
Abstract
Isolated duodenal variceal hemorrhage is rare and has a high mortality rate, but the diagnosis and treatment can be challenging. We describe a case in which endoscopic variceal injection was deemed too high risk and not feasible due to patient factors of rapid blood flow and an unstable scope position. Eventually, an interventional radiology (IR) based embolization technique, using a combination of coils and glue, was successful in achieving hemostasis. This case presents an alternative strategy for clinicians in managing duodenal variceal bleeding.
Keywords
Introduction
Isolated duodenal varices are an uncommon complication of portal hypertension, usually found together with gastroesophageal varices. 1 The most common location of occurrence is the duodenal bulb, with incidence decreasing distally. 2 Duodenal variceal hemorrhage has an incidence of only 0.4 – 1.0% but is accompanied by a disproportionately high mortality rate of up to 40%. 3 The diagnosis is difficult due to limitations of the endoscope in visualizing the distal end of the duodenum, further hampered by duodenal varices often being found deeper in the submucosal or serosa layer. 4 A high index of suspicion is needed and computed tomography (CT) scans are often required for visualization of the vascular anatomy. 4 There are various therapeutic interventions and one of the more common approaches is that of endoscopic treatment due to its ready availability and less invasive nature. 5 Duodenal varices often arise from the main tributaries of the portal venous system i.e., superior mesenteric vein, portal vein and splenic vein draining into the inferior vena cava (IVC) through the veins of Retizus. 6 The heavy blood flow together with its location, presents technical challenges. 7
Case report
