
Abstract
Background
Emergency Department (ED) crowding is a global public health issue with low-acuity ED attendances (LAA) being widely identified as contributors to the issue. A primary care partnership programme, GPFirst, was developed to encourage low-acuity patients to visit their General Practitioners (GP) first, instead of the ED. We utilised a qualitative approach to gain an understanding of participants’ perceptions of GPFirst, their health-seeking behaviours, and explore recommendations for enhancing GPFirst.
Methods
A qualitative study design, underpinned by an interpretivist approach, was employed. Purposive sampling was used to recruit 12 GPFirst patients from a single tertiary care centre for semi-structured interviews. These interviews were analysed using Braun and Clarke’s reflexive thematic analysis.
Results
Participants’ age ranged from 25 to 63 years old. Four themes were identified. Firstly, “perceptions of GPs”, described the variations in participants’ perceptions about GPs. Secondly, “patients’ expectations of GPFirst”, noted the ED fee subsidy and prioritisation of ED care as key expectations of GPFirst. Thirdly, “facilitators and barriers to utilising GPFirst” highlighted the facilitators and barriers that influenced participants’ health-seeking behaviours and finally “recommendations for programme improvement” offered strategies for improvements.
Conclusion
This is the first qualitative study to examine participants’ perceptions of GPFirst. Recommendations may inform future programme redesign to optimise patient experience and facilitate programme uptake, contributing to overall efforts to reduce ED crowding locally. Future research may consider exploring GPFirst providers’ perspectives to elicit facilitators and barriers in implementation.
Introduction
Emergency department (ED) overcrowding is a global concern,1,2 straining resources and raising healthcare costs while compromising care quality, resulting in extended hospital stays.3,4 Low-acuity ED attendances (LAA) been identified as one of the contributors to ED overcrowding.3,4 The Patient Acuity Category Scale (PACS) designates patients as P1 for those requiring immediate attention, and P2 for acutely ill individuals with severe symptoms. In Singapore, 53% of ED visits are from P3 and P4 patients, classified as less acutely ill and stable on the PACS,5–7 and are considered as LAA. 8 Low-acuity ED attendances could be managed in primary care, and their ED visits hinder timely care for urgent cases.6,7,9 Given the widespread prevalence of this issue, there is an interest in identifying strategies for the local population aimed at reducing LAA. A review highlighted the effectiveness of co-payment schemes, and imposing of higher financial penalties in reducing LAA.10,11 However concerns have been raised about its potential to limit access to care for individuals in the lower income group. 10 Additionally, studies have shown that financial incentives, like a General Practitioner (GP)-referral subsidy scheme, and strengthening primary care services, with a focus on enabling GPs to handle a significant portion of LAA patients, are better strategies for mitigating ED overcrowding compared to increasing ED capacity.6,7,12
GPFirst, initiated in 2014 by Changi General Hospital (CGH) aimed to address ED overcrowding by promoting initial health-seeking at GPs for mild-to-moderate conditions. Patients who were subsequently referred to the ED are offered a $50 ED fee subsidy and priority classification for expedited care. To date, over 52,000 patients and 240 GP clinics in the eastern region of Singapore have participated in GPFirst.12–14 In the first year of GPFirst, the annual decline of self-referred LAA in the CGH ED was over 3.5 times higher than the decline observed in all other EDs across Singapore. 15 From 2014 to 2019, there was a 14% decrease in non-urgent cases and over a 36% decrease in the number of walk-in attendees without a doctor’s referral compared to pre-launch period.13,14 Additionally, GPFirst participants expressed high satisfaction with the programme.13,14,16
Singapore’s Ministry of Health (MOH) had plans to expand GPFirst beyond CGH’s region. 17 The programme was progressively implemented in all tertiary hospitals nationwide from 2020 to 2023, and is included as a care protocol under Healthier SG, a national preventative care initiative by MOH.13,14,18,19 No study has been conducted to examine the experiences of GPFirst participants, and to ensure the continued success of GPFirst, it is crucial to address this research gap. We utilised a qualitative approach to gain an in-depth understanding of participants’ perceptions of GPFirst, their health-seeking behaviours and explore recommendations for enhancing GPFirst.
Methods
Study design
The COREQ (Consolidated Criteria for Reporting Qualitative Research) 20 was utilised to guide the reporting of this study (Supplementary File 1). This study adopts an exploratory qualitative approach grounded in an interpretivist paradigm.21,22
Ethics
This study was conducted in accordance with the Declaration of Helsinki. Ethics approval was granted by the Singhealth Centralised Institutional Review Board (Ref: 2022/2691), and written informed consent was sought from participants.
