dialysis initiation (OR = 2.44, 95% CI 1.16-5.26, p = .039), even after adjusting for the aforementioned factors. This OR indicates that patients in the MDC group were significantly more likely to transition to AVF/AVG within 6 months compared to those in the conventional group.
Secondary outcomes on catheter-related bloodstream infections (CRBSI), intensive care unit (ICU) admissions, and recurrent hospitalization
Figure 3 presents secondary outcomes, including rates of CRBSI, ICU admissions, and recurrent hospitalizations. The MDC group showed lower CRBSI rates (5.6%) compared to the conventional clinic group (14%), although this difference was not statistical significant (OR = 0.34, 95% CI 0.05–2.13, p = .709). Notably, patients in the MDC had significantly fewer ICU admissions (OR = 0.92, 95% CI 0.87–0.97, p = .026) and recurrent hospitalizations (OR = 0.13, 95% CI 0.04–0.49, p = .001). Secondary outcome at 12-months of follow up.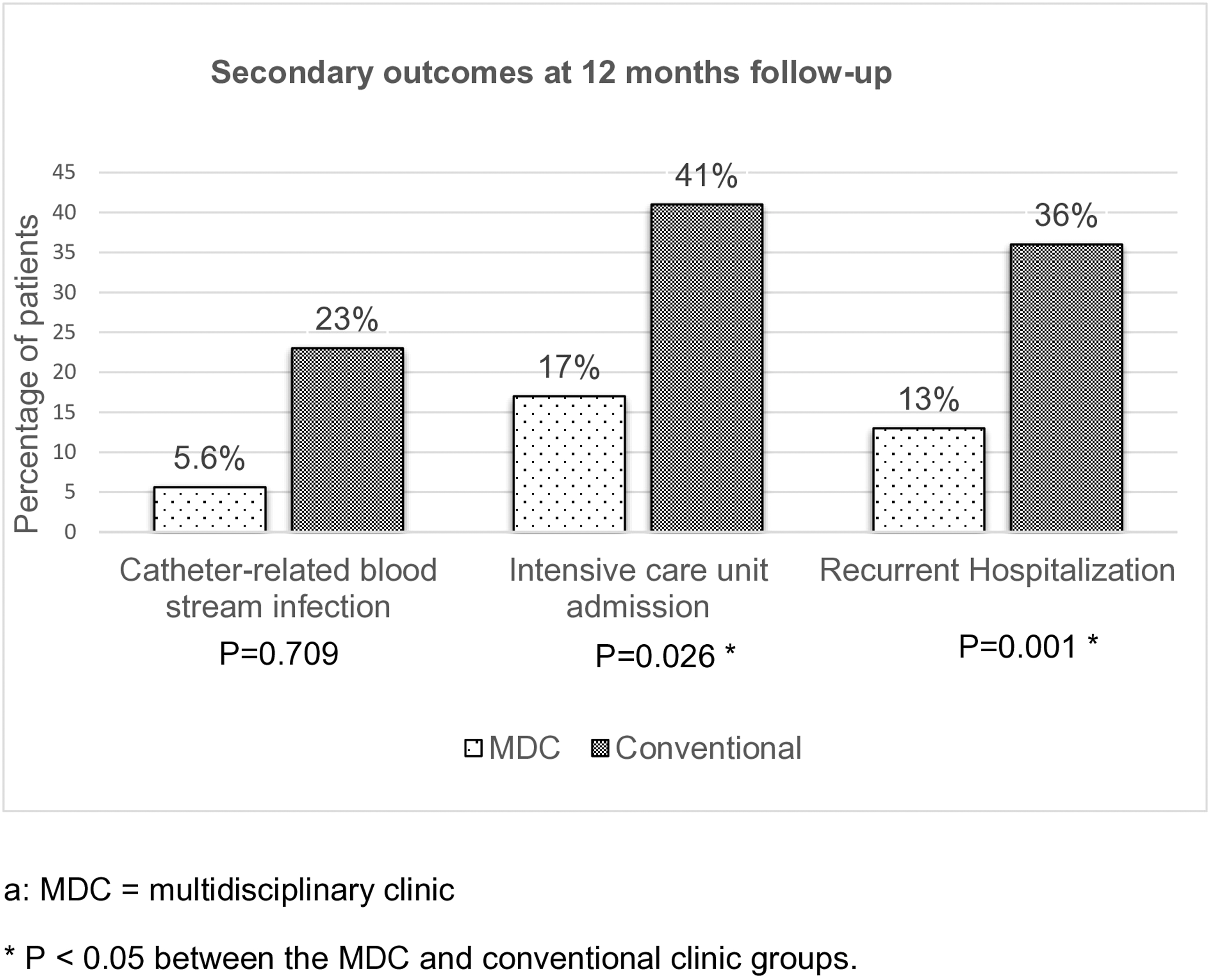
Discussion
Impact of MDC on haemodialysis patients
This study aimed to evaluate the impact of MDC on the use of definitive vascular access and other secondary clinical outcomes such as CRBSI, ICU admissions, and recurrent hospitalizations in haemodialysis patients. The objective was to determine if the MDC approach enhances the use of AVF or AVG and reduces catheter-related complications compared to conventional single-nephrologist care. Previous research has examined the effects of multidisciplinary clinics on mortality and morbidity in haemodialysis patients, focusing on either the initiation stage of dialysis or post-dialysis care.13,14 However, haemodialysis management is a continuous process, covering from pre-dialysis to post-dialysis phases. 15 This pilot study assessed the comprehensive care delivered by MDCs throughout the entire dialysis journey.
The MDC program was initiated 1 year before the start of haemodialysis in the low clearance clinic and extended through the transitional care clinic for up to one-month post-dialysis initiation. Patients choosing haemodialysis were monitored every 2–3 months before dialysis initiation and re-evaluated 1 month after starting treatment. A key focus was on the timely creation of definitive vascular access, such as AVF or AVG. In the low clearance clinic, patients are offered an educational program by the National Kidney Foundation called the “Know Right Start Right” program, which emphasizes the importance of establishing definitive dialysis access, such as AVF/AVG, for those opting for hemodialysis. 18 This approach emphasized the importance of establishing functional vascular access before starting haemodialysis, ensuring a smooth and structured transition to dialysis.
