
Abstract
Background
While the impact of COVID-19 on health care seeking behaviour has been well documented in adult studies, little is known about the impact of COVID-19 on ambulatory paediatric care in South East Asia.
Objective
To analyse the impact of early COVID-19 events on weekly clinic attendance volumes and default rates in the ambulatory paediatric service of a large tertiary teaching hospital in Singapore.
Methods
We used independent t tests to compare the weekly aggregate clinic attendance and default rates of the different time periods of the early COVID-19 pandemic (early COVID-19, movement controls, release of movement controls).
Results
The total weekly clinic attendance decreased significantly and default rates increased significantly during the early COVID-19 period prior to the implementation of movement controls. During the period of movement controls, the first visit default rate remained significantly increased despite the postponement of all non-essential first visits. Post movement controls, both the first and follow up visits rebounded to pre-COVID 19 levels. The default rate for follow up visits was significantly lower than baseline in the post movement control period.
Conclusions
Decreased utilization of ambulatory paediatric care in Singapore in a pandemic has implications for future pandemic preparedness including both health care resource allocation and health communication.
Introduction
Understanding the impact of the early COVID-19 pandemic on ambulatory paediatric clinic attendance provides valuable information for paediatric health care resource planning for future pandemic preparedness.
Research described decreased utilization of non-COVID-19 paediatric healthcare during the COVID-19 pandemic across health care settings including paediatric emergency room care,1–4 paediatric inpatient care3,5 and paediatric ambulatory care,6–10 including immunization services.11–13 Conversely, usage of teleconsultations increased in paediatrics.6,7,9 This mirrors the findings of other specialities, where the use of non-COVID 19 related health care declined and negatively impacted health outcomes.5,14–19 Similar patterns of decreased health care utilization during epidemics have previously been noted during the SARS and MERS outbreaks in Asia.20–23
The reasons for decreased health care utilization during epidemics are multifactorial. Health system factors can contribute to decreased utilization through reallocation of health care resources to meet pandemic-related health care needs, decreased available healthcare workforce, supply chain disruptions, and governmental movement restrictions. 24 Patterns of disease may change; the COVID-19 public health measures led to decreased accidental injury and communicable diseases.3,25,26 Individual-level decision making also may contribute to decreased health care utilization during a pandemic independent of health system factors as individuals balance their perceived need for seeking health care against the perceived risk of the outbreak-related infection.22,23,27
To the best of our knowledge, research examining the impact of COVID-19 on general paediatric ambulatory care has not been described in Southeast Asia. The early phase of the pandemic in Singapore provides an unique opportunity to examine changes to healthcare utilization prior to the significant influence of health-system factors and the implementation of nonessential movement controls. Furthermore, while changes in clinic visit volume may reflect the influence of both health care system factors as well as individual choice regarding care seeking, the examination of default rates can provide insight into individuals’ health care decision making as the visit was available and unaffected by health system factors. Thus, we describe the associations between COVID-19 events in Singapore on the clinic visit volume and non-attendance (default) rates in the ambulatory paediatric service of a large tertiary teaching paediatric hospital.
Methods
Setting
Singapore and COVID-19
Key elements of Singapore’s early response to COVID-19 included containment measures, financial support for COVID-19 health care costs, and transparent communication with the public. 28 Singapore utilized a disease outbreak response system condition (DORSCON) framework as a tool for pandemic planning and communication with the public regarding the level of public health risk. 29 The framework consists of four color-coded levels (green, yellow, orange, and red) of escalating public health risk.
The ambulatory paediatric service
Our hospital is an 830-bed tertiary government hospital which provides two-thirds of the public paediatric health care in Singapore. The hospital was designated as a paediatric treatment site for paediatric patients with COVID-19.
The Ambulatory Paediatrics Service provides health care to children less than 18 years of age and accepts referrals from the primary care system and emergency medicine department. The clinic provides consultations and follow-up care for common childhood conditions such as asthma, growth and developmental concerns, abdominal pain, and headaches. These clinics do not routinely provide regular childhood immunizations.
COVID-19 timeline and ambulatory paediatric changes
Early COVID-19 period: DORSCON yellow and orange
On January 23, 2020, Singapore identified the first case of COVID-19 in Singapore and escalated the DORSCON level to yellow. The Department of Paediatric Medicine initiated symptom and travel history screening measures in the ambulatory setting with rescheduling of patients with risk factors if required.