Participant recruitment
Participants were eligible if they were: (1) referred to CGH ED through GPFirst within the preceding month; (2) aged 21 years or older; (3) English-literate; (4) Singaporean residents; and (5) able to provide consent. To prevent interference with their recovery, individuals who met these eligibility criteria but were subsequently readmitted before their interview were excluded from the study. This study utilised purposive sampling, targeting individuals referred to CGH ED through GPFirst within the previous month. All eligible participants were contacted through phone, using the monthly list of ED attendances provided by CGH. Study details were provided during the initial phone contact, and interested individuals were emailed a participant information sheet and an electronic consent form. A follow-up phone call was scheduled 24 h later, to address inquiries, obtain informed consent, and arrange the interview mode (in-person, phone call, or Zoom video call). Out of 88 invited participants, 13 (14.7%) initially agreed to be interviewed over Zoom, but one dropped out due to scheduling difficulties, resulting in a total of 12 recruited participants.
Data collection
An interview guide (Supplementary File 2) was developed based on literature review,11,16,23,24 and input from CGH GPFirst stakeholders. This guide aimed to explore participants’ experiences of their GPFirst journey and understand GPFirst’s facilitators and barriers. Semi-structured, in-depth interviews were conducted from February to May 2023 by first author GWX. GWX is a Chinese female in her thirties, employed as a podiatrist at Singapore General Hospital, with a Master of Public Health degree and training in qualitative research. There was no prior relationship with participants and GWX. Participants received a SGD30 voucher as a token of appreciation. All interviews were audio-recorded, anonymized, transcribed verbatim and notes were taken by GWX after each interview. The interviews ranged from 22 to 45 min.
Data analysis
Details of qualitative data analysis.

1. Braun V and Clarke V. Reflecting on reflexive thematic analysis. Qual Res Sport Exercise Health. 2019; 11(4): 589–597. DOI: 10.1080/2159676X.2019.1628806.
Results
Participant characteristics
Sociodemographic characteristics of study participants.

Themes, subthemes and supporting quotes.

Theme 1: Perceptions of GPs
GPs as the first port of call
The majority of GPFirst participants express a longstanding habit of initially consulting with their GP whenever they have a medical issue (Table 3).
Additionally, some chose to consult the GP due to civic responsibility, emphasising the prioritisation of ED care for those who needed it. “For me it is always GP first. Always…. if I was going to the ED, I would appreciate that all those people who do not need to be there, to not be there in the first place and take up my time, my medical attention there that I may need, or especially others that actually come in you know, really bad.” - IDI 8 (34yo, F, Eurasian)
Participants’ narratives underscored a preference for primary care and suggested a belief in using the ED only when necessary.
The reassuring role of the family GP
All participants had a regular GP and mentioned that consulting their GP prior to visiting the ED provided them with assurance and a better understanding of their medical condition. As a result of this preparatory interaction with their GP, participants experienced reduced anxiety.
Participants who chose to see a non-regular GP offered reasons such as the unavailability of their family doctor or the desire for a second opinion. “That day, I went to the (non-regular GP) clinic first was because I was nearby and it was open… I do have a usual family GP… they (family GP) are more caring.” – IDI 12 (32yo, M, Chinese)
It is noteworthy that none of these participants expressed a similar sense of reassurance when consulting with their non-regular GP. These narratives highlight the importance of the regular provider-patient relationship in patients’ health-seeking behaviours.
Theme 2: Patients’ expectations of GPFirst
ED fee subsidy fell short of participants’ expectations
While some participants expressed gratitude for the $50 ED fee subsidy, the majority held the perspective that “the $50 don’t really cover much” (IDI 10 – 44yo, F, Chinese). This sentiment was due to the dual payment incurred at both the GP and ED, resulting in a potentially higher bill size.
Furthermore, the adequacy of the $50 subsidy diminished when participants encountered additional expenses in the form of GP surcharges for weekend or after-hour care (Table 3). These suggested that adjustments to the GPFirst fee subsidy may be needed.
Prioritisation of GPFirst patients access to care at the ED
A minority experienced ED waiting times averaging 1–2 h, while the majority faced significantly longer waits, often exceeding 3 h. Importantly, many did not perceive any notable advantage in terms of faster service, despite being referred through GPFirst (Table 3).
