
Abstract
Background
Simulation training, an important component of the Emergency Medicine (EM) training curriculum, was affected by the COVID-19 pandemic due to social distancing policies. As a result, there was a need to find alternative approaches to medical simulation that could facilitate effective teaching and practising of team resuscitation.
Objectives
This paper describes an alternative approach to face-to-face simulation teaching due to pandemic-related limitations.
Methods
We conducted a virtual simulation session for nine junior doctors (medical officers, emergency medicine residents, and internal medicine residents). The sessions were carried out through video conferencing and medical simulation software. The session included pre-class readings, prior briefing on what to expect during the simulation case scenario, running of three case scenarios, team debriefing, and post-class feedback of the session conducted via Google Forms.
Results
Student feedback was obtained via a post-class survey. Feedback was largely positive as most participants found the session interactive and the pre-specified outcomes during the pre-simulation brief were achieved. Most participants also felt that fully online simulation training was an effective alternative to face-to-face simulation training.
Conclusions
A virtual simulation method is a feasible alternative to face-to-face simulation amidst the COVID-19 pandemic. We hope to increase awareness of this mode of teaching in the broader medical education community to benefit more learners.
Introduction
Simulation training has been an integral part of the Emergency Medicine (EM) training curriculum in the past decade. It allows the realistic set-up of the patient care experience setting, allowing participants to practise a range of skills, diagnose and manage both common and rare diseases, and improve skills such as teamwork and communication in a safe environment.1,2
This curriculum comprises various simulation modalities such as the use of simulated patients, part-task trainers, high-fidelity manikins, and computer-based simulation training. 3 One core skill that simulation training has proven useful would be the development of team resuscitation skills which requires a combination of individual knowledge, skill and decision-making plus team communication and collaboration.
Traditionally, team resuscitation simulations have been conducted in person, using low or high-fidelity mannequins. Unfortunately, these methods of teaching were unsuitable due to social distancing and team segregation measures during the COVID-19 pandemic. Due to the risk of the spread of the virus, the closure of simulation centres and cancellation of in situ simulation sessions were necessary to ensure that interactions between staff and patients were kept to a minimum. 4 As a result, there was a need to find alternative approaches to medical simulation that could facilitate effective teaching and practising of team resuscitation.
We describe one such approach, with realistic teaching of team resuscitation done purely through an online method during the COVID-19 pandemic.
Methods
Period
The simulation was carried out in October 2021, during strict movement control orders due to the COVID-19 pandemic.
Learners
It involved a total of nine learners, including junior medical officers, emergency medicine residents, and internal medicine residents. They had varying levels of experience with team resuscitation and most had undergone face-to-face simulation training before in the course of their medical education.
Facilitators
It involved a total of four facilitators and a session coordinator, who were specialist emergency physicians with prior experience in teaching face-to-face simulation.
Software
The entire session was carried out primarily through the Video-Conferencing Software (VCS) Zoom (Zoom Video Communications, Inc.), with the facilitators additionally using Presentation Software (PS) Microsoft PowerPoint (Microsoft Corporation), Simulation Software (SS) Med Sim Studio (by Adam D. Blumenberg, MD) and Voice-Changing Software (VO) MorphVOX Jr. (Screaming Bee Inc).
Pre-simulation readings and brief
A week before the session, the learners were given reading materials about the scenarios they would be going through.
Before the start of the simulations, they were briefed as a group by the facilitators using the PS on the VCS.
This briefing covered the following: 1) Overall learning objectives and expected observed outcomes Structured approach to crisis management in the ED Closed Loop communication and readback Leadership and delegation of roles in a crisis. 2) Flow of the session Duration of each scenario (20 min) and follow-up debrief session (25 min) within the same room 3) Explanation of the roles the learners were supposed to play in each scenario. Senior Doctor, Junior Doctor, Nurse 4) Examples of how they were expected to communicate to the patient and one another for example “Sister Tan, please get a set of vital signs from the patient”, “Dr Koh, I note that the patient’s White blood count is high, should we start antibiotics?” 5) Need for confidentiality and non-disclosure of contents of the session to non-participants All the participants agreed on the above.
