
Abstract
This case series reports the integration of repetitive transcranial magnetic stimulation (rTMS) with conventional rehabilitation therapies in three early subacute ischemic stroke patients with upper limb motor impairment. In Malaysia, data on the combination of rTMS with intensive rehabilitation for stroke patients remains limited. The three patients with completely paretic upper limb, began therapy on post-stroke day 20, 16, and 15, respectively. They received rTMS sessions with inhibitory protocols targeting the contralesional primary motor area (M1) at 1 Hz, 5 days per week for 2 weeks (10 sessions). Each session included 1800 pulses at 120% resting motor threshold for 40 minutes, followed by 60 minutes of upper limb motor-function training. Outpatient occupational therapy was then continued for 3 months. All patients showed neurological and functional recovery as measured by the Medical Research Council scale and Fugl-Meyer Assessment-Upper Extremity Motor. The gains were observed immediately after the 10 rTMS sessions and persisted at 3 months post-stroke. Furthermore, all patients also achieved total independence in daily activities, with Modified Barthel Index scores of 99-100. No serious adverse events were reported. This case series suggests that combining rTMS with conventional rehabilitation therapies during the early subacute phase may enhance upper limb motor function recovery in stroke patients.
Introduction
Up to 75% of stroke survivors experience upper limbs (UL) dysfunction, affecting their ability to perform activities of daily living (ADL). 1 Given the complexity of the UL, conventional rehabilitation methods such as neurodevelopmental therapy, motor relearning and task-specific training provide limited improvement. Thus, current treatment focuses on therapeutic strategies that directly target brain functional restructuring to promote neuroplasticity, such as repetitive transcranial magnetic stimulation (rTMS). It is an off-label, non-invasive neuromodulation therapy, often utilized alongside conventional rehabilitation. However, evidence of rTMS effectiveness in subacute stroke remains limited, with 73% of studies focusing on chronic stroke patients.2,3
Although rTMS has been studied in Europe and parts of Asia, reports from Southeast Asia are scarce.4,5 There is no consensus on the optimal therapeutic protocol for applying rTMS to post-stroke patients in this region. In Malaysia, despite extensive rehabilitation services, 6 rTMS availability post-stroke is limited to a few private settings. Additionally, there is a lack of local data supporting the integration of rTMS with conventional rehabilitation therapies. Our centre is the first public hospital to provide rTMS service for post-stroke recovery in Malaysia. In this case series, we present the combined therapies (rTMS and conventional rehabilitation) in managing UL motor impairment during the subacute post-stroke phase. This highlights the potential for incorporating rTMS as a routine part of stroke rehabilitation in Malaysia.
Case report
Summary of patients’ and controls’ characteristics.

ACA: Anterior Cerebral Artery, MCA: Middle Cerebral Artery, rTMS: repetitive Transcranial Magnetic Stimulation.
aDuration from stroke to initiation of combined rTMS and conventional rehabilitation therapies.
bDuration from stroke to initiation of inpatient conventional rehabilitation therapies.
cMissing data as the control six defaulted follow-up.
They received intensive inpatient rehabilitation and combined therapies were initiated on post-stroke day 20, 16, and 15, respectively. A total of 10 rTMS sessions with inhibitory protocols of 5 days/week over a 2-week period were chosen based on the interhemispheric imbalance theory post-stroke 7 and the consensus among the rTMS providers in the centre. Stimulation was delivered using a figure-8 coil connected to a Magstim Rapid stimulator, targeting the contralesional primary motor area (M1) at a low-frequency of 1 Hz.
The M1 was located using the 10-20 EEG system, with the motor hotspot identification and resting motor threshold (RMT) value determination based on the method outlined by Rossini et. al. 7 Each session comprised 1800 pulses at 120% RMT, divided into 40 pulse trains. Each train lasted 45 seconds with a 15-second intertrain interval, resulting in the total duration of 40 minutes. The treatment coil was secured at the initial stimulation target on the patient’s scalp with a specialized coil-stand holder and regular checks by the technician. A neck pillow was used to minimize head movement throughout the procedure.
Conventional rehabilitation therapy was provided immediately following rTMS, including 60 minutes of goal-directed UL motor-function training. The therapy was personalized to each patient’s UL impairments accordingly. It incorporated purposeful activities with sufficient repetition and intensity, while gradually increasing difficulty and applying task-specific training that focused on skilled movements to enhance UL motor recovery.