A prevalent sentiment among participants was that there was “no difference” in waiting times between GPFirst referrals and self-referred patients. They believed that the ED prioritised cases based on the severity of the medical condition, irrespective of the referral source. “It doesn’t matter if I am a type 2 (P2) patient and... everybody there is a type 2 (P2) patient” – IDI 10 (44yo, F, Chinese)
In general, there was consensus that “those who walk in with a GP(First)… should be very high on that priority list to see the (ED) doctor first. Because they are walking in having seen a fellow doctor” (IDI 8 - 34yo, F, Eurasian). Participants believed that if their healthcare needs warranted escalation to the ED, then “being prioritised is actually the main thing” (IDI 12 – 32yo, M, Chinese). These narratives suggested that perceived severity of the condition outweighs the importance of financial subsidies.
Theme 3: Facilitators and barriers to utilising GPFirst
Cost influenced health-seeking behaviour
Almost all participants mentioned the influence of healthcare costs on their health-seeking behaviour. Participants tended to choose to visit providers whom they have medical cover for (Table 3).
Many suggested that reducing the cost of GP visits could incentivize GPFirst participation. They proposed various strategies to achieve this, such as eliminating GP surcharges, increasing government subsidies for GP visits, and raising the current $50 ED fee subsidy. “...subsidise more for the GP... It’s all money... if I know that if I go to the GP for almost free, I will go to the GP first.” – IDI 12 (32yo, M, Chinese)
Participants without any medical coverage tended to opt for providers who could offer services at the lowest out-of-pocket cost. There is consensus that visiting the GP “is a cheaper option” (IDI 3 – 31yo, F, Malay) compared to ED. However, the inclusion of GP surcharges reduced the cost difference between visiting the GP and ED and was perceived to be a deterrent to GPFirst.
Greater accessibility to care at GPs, but services offered was limited
Consensus existed among participants that waiting times at GP clinics were generally shorter, acting as a facilitator for GPFirst. The majority emphasised that “time is precious” and were “not willing to wait” (IDI 7 – 34yo, F, Chinese) for medical attention. Another facilitator mentioned was having a GP conveniently located close to their homes. However, when the GP clinic near to the participants was closed, accessing alternative healthcare providers such as the ED became a more feasible option (Table 3). “Some participants expressed unhappiness at the lack of relevant diagnostic or treatment facilities at their GP, which necessitated an ED visit. “He (GP) said he cannot do anything here – he told me to go ED.” – IDI 12 (32yo, M, Chinese)
These suggested that improving access to ancillary services might potentially reduce unnecessary ED visits by patients who lacked these services in primary care.
Interpersonal influences on health-seeking behaviour
The majority emphasised interpersonal factors, particularly their GP relationship and input from family and friends, as determinants for GPFirst utilization. Participants with a family GP were motivated to choose GPFirst due to the strong rapport with their physician. They believed that their GP’s intimate knowledge of their medical history, placed them “in a better position” (IDI 3 – 31yo, F, Malay) to guide their care. These participants also expressed confidence in the professionalism and care provided by their GP.
A common theme among most participants was the influence of family members and friends on their health-seeking behaviour in general. They placed high trust in the recommendations of their social circle. One participant expressed confidence that his family members would be “more sound minded to know where I should go” (IDI 12 – 32yo, M, Chinese) when he was unwell.
Recommendations for programme improvement
GPs as drivers of GPFirst awareness
The majority of our participants considered knowledge as a prerequisite for action, emphasising the importance of raising awareness to enhance GPFirst adoption. Many saw healthcare institutions as suitable platforms for promoting GPFirst. GPs were perceived to be more effective drivers of GPFirst compared to hospitals. This perception stemmed from the belief that given GPs’ frequent interactions and established therapeutic relationship, they had more opportunities for dissemination, either during consultations or while patients were waiting.
Leveraging social networks for GPFirst awareness
Compared to traditional or social media, participants believed that “word of mouth, that’s the best way” (IDI 5 – 31yo, F, Indian) to raise awareness of GPFirst. They perceived personal endorsement by individuals in their immediate social circle to be more persuasive than media advertisements (Table 3).
Address public misconceptions about GPFirst
A few highlighted the need for increased programme clarity. Rather than defining mild to moderate medical conditions, participants mentioned that “the most important things is for people to be aware of when is required to go to the emergency” (IDI 5 - 31yo, F, Indian). One participant also suggested that explaining the emergency department’s triage system could help GPFirst participants comprehend how they might benefit. Misunderstandings regarding the level of subsidies provided to GPFirst patients were also expressed.