With increasing disease prevalence, Singapore escalated its response to DORSCON orange on February 7, 2020. The hospital re-assigned physicians from the ambulatory service to create segregated care teams for COVID-19 care. From February 10 to 21, 2020, the ambulatory team actively rescheduled patients with non-urgent follow up appointments and remotely re-filled necessary medications. The team defined non-urgent cases as stable conditions where a delayed visit would not negatively impact health. Starting February 24, 2020, as patient self-cancellations and defaults had decreased clinic attendance, the ambulatory team discontinued this active rescheduling as the clinic could maintain appropriate staffing and social distancing without this intervention.
Early COVID-19: The 2020 “Circuit breaker”
Stricter movement controls, in the form of a lockdown or circuit breaker, were enacted from April 7 -June 1, 2020. During this period of strict movement controls, non-essential clinic visits were postponed or rescheduled. The lifting of the movement controls started on June 2, 2020 and the study period ended on September 26, 2020.
Data analysis
We obtained the weekly totals of scheduled, attended, and defaulted general paediatrics visits from January 5, 2020 through September 26, 2020 as well as a 3-month period from 2019 from a centralized appointment management system. The system categorizes visits into first visits which are the initial consultations for new medical conditions and follow up visits which are return visits for established conditions. We defined defaulted visits as scheduled visits that the patient did not attend but remained scheduled and calculated default rates by dividing the total number of defaulted visits by the total scheduled visits.
We compared attendance and default data with a timeline with dates of critical COVID-19 events (Figures 1 and 2) and correlated timeline dates with the dates of the weekly aggregated data. We identified January 5 through January 26, 2020, as the 2020 pre-COVID-19 period. Comparison between the 2020 pre-COVID 19 period and a 3-month historical baseline (January–March 2019) revealed no differences in the mean weekly clinic attendance and default rates, and thus we concluded that the 2020 pre-COVID 19 period was an accurate baseline of clinic activity. We defined the COVID-19 intervals as early COVID-19 (DORSCON Yellow and Orange: January 26–April 4, 2020), movement control period (April 5–May 31, 2020), and post movement controls (May 31–September 26, 2020). Each time interval was compared against the 2020 pre COVID period. Weekly patient volumes by type in 2020 with annotated COVID-19 related events in Singapore. Weekly ambulatory default rates by type in 2020 with annotated COVID-19 related events in Singapore.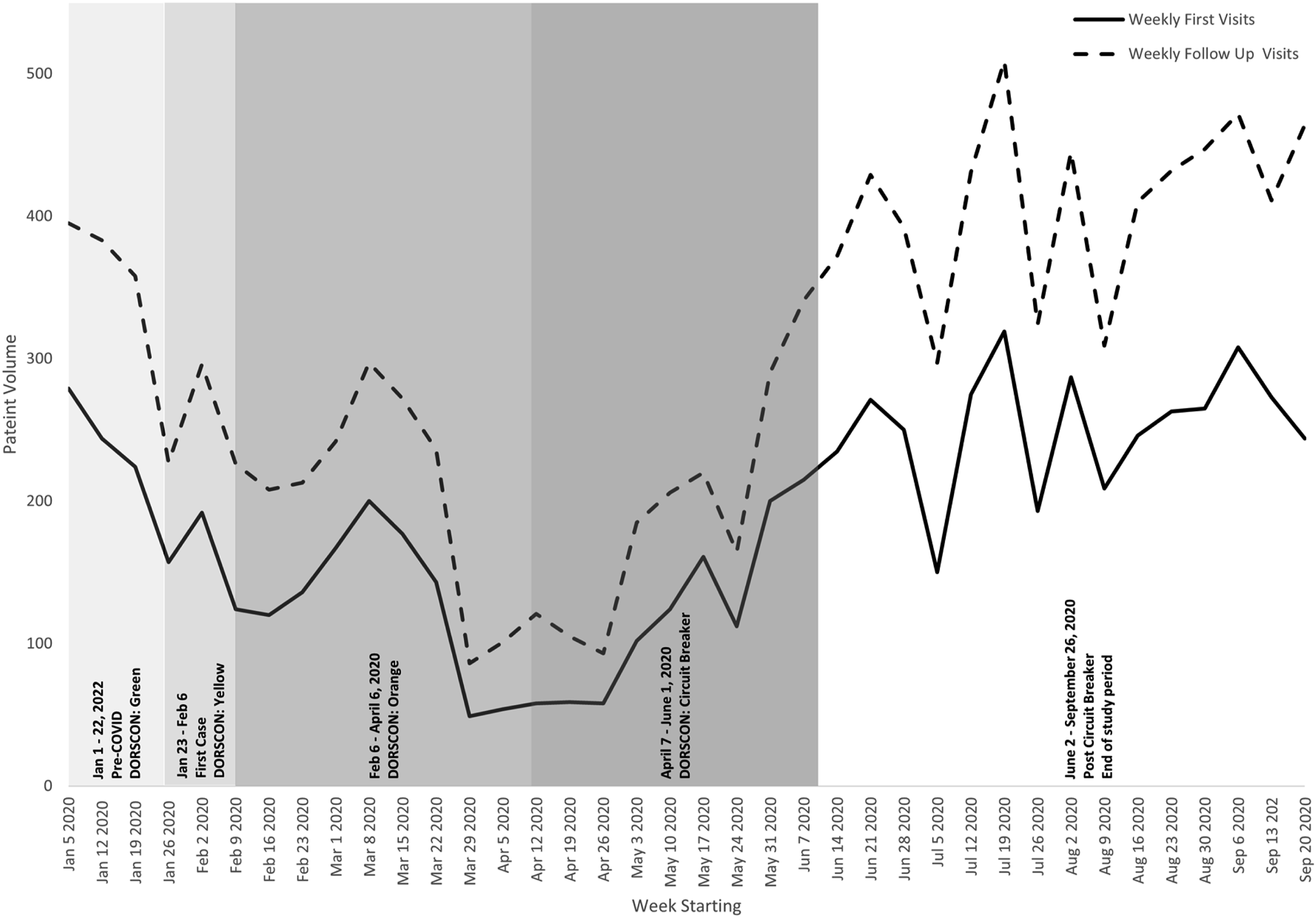