Simulation flow
The learners were then divided into groups of three and each group was sent to their pre-assigned breakout rooms (three in total) by the session co-ordinator using the VCS (Figure 1). Learners and facilitators were assigned to breakout rooms using the VCS.
Each breakout room had a facilitator who would guide the participants through a simulated clinical scenario lasting 25 min. Following the scenario, the facilitator in the same breakout room would conduct a debrief of the case over the next 20 min.
After each session, the learners remained in their respective breakout rooms while the facilitators rotated to the next room to run their scenarios. This process repeated until every group of learners had gone through all the cases.
Pre-scenario preparation
Before the session, the scenarios and instructions were transcribed into slides using the PS, which was installed along with the VCS, SS and VO on the computer desktops of the facilitators. Additional images (e.g. ECG and Radiographs), apart from what was already in the database of the SS, were also uploaded to a shared online folder accessible to the facilitators. This allowed them to conveniently download the images into the SS for display during the scenario. A list of the roles of the participants (Senior Doctor, Junior Doctor and Nurse) was also pre-populated.
Running of scenario
At the start of each scenario, upon entering each room, the respective facilitators assigned the learners their roles based on the pre-populated list. They were informed to rename themselves in the VCS to reflect their role. (Figure 2) They were also instructed to switch on their microphones and cameras. Learners were instructed to rename themselves in the VCS to reflect their role in the simulation.
During the scenario, the facilitator simultaneously role-played as the patient and the facilitator using separate VCS accounts on his/her phone and computer desktop. Input to the “Vitals screen” (seen by participants) was programmed from the control panel of the SS hosted and shared from the computer desktop. The software allowed instant display of various investigations, including blood results, ECG, and static, and dynamic radiology images. These either came pre-built with the software or had been uploaded earlier into the software from the facilitators’ computer desktop folder (Figure 3). Real-time vital signs of the patients and investigation results were displayed on the VCS.
To increase realism, while role-playing the patient, the facilitator used a simulated profile name and picture and the VO to change his/her voice output to the VCS. Deliberate care was also taken during the scenario to minimize direct interaction between the session facilitator and the participants to ensure participants were focused on the simulated patient and their team members.
During the scenario, the learners were brought through various checkpoints. Each of these checkpoints was carefully sign-posted, in the form of “typed-out prompts” reflected on the screen using the SS. This function was also used to display corroborative history, physical examination findings, and results of investigations the learners requested (Figure 4). Real-time vital signs of the patients and physical examination findings were displayed on the VCS.
Post scenario debrief
After each scenario, a debrief was conducted by the room facilitator, who un-muted him/herself and showed his/her face using his phone’s VCS. He/she used the PEARLS Healthcare Debriefing Tool to guide his debrief about the domains of medical management, communication, leadership, and teamwork.
Scenario Content
The scenarios covered during the simulation were as follows: Scenario 1 – Patient with acute pulmonary oedema Scenario 2 – Patient with seizure from thyroid storm Scenario 3 – Patient with diabetic ketoacidosis
These scenarios were similar to those used previously during face-to-face simulation sessions. They were taken from a bank of scenarios involving common crisis situations in our ED. They involved interpreting information from provided history, vital signs, physical findings and investigation results. The patient’s conditions evolved during the scenarios (e.g. Patient one became more breathless, requiring intubation, Patient two had recurrent seizures and Patient three became more breathless and acidotic), allowing the facilitators to assess the learners’ abilities to respond. Procedural skills (e.g. CPR, intubation) and physical examination techniques of the learners were not tested during the scenarios. The difficulty levels of the scenarios were pegged to suit the learners.
Feedback
At the end of the session, semi-anonymised feedback from the participants and facilitators was obtained using a structured form.
Results
Participant feedback
All the participants provided feedback on the session in various domains.