Improving access and capabilities of GPFirst clinics
Most placed a high value on convenience when seeking healthcare. Several expressed a strong desire for more GPFirst clinics to extend their operating hours into the weekends and after regular hours (Table 3). Additionally, two participants suggested the use of telemedicine as an approach to enhance GPFirst utilization.
Participants expressed optimism about the potential impact of GPFirst in reducing crowding in the ED. They highlighted the importance of equipping GPFirst clinics to handle minor procedures such as stitching and same-day diagnostic tests (Table 3). Additionally, one participant recommended streamlining the referral process between GPs and Specialist Outpatient Clinics to enable same-day urgent reviews.
Ensuring fair prioritisation protocols at the ED
A few participants emphasized the necessity of prioritizing GPFirst patients in the ED. They believed that “the core purpose (of GPFirst) should be that it should differentiate the urgency (between walk ins and GP-referred patients)” (IDI 8 - 34yo, F, Eurasian) because GPFirst participants have already undergone assessments indicating their need for urgent care. Prioritizing GPFirst cases within the ED was seen as an opportunity to “increase visibility” (IDI 8–34yo, F, Eurasian) if done right. It was suggested that a dedicated queue in the ED exclusively for GPFirst patients could expedite care and generate further demand for the service.
Discussion
This exploratory qualitative study is the first to offers insights into the perceptions of GPFirst among participating patients. Extended ED waiting times, despite choosing GPFirst, raised questions among participants about the advantage of using GPFirst clinics when there is no improvement in ED wait times. Addressing this pressing issue is paramount to maintaining the programme’s relevance and effectiveness. Participants who were intrinsically motivated to embrace primary care showed support for the programme’s objectives. Those with established positive relationships with their GPs expressed fewer negative sentiments when reflecting on their GPFirst experiences and felt that their care was comprehensive, even in cases requiring escalation. This observation aligns with previous research highlighting the influential role of patients’ experiences with their primary care physicians in shaping their perceptions of the healthcare system, irrespective of their satisfaction with the care received. 28
Most participants contended that the $50 ED fee subsidy provided by GPFirst failed to offset the costs associated with their GP visits. Prior research has highlighted the importance of the GP-referral discount size in influencing the effectiveness of primary care linkage programmes. 12 Hence, this suggests the need for re-evaluation of GPFirst subsidies, considering that the subsidies have remained unchanged since GPFirst’s inception in 2014.
Participants discussed various external factors that influenced their decision to participate in GPFirst. Facilitators included reduced out-of-pocket GP expenses, shorter GP wait times, the convenience of GP clinic locations, and established relationships with their GPs, including recommendations by family and friends. Conversely, barriers encompassed the absence of medical coverage for GP visits, GPs being closed during weekends and after hours, and the absence of ancillary services at GPs. These findings are consistent with the literature 23 and the 2019 GPFirst survey, 16 whereby affordability of care, clinic accessibility, service availability, wait times, and the patient-physician relationship were common factors influencing engagement with primary care. 29
The interplay between these factors underline the interdependent relationship between health-seeking behaviour and the environment, as described by the Social Cognitive Theory. 30 Participants’ readiness to engage with GPFirst is tied to the broader context in which it operates, encompassing the healthcare and cultural landscape of Singapore. Consequently, it is imperative to collaborate with stakeholders such as Ministries and regional health systems beyond CGH to influence these factors. The inclusion of GPFirst in Healthier SG, 19 could offer novel opportunities to advocate for changes within the primary healthcare environment and cultivate stronger patient-physician relationships, in line with the “one family doctor, one care plan” policy.
Based on the findings from our study, recommended strategies to improve GPFirst were summarised utilising the micro, meso, and macro framework
31
(Figure 1; Supplementary 3). At the micro-level, it is crucial to intensify efforts in raising awareness about the programme. This involves expanding the role of GPs as advocates for GPFirst, utilizing the influence of existing GPFirst participants and their social networks to disseminate information, and addressing any misconceptions that may exist. Additionally, strategies for improving access include incorporating more 24-h GP clinics into GPFirst, offering alternatives for after-hours care such as urgent care centres, and exploring the potential integration of telemedicine services across all GPFirst clinics. Moving to the meso-level, strategies focus on expanding the capabilities of GPs by upskilling them to perform minor procedures onsite and facilitating their access to diagnostics and treatment modalities. This can be achieved by leveraging Primary Care Networks