Independent t tests determined the difference in total, first visit, and follow up clinic attendance as well as default rates between the 2020 pre-COVID baseline and the different COVID-19 intervals. Further analysis evaluated for differences between the DORSCON yellow (January 26–February 8 2020) and DORSCON orange (February 9–April 4 2020) as well as examined the period of active rescheduling (February 10 to 21 2020) and the remaining portion of the early COVID-19 period.
Due to the weekly aggregated nature of the data, the dates defining the intervals for data analysis varied slightly from the historical dates defining these periods. We set the p value for significance a priori at 0.05. SPSS Version 19.0 was used for data analysis. The study was reviewed by the SingHealth IRB who determined the study did not require IRB approval due to the aggregate nature of the data.
Results
Impact of early COVID-19 events on default rates and mean weekly number of visits seen in the outpatient general paediatrics service in 2020.

*p < 0.05.
Further analysis of the DORSCON yellow and orange time periods revealed no statistical differences in total weekly volume of patient attendance (263.0 ± 46.7 vs 222.5 ± 62.7 p = .413) or total default rates (53.1 ± 1.9 vs 54.0 ± 5, p = .826) between the two periods. In addition, there was no significant changes in mean weekly volume of patient attendance (217 ± 12.7 vs 234.0 ± 67.3, p = .742) between the weeks with active physician-led rescheduling (February 10–21, 2020) and the remainder of the DORSCON yellow and orange COVID-19 period.
During the period of movement controls, the total volume of both first visits and follow up visits decreased significantly (First: 129.7 ± 12.1 vs 58.4 ± 17.1 p = .000; Follow up: 249 ± 27.8 vs 91.0 ± 39.9 p = .000) (Table 1). The first visit default rate was increased (First: 35.3 ± 7.8 vs 58.4 ± 17.1 p = .000) although there was no significant change in the follow up default rate from baseline (Table 1).
However, post movement controls, both the first and follow up visits rebounded to pre-COVID 19 levels (First: 129.7 ± 12.1 vs 151.3 ± 31.5 p = .264; Follow up: 382.0 ± 23.5 vs 398.5 ± 65.9, p = 0.678) (Table 1). The default rate for follow up visits was significantly lower than baseline in the post lockdown period (Follow up: 44.3 ± 2.5 vs 36.4 ± 4.5, p = .009) (Table 1).
Discussion
The findings of this study mirror other research that demonstrated decreased health care utilization during the COVID-19 period and provides information for future outbreak preparedness for paediatric populations.4,8,14,30,31 While the context of future pandemics may vary in terms of disease severity and governmental response, this study highlights the potential for significant decreases in ambulatory paediatric visits, the potential role for telemedicine, the need for post-pandemic service provision, and the importance of risk communication with families.