Upon discharge, patients were given personalized home-based exercise instructions aligned with their functional status. These included 5-10 minutes of flexibility and range of motion exercises, performed two to three times a day, as well as 45-60 minutes of UL dexterity and strengthening exercises with task-specific training daily. All patients continued outpatient occupational therapy for 3 months. As they progressed, the complexity of the training was increased, and the goals were adjusted accordingly. Outcomes were measured at baseline, after 10 combined therapy sessions, 1- and 3-month post-treatment.
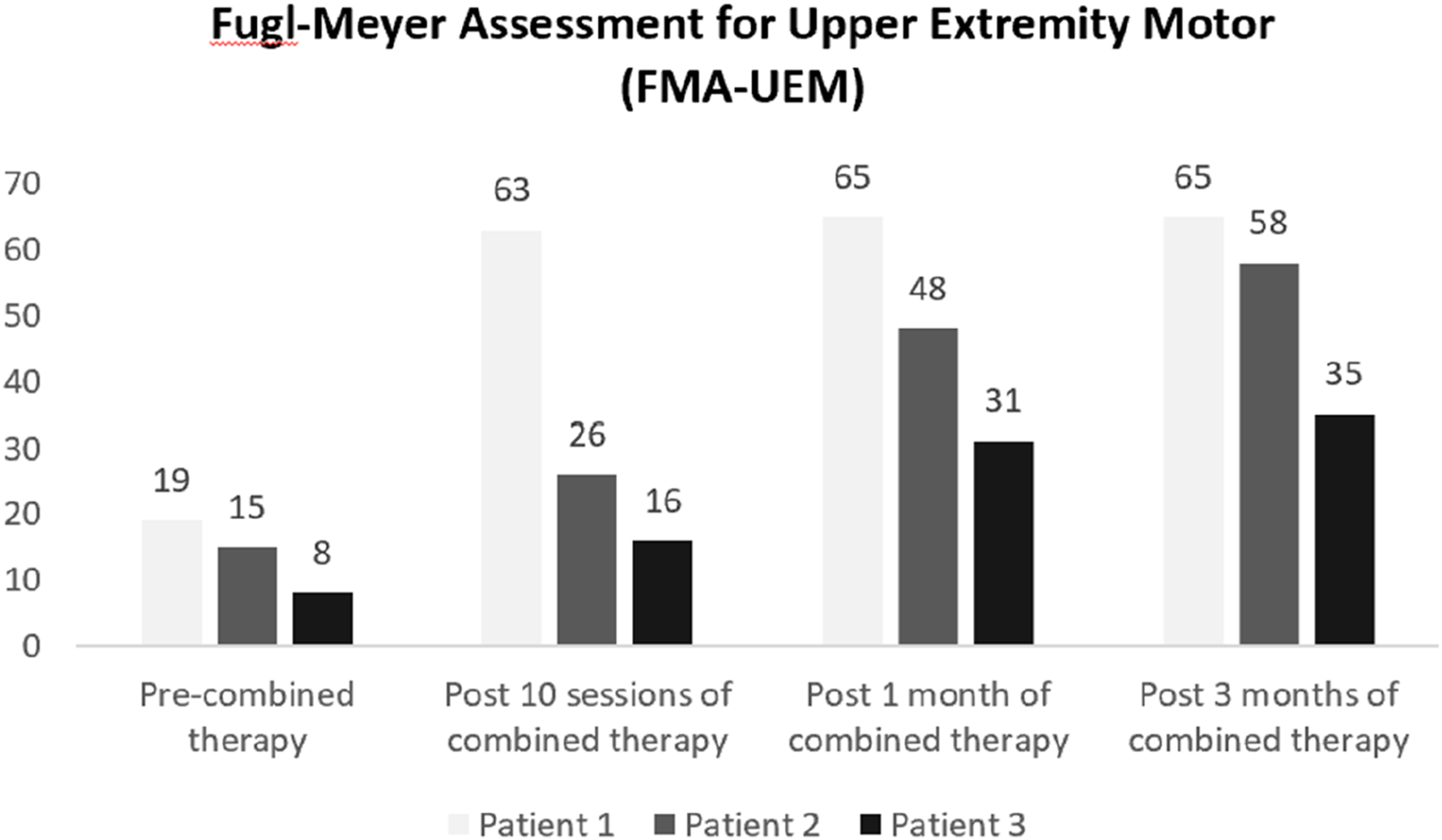
Significant improvements were observed in the MRC (Figure 1) and the Fugl-Meyer Assessment-Upper Extremity Motor (FMA-UEM) scores (Figure 2) for all patients. The initial gains were noted between the 3rd and 5th sessions, with continued enhancement through 3 months post-stroke. Patients one and two showed notable UL functional improvements, leading to significant gains. All patients achieved full independence in ADL with Modified Barthel Index score of 99 or 100. No major adverse events such as