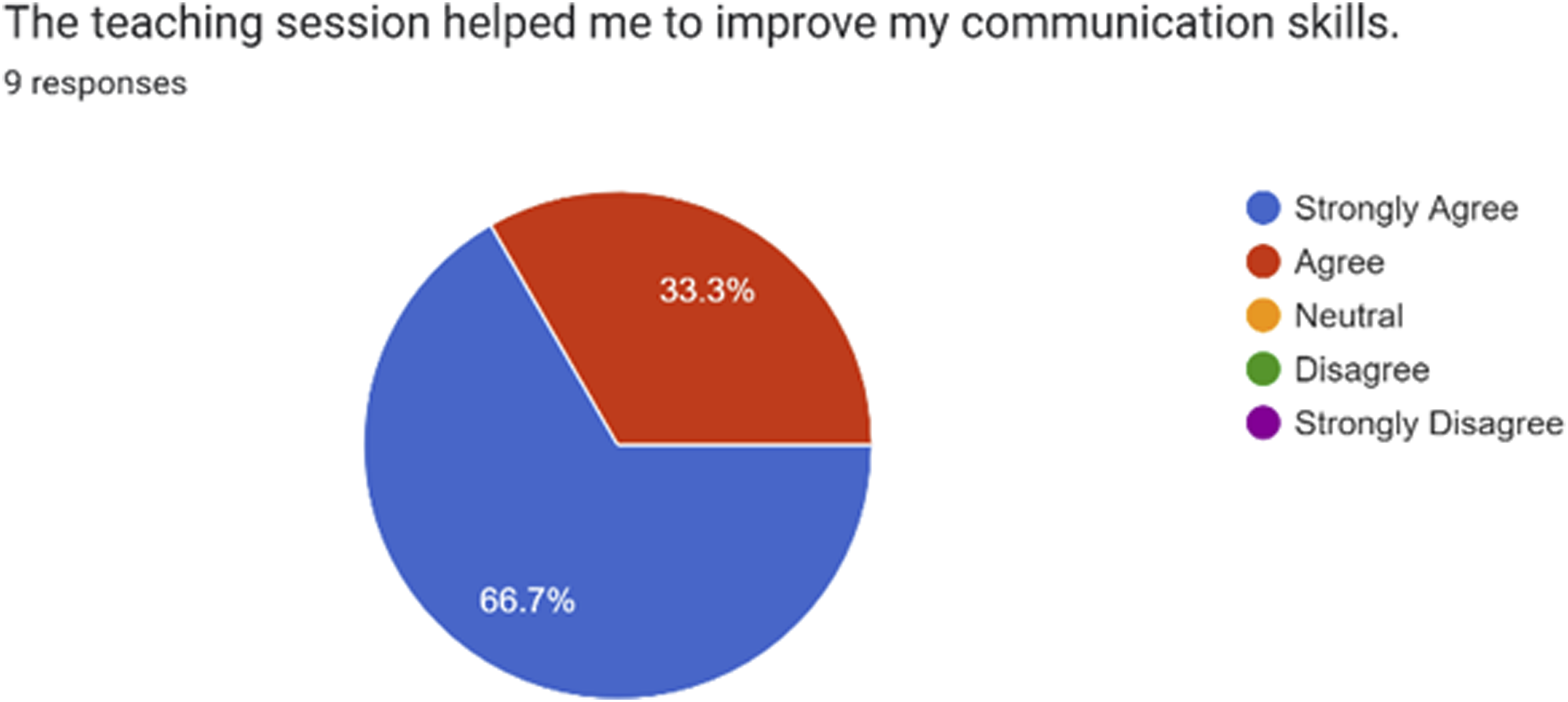
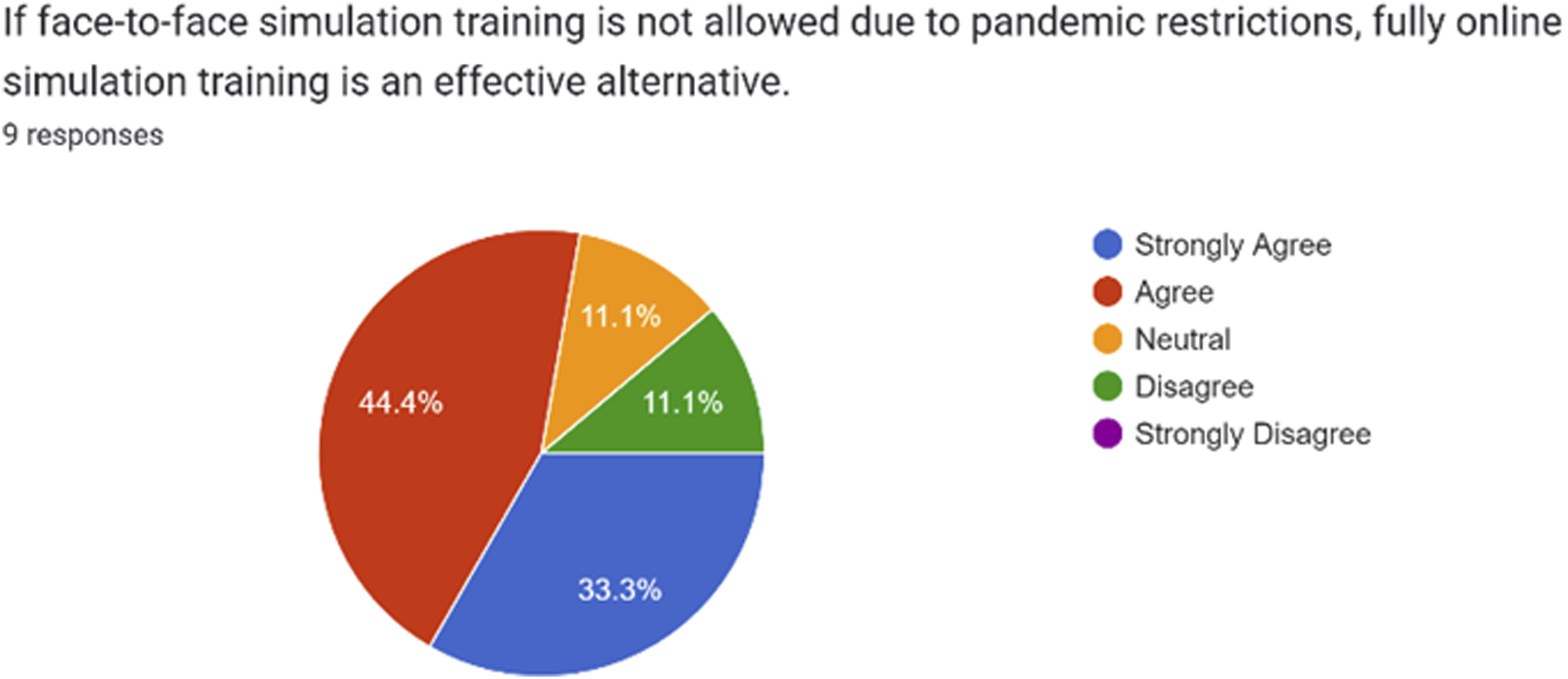
Overall, most participants found the session interactive and helped them improve their clinical decision-making and communication skills. They also agreed that it was conducted in a psychologically safe environment and that fully online simulation training was an effective alternative to face-to-face simulation training. (Figures 5, 6, 7, 8, 9 and 10). One anonymous participant disagreed with the statement that fully online simulation training was an effective alternative to face-to-face simulation training but did not elaborate further. Overall, the session achieved the outcomes that had been pre-specified during the pre-simulation brief. The participants felt that the teaching session was interactive and engaging. The participants felt that the teaching session helped them to improve their clinical decision making. The participants felt that the teaching session helped them to improve their communication skills. The participants felt that the teaching session was conducted in a psychologically safe environment. Majority of participants felt that fully online simulation training was an effective alternative to face-to-face simulation training. The participants rated the session as excellent and good.



Specific feedback obtained included the following: “awesome scenarios that were set. Very well run. Feels very much like a real simulation done face to face. Thank you very much for taking time off to do these for us” “zoom makes it difficult for multiple things to happen at the same time” “Concise and realistic scenarios”
Facilitator feedback
All the facilitators found the online simulation sessions to be realistic and effective in teaching medical decision-making and communication. They all agreed that the participants had achieved the pre-specified outcomes (structured approach to crisis management, closed loop communication, readback, leadership and delegation of roles), with all the groups exhibiting the above by the final scenario.