For patients who began haemodialysis without a definitive access, their vascular access status was assessed during follow-up in the transitional care clinic within 1 month of dialysis initiation. The renal coordinator provided additional education, and early referrals to vascular surgeons were arranged by nephrologists, typically within 4–6 weeks, to expedite the creation of definitive access. Our dedicated vascular team has established an agreement to proactively assess incident haemodialysis patients who are still using tunnelled dialysis catheters, ensuring that they receive an early review within 4–6 weeks for timely vascular access creation. This coordinated effort ensured that patients received timely and comprehensive care, ultimately promoting better vascular access outcomes.
In this study, the demographic and clinical characteristics suggest that the two patient groups were well-matched at baseline, indicating a balanced comparison for subsequent analyses. The annual mortality rate for ESKD patients in Singapore remains steady at 12%–14%, 12 with mortality often linked to catheter-related complications, 16 particularly among those requiring urgent haemodialysis initiation via catheters.7,8 The 2018 SONG-HD initiative highlighted the importance of vascular access in haemodialysis, alongside mortality and cardiovascular status. 17 Despite these guidelines, our hospital has struggled with establishing definitive dialysis access, with only 10% of patients initiating haemodialysis with such access. In contrast, the MDC group showed a significant improvement in the use of definitive vascular access after 6 months (51% vs 37%, p = .039). This improvement is attributed to the preparatory efforts of the MDC team, which facilitated better patient readiness for vascular access. Additionally, the MDC group had lower risks of ICU admission (3.7% vs 42%, p = .026) and recurrent hospitalization (13% vs 35%, p = .001), likely due to reduced catheter-related complications.
The lower, albeit non-significant, rate of catheter-related bloodstream infections (CRBSI) observed in the multidisciplinary clinics (MDC) group warrants further exploration. The lack of statistical significance may be primarily attributed to the small sample size, which likely limited the study’s power to detect meaningful differences. Additionally, variability in catheter usage duration among patients might have influenced the risk of CRBSI, as longer usage is typically associated with higher infection rates. Unmeasured confounders, such as adherence to infection control protocols and variations in catheter insertion techniques, could also have contributed to these outcomes. Furthermore, the retrospective nature of our study limits our ability to control for these potential confounders. Despite these limitations, our findings align with some published studies that report trends toward lower infection rates in multidisciplinary settings, highlighting the need for further research. 19 Future studies with larger cohorts, prospective designs, and standardized infection prevention strategies are essential to better understand the relationship between MDC interventions and CRBSI outcomes.