seizure, severe headache or dizziness were reported. Compliance with both rTMS and conventional rehabilitation therapies was high, likely due to the visible early improvements in UL strength and function, which helped boost patients’ motivation. Patient’s MRC scores according to different joint actions. Fugl-Meyer Assessment for upper extremity Motor (FMA-UEM) showed continuous improvement with a favourable trend observed at 3-month. (Maximum points of FMA-UEM in the upper limb is 66 points).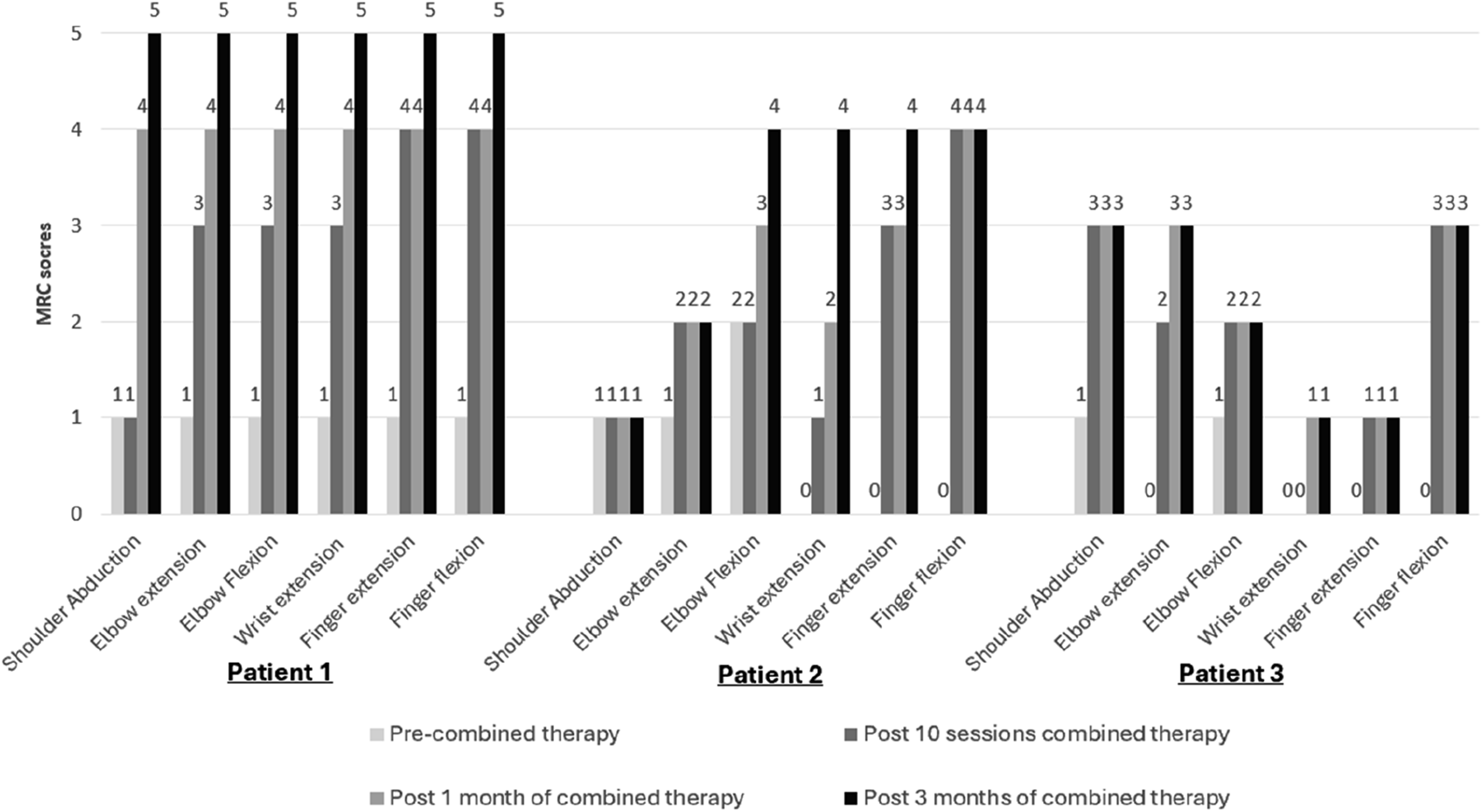
To address the absence of a control group, we analysed existing data from six patients who received intensive inpatient conventional rehabilitation therapy without rTMS during the same period. These patients either declined rTMS due to financial constraints or requested early discharge for personal reasons. All six patients met the eligibility criteria for rTMS. At 3 months post-stroke, four out of the six patients had UL MRC scores of 0-2 and an average FMA-UEM score of 32, both of which were significantly lower compared to the three patients who received rTMS alongside conventional rehabilitation therapy.