Challenges they faced included the amount of multi-tasking needed to role play as the patient, confederates, and toggle the settings of the
They agreed that fully online simulation training was a viable alternative to face-to-face simulation training, invaluable during a pandemic situation.
Discussion
Medical simulation remains a key component of the EM training curriculum and can be used to teach team dynamics, crisis resolution skills and communication skills among healthcare workers as well as with their patients and families. 5 One systematic review investigating its impact within EM and Critical Care showed overall benefit to the team’s knowledge and attitudes towards non-technical skills. 6 Carefully designed and implemented Simulation-Based Training has also been shown to improve team effectiveness and performance. 7
Simulations may involve the use of standardised patients, task trainers, software-based simulation, mannequins and a virtual reality environment. 8 Computer-based simulation systems have been shown to reduce training costs, whilst helping students and residents better learn emergency medical treatment algorithms.9,10 Screen-based simulation in Paediatric EM is a form of simulation in which a clinical scenario with one or more patients is presented through a digital screen surface. This tests knowledge and data gathering, cognitive thinking, procedural skills, communication, teamwork, and interaction with patients and families for situations relevant to Paediatric EM. 11
Online computer-based simulations allow participation from different locations. 12 In addition, operational manpower, space, and equipment needed to conduct such an activity are reduced, compared to face-to-face simulation. More groups can thus be trained simultaneously, limited only by the number of faculty and number of trainees that can be off duty at the same time. At the same time, based on the feedback obtained from the learners and facilitators, it is just as effective and realistic as face-to-face simulation training. This is consistent with feedback from participants of other online simulation-based exercises in similar healthcare settings, who rated them to be adequately realistic, innovative and effective in teaching clinical concepts and soft skills.12–14
Importantly, such simulations allow participants to experience and manage complex situations replicating real-life scenarios in a controlled setting, helping to bridge the gap between theoretical knowledge and real-world application. They help participants develop competence in the areas of collaboration and non-technical skills.
Such simulations differ significantly from a traditional online tutorial with vital signs on display as they facilitate interactive engagement, with participants having to make decisions in real-time, and respond to changing patient conditions and vital signs. Participants also receive real-time feedback, allowing them to see the immediate consequences of their actions. Compared to online tutorials, which typically present information in a more controlled and linear fashion, such online simulations feature complex, evolving scenarios that mimic real-life situations. Most online tutorials are also focused on individual learning rather than team-based exercises.
Limitations of such online simulations include the inability to assess physical examination skills, non-verbal skills related to body language, as well as procedural skills. Removal of learning outcomes related to the above may be needed if pre-existing face-to-face scenarios are used. A certain amount of realism is lost as well, given the shortened time taken to run these compared to actual resuscitations, as well as the quick release of investigation results. Simulations may also be hampered by technical limitations such as poor Internet connection speed and reliability and require a certain amount of IT savviness and multitasking by the facilitators and participants.
Given the positive outcomes, our simulation team will strongly consider this modality of teaching to train our learners amidst future pandemics, where face-to-face simulations may be prohibited. Such online simulations may also be carried out to overcome limitations arising from physical space and logistical constraints during in-person simulations, even during non-pandemic situations. Ultimately, learners will benefit from undergoing both methods of simulation training as it would increase their exposure to more crisis scenarios. Together with other existing modalities of simulation teaching, this should be employed in the training curriculum as part to maximise the learning of EM teams involved. By publishing our experience in this article, we hope to increase awareness of this mode of teaching in the broader medical education community so that more learners may benefit.
Footnotes
Acknowledgements
The authors acknowledge Dr Ganti Sameera for her support in the execution of this online simulation. They also acknowledge the use of Commercial Video-Conferencing Software (VCS) Zoom, Presentation Software (PS) Microsoft PowerPoint, and Free to download Simulation Software (SS) Med Sim Studio and Voice-Changing Software (VO) MorphVOX Jr. during the online simulation session.
Author contributions
All the authors were involved in the running of the simulation and contributed to the writing of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Data availability statement
Data sharing is not applicable to this article as no datasets were generated or analysed during the current study.