Although ambulatory paediatric services remained generally available during the early COVID-19 period in Singapore, the volume of visits was significantly lower than baseline and the default rates for both first visits and follow up visits increased significantly. This suggests families were not seeking ambulatory paediatric care although it was available. This mirrors findings from an adult study in Taiwan which found an early decrease in adult ambulatory care visits despite the ready availability of health care services and low cases of COVID-19. 23
During the early COVID-19 period, our total number of visits decreased by 39.6% and during the COVID-19 movement controls, our total number of visits decreased by 60.8%. This is similar to the decrease in paediatric outpatient visits reported from studies in other countries including Spain 9 (40-50%), South Korea 16 (37.5%), Germany 32 (35%), and Japan 33 (45%). Thus, during a pandemic, decreased clinical volume in ambulatory paediatric clinics is likely and thus health care workers and clinical space can be re-directed to meet the needs of pandemic-related medical care, as required.11,21 The magnitude of these decreases in clinic volume also highlights the role of telemedicine as an important tool in a pandemic setting to ensure timely paediatric care.6,9,34–37
While there was a significant decrease in clinic attendance and increase in default rates at the start of DORSCON yellow, there was no further significant changes after escalation to DORSCON orange. This contrasts with findings from a recent study looking at emergency room visits and hospitalizations in Singapore which showed a decrease in paediatric emergency room visits from DORSCON yellow to DORSCON orange while hospitalizations remained stable. 3 This may reflect that parents prioritized emergency paediatric care differently from ambulatory paediatric care during the early COVID-19 period likely due to differences in the acuity and severity of the presenting medical condition. This is consistent with other studies from the COVID-19 pandemic3,4,8 as well as previous epidemics.22,38 We speculate that given Singapore’s experience with previous outbreaks and location in Asia, that the population had an early awareness of COVID-19 which may have influenced these early decreases in clinic attendance. 28
During the period of movement controls, active postponement of non-essential visits contributed to the decrease in clinic visit volume. There was no increased default rates for follow up visits from baseline, likely due to a larger proportion of these visits being postponed and thus less opportunity for defaulting. Significantly, default rates for first visits remained statistically higher than baseline suggesting that parents remained reluctant to seek ambulatory paediatric care despite their case having been triaged as essential by the health care team. This reflects a risk that parents may be delaying or forgoing important medical care for their child especially around potential new diagnoses. This risk can be mitigated through communication strategies that highlight the importance and safety of obtaining needed healthcare as well as increased utilization of telemedicine.
In Singapore, while clinic volume returned to baseline after the movement controls, it is important to note that default rates for follow up were lower than the historical baseline. This suggests that parents who postponed care during the pandemic, returned to ambulatory paediatric care after the lifting of movement controls and an improvement of the pandemic conditions. Interestingly, while other countries saw rebound in non-COVID-19 ambulatory health care usage as COVID-19 conditions improved and movement controls were lifted, studies from other countries found a slower rate and smaller magnitude of this rebound effect, with many studies not showing a full return to their pre-pandemic baseline.9,23,32–34,39,40 This likely reflects differences in the country-specific COVID-19 situation at the time, health system resilience including service availability, as well as patient and family preferences. Health systems also must plan to meet these post-pandemic needs. 25
The study had several limitations. Due to the aggregate nature of the data, we are unable to analyse in further detail regarding the demographic or clinical characteristics of attended versus defaulted visits. Research in other countries has suggested that risk factors for decreased paediatric ambulatory care utilization included older age of the child,41,42 socio-economic factors, 43 and well child or chronic disease diagnoses as opposed to acute illness. 42 However, further evaluation of clinical and demographic factors is required in the Singapore context. Second, the measured default rates are likely an underestimation of the true cancellation or default rate as it does not take into account the visits that were pre-emptively cancelled by parents and thus not included in the measured default rates. Moreover, while we have attributed defaulted visits to delays in care, we are unable to assess if families shifted their paediatric care to a different site. We feel this is less likely given the post-movement control return to baseline paediatric volumes as well as paediatric health care landscape in Singapore. Finally, although our findings mirror the findings of many other health care utilization studies during the COVID-19 period, our study is only able to correlate changes in clinic attendance to COVID-19.
Nonetheless, our study has several strengths. We evaluated both clinic volume and default rates through multiple phases of the COVID-19 pandemic which provided complementary information regarding health care utilization. Secondly, Singapore is a unique case study as paediatric health care remained available in Singapore with only minimal disturbance during the early pandemic. Further research is needed to understand the patterns of paediatric health care utilization in pandemics across different settings, types of paediatric conditions, and patient demographics to aid in planning for paediatric care in the setting of future pandemics. Secondly, we need to better understand factors in parental decision making to inform interventions that accurately communicate the pandemic risks and reassure parents sufficiently to seek necessary care so as to minimize any impact on children’s health through unnecessary delays in needed care.1,24,28,44
Footnotes
Acknowledgments
The authors would like to acknowledge Dravid Koura for his help in creating the figures.
Author contributions
CD and RK researched literature and conceived the study. CD and RK were involved in protocol development and gaining ethical approval. CD completed data analysis. RK wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Data availability statement
The datasets generated and/or analysed during the current study are available from corresponding author.