In the MDC model, nephrologists, renal coordinators, and medical social workers play crucial roles in delivering comprehensive care. Details of their specific contributions to patient care, particularly in the context of enhancing vascular access, are provided in Appendix Table 1. Nephrologists oversee patients’ renal function, monitor overall health, and manage complications related to ESKD and haemodialysis, with a particular focus on dialysis access.
Renal coordinators play a crucial role in ensuring continuous monitoring and seamless integration of the treatment plan, effectively addressing logistical and administrative matters. They also provide patient education on AVF/AVG procedures and postsurgical expectations, using visualization techniques to improve acceptance (Figure 4). Additionally, medical social workers offer vital psychosocial support, counselling, and assistance with social and financial challenges that could affect health and treatment adherence. This collaborative approach, which emphasizes early intervention, patient education, and comprehensive support, not only helps reduce complications and hospitalizations but also empowers patients to manage their condition more effectively, ultimately leading to improved overall outcomes. Educational material used by renal coordinator to educate patients on different vascular access for haemodialysis.
Study limitations and implications for clinical practice
The retrospective, single-centre design of this study introduces the potential for selection bias and confounding factors, and the small sample size with a brief 12-month follow-up period may further limit the generalizability and statistical power of the findings. Although efforts were made to minimize these biases by including all eligible patients during the study period, differences between the MDC and conventional clinic groups may still have influenced outcomes. For instance, the baseline demographics (age, gender, ethnicity, comorbidities) were carefully compared and found to be similar between the two groups, suggesting that selection bias was limited.
To address missing data, multiple imputation techniques were employed, which enhanced the robustness of the analysis. Sensitivity analyses, comparing the imputed dataset with complete case analyses, confirmed the consistency of the results, further strengthening the validity of our findings. However, unmeasured confounders such as patient adherence, socioeconomic status, and differing levels of engagement with healthcare services may still have affected the outcomes. Future prospective studies with larger sample sizes, longer follow-up periods, and multiple centres are recommended to further validate these findings and control for potential confounders.
Additionally, future research should incorporate a cost-benefit analysis to evaluate the economic implications of the MDC model. Despite these limitations, the study offers valuable insights into the effectiveness of multidisciplinary care in improving vascular access and patient outcomes. The education and preparation provided in the MDC are crucial for empowering haemodialysis patients, helping them mentally and physically prepare for dialysis initiation, and potentially enhancing their overall well-being during the post-dialysis period. This comprehensive multidisciplinary approach holds significant promise for improving dialysis access outcomes, as highlighted by the findings of this study.
Conclusion
In conclusion, this study demonstrates that the implementation MDC significantly improves the utilisation of definitive vascular access and reduces the rates of ICU admissions and recurrent hospitalizations in haemodialysis patients. The comprehensive and coordinated care provided by MDC, including early intervention, continuous monitoring, patient education, and holistic support, addresses the complexities of haemodialysis management more effectively than conventional single-nephrologist care. Despite the limitations of a retrospective, single-centre design and a small sample size, the positive trends observed suggest that MDC can enhance patient outcomes, emphasizing the need for broader adoption and further research to confirm these benefits in diverse settings.
Footnotes
Acknowledgments
We extend our gratitude to the dedicated team of nephrologists, renal coordinators, and medical social workers for their pivotal role in managing the multidisciplinary care services. We are also thankful to the study participants for their consent and to the renal coordinators for their efforts in data collection.
Authors’ contributions
Boon Cheok Lai conceived and coordinated the study, acquired and analysed the data, and reviewed the final manuscript, ensuring accountabilities for all aspects of the work. Pei Shan Lee participated in the design, coordination, and drafting of the manuscript, and reviewed the final manuscript, ensuring accountability for the work’s accuracy and integrity. Hui Boon Tay contributed to the design, data analysis, manuscript drafting, and final review, also ensuring accountability for the work’s accuracy and integrity.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.