We describe a case of a 75-year-old female with no relevant past medical history presenting with massive upper gastrointestinal bleeding to the emergency department. On presentation, she was hypotensive, drowsy, with generalised mild abdominal discomfort. There was no elicited hepatic flap. She required urgent fluid resuscitation and blood transfusion. Early blood tests revealed a 5.5 g/dl drop in hemoglobin from 15 to 9.5. Platelet count was 192 × 109/L; albumin was 26 g/L, total bilirubin 23 umol/L, alkaline phosphatase 122 U/L, alanine transaminase 36 U/L, aspartate transaminase 45 U/L. Prothrombin Time was 11.9 and activated partial thromboplastin time was 26.9. In view of her obtundation and massive hematemesis, elective intubation was done to minimise aspiration risk. Endoscopy revealed large varices (Figure 1) in the third part of the duodenum (D3), with stigmata of recent hemorrhage without any accompanying esophageal or gastric varices. The varices were not actively bleeding at the time of endoscopy and a decision was made not to attempt endoscopic variceal injection due to the unstable scope position in D3. An urgent computed tomography (CT) angiography was performed, demonstrating an irregular, nodular liver outline suggestive of cirrhosis. Prominent collateral vessels were seen along the para-aortic and para-caval regions, with some submucosal in location along the second and third portions of the duodenum. No active hemorrhage was noted in the scan. Somatostatin therapy was commenced but re-bleeding occurred 3 days later. Referral for interventional radiology (IR) guided embolization was made. Endoscopic view of duodenal varices in distal third of duodenum.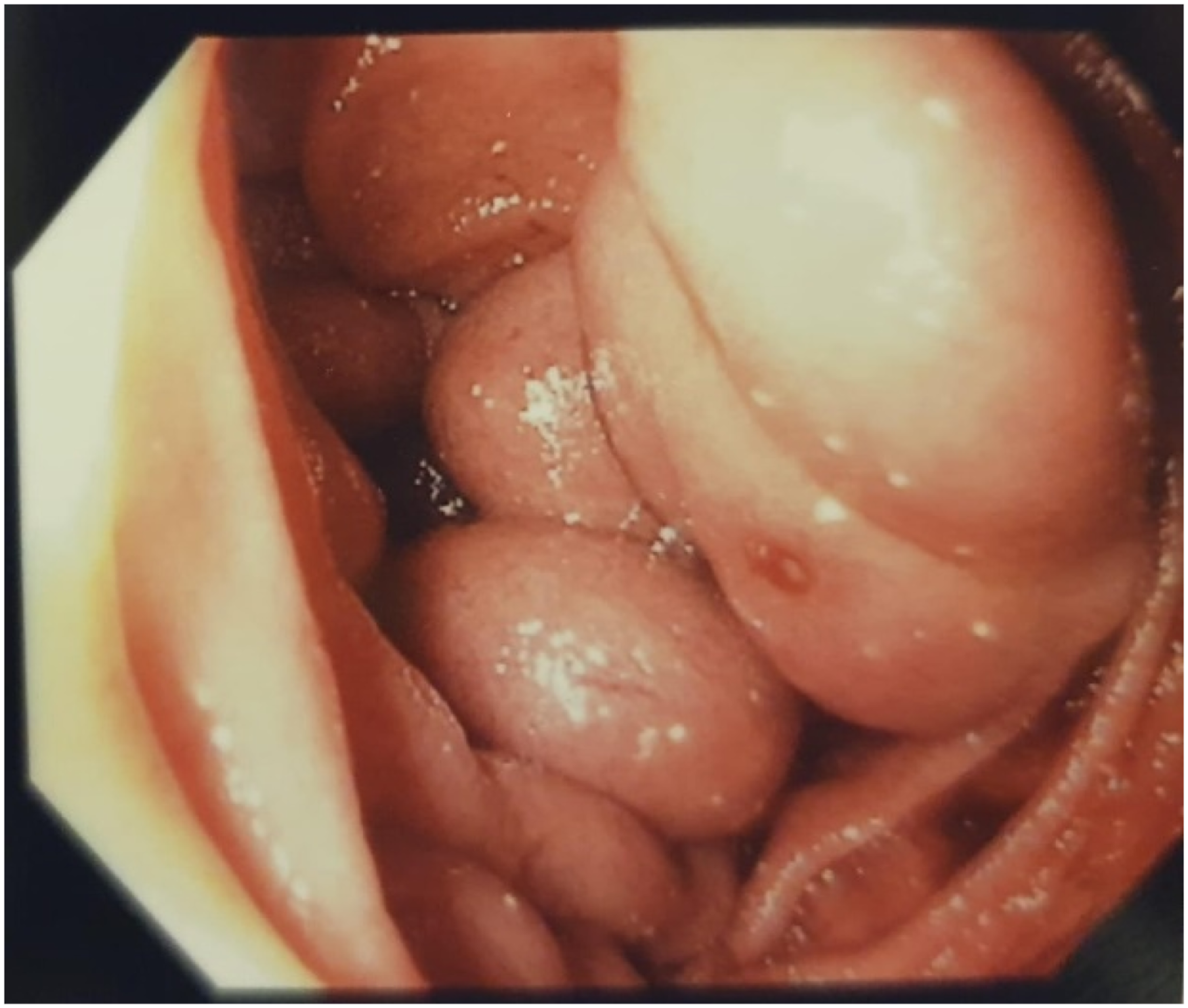
Transhepatic portal venography (Figure 2) revealed a tributary of the superior mesenteric vein as the culprit vessel. Proximal glue embolization was first attempted, but rapid flow impeded adherence to the venous wall. A microcatheter was inserted into the distal portion of the varix, allowing sandwich embolization with coils and glue. Post embolization angiogram showed complete obliteration of the varix (Figure 3). The patient was initiated on non-selective beta-blockers for secondary prophylaxis and discharged well with no further episodes of variceal bleeding at 6 months follow up. Transhepatic portal venography. Post embolization angiogram showing complete obliteration of the varices.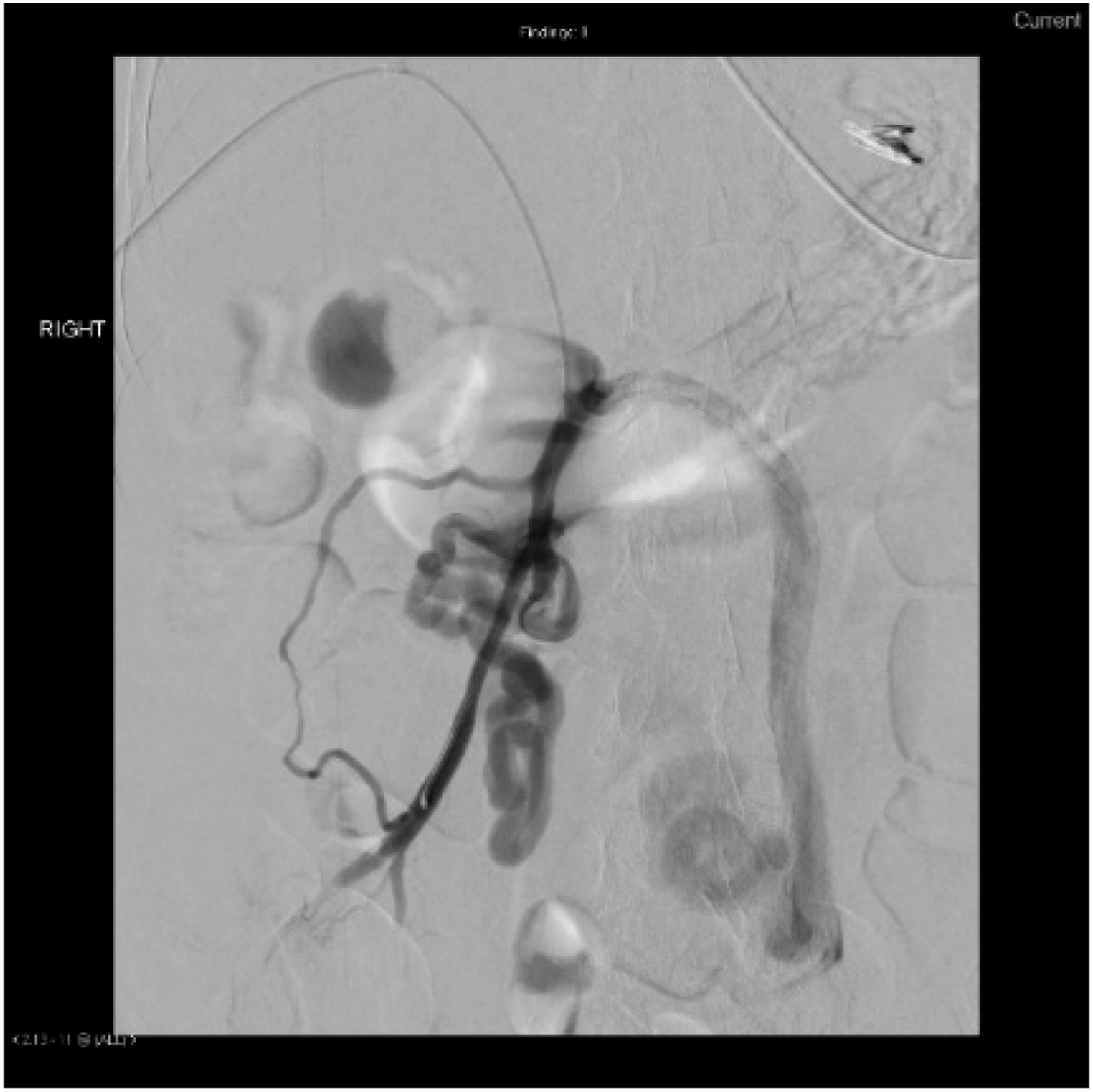

Discussion
Ectopic variceal bleed presents a therapeutic challenge. Due to its uncommon occurrence, there remains no standardized management guidelines. The patient in this report was initially considered for endoscopic variceal injection, before finally undergoing an IR guided embolization approach. In retrospect, it was fortuitous that endoscopic variceal injection was not attempted as the rapid venous flow would not only impede hemostasis, but also risk non-target systemic glue embolization to other sites. This case contributes to the existing literature an alternative IR based strategy for successful management of isolated duodenal varices.
Conclusion
Ectopic variceal bleeding is a life-threatening complication of liver cirrhosis that requires timely resuscitation and emergent endoscopic evaluation. Whilst esophageal variceal bleeding has the temporizing option of the Sengstaken – Blakemore tube, this option is not available in ectopic variceal bleeding. This case highlights the need for a multidisciplinary consultative management approach between gastroenterologists and interventional radiologists.
Footnotes
Author contributions
Tze Tong Tey and Gemaine Kar Mun Chan conceptualized the study and design. Yi Yuan Tan and Gemaine Kar Mun Chan drafted the paper. Rajneesh Kumar and Yi Yuan Tan analyzed and interpreted the data. Tze Tong Tey and Farah Gillan Irani were responsible for critical revision of the article for important intellectual content as well as final approval of the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Data availability statement
Data sharing is not applicable to this article as no datasets were generated or analysed during the current study.