Discussion
The importance of post-stroke rehabilitation is to explore alternative methods to enhance motor function recovery. According to the ‘proportional recovery rule’, around 70% of the maximum potential recovery in UL impairments occurs proportionally within the first 6 months post-stroke, irrespective of the initial impairment levels. 8 However, this recovery depends on the integrity of the ipsilesional corticomotor tract. Not all patients follow this proportional pattern. A subset of individuals (non-fitters) experience poor recovery, likely due to the limited self-repair capabilities of damaged neurons. 9
These variations in recovery outcomes may be explained by disruptions in the neural balance between the affected and unaffected hemispheres. Stroke may affect the balance of transcallosal inhibitory pathways between affected and unaffected hemispheres. Studies have indicated that patients often exhibit increased inhibition in the ipsilesional hemisphere, and heightened excitability in the contralesional hemisphere.2,10 Therefore, modulating interhemispheric inhibition is recognized as a therapeutic strategy for post-stroke recovery.
In this case series, the low frequency inhibitory protocol was applied over the contralesional M1 in all three patients. The approach is typically chosen in early subacute stroke rehabilitation to suppress excessive excitability in the contralesional M1, normalize interhemispheric imbalance, and restore function in the paralyzed limbs of stroke patients.3,11 We opted not to use high-frequency rTMS on the affected hemisphere in our patients to avoid potential overstimulation. Excessive stimulation could disrupt the recovery process by increasing neuronal firing and exacerbating neuroinflammation. Inhibitory stimulation of the contralesional M1 appeared to be a safer approach, indirectly modulating the affected hemisphere with a relatively low risk of inducing adverse events.12,13
Our findings suggest that both rTMS and rehabilitation therapy can be safely applied in early subacute ischemic stroke patients. All three patients received rTMS within the first 3 weeks post-stroke, without significant adverse effects observed. In our practice, rTMS is generally avoided within the first 7 days post-stroke. Most patients are still experiencing medical instability (e.g., uncontrolled hypertension) and have not yet transferred to the rehabilitation ward. The treatment duration per session was also increased to 40 minutes by extending the intertrain interval. This adjustment aimed to reduce the likelihood of major adverse event, such as seizures, or side effects, including scalp discomfort, headaches, and dizziness.
We could not confirm that the observed improvements were solely attributable to rTMS because of the absence of a control group. To address this, we compared data from patients in our ward who received intensive conventional therapy without rTMS. The findings suggest that rTMS, combined with conventional rehabilitation, may have significantly contributed to UL motor recovery. Further controlled studies are needed to isolate the specific effects of rTMS and validate its efficacy.
In Malaysia, rTMS remains relatively limited as a treatment for stroke rehabilitation. The reasons include the limited availability of rTMS facilities in public healthcare settings, the high cost of treatment (USD 450 for 10 sessions in public settings) and a lack of awareness among healthcare professionals or the public regarding its potential for stroke recovery. Rehabilitation physicians are the primary specialists for stroke rehabilitation in Malaysia, yet fewer than 10 (approximately 3%) have received formal training and credentials to perform rTMS. Our centre is the first public hospital in the country approved to offer structured rTMS treatment post-stroke. A nationwide survey would be valuable to identify the facilitators and barriers to incorporating rTMS into stroke rehabilitation therapy in Malaysia.
This case series has a few limitations. We did not measure the latency and amplitude of motor evoked potentials on both the ipsilesional and contralesional sides for all patients. Additionally, factors such as corticomotor tract damage, stroke lesion size, and location could be significant confounders. The absence of a control group limits our ability to definitively demonstrate the added benefit of combining rTMS with conventional rehabilitation therapy. However, comparisons with existing patient data suggest that rTMS may have contributed to the observed UL motor recovery.
Conclusion
Combining rTMS and conventional rehabilitation therapy during the subacute post-stroke period shows potential for enhancing UL motor function recovery, with benefits persisting at 3 months with continued conventional rehabilitation therapy. To better quantify the impact of this combination therapy, larger-scale studies involving diverse ischemic stroke patients are recommended in Malaysia.
Footnotes
Acknowledgements
We would like to thank Nur Hanis Jaffar for performing outcome measurements for patients in this case report. This submission has not been published anywhere previously and it is not being considered for any other publication.
Author contributions
MYP conducted the literature review and drafted the initial manuscript. All authors were involved in patient recruitment. MM provided critical input and supervised the manuscript. All authors reviewed and approved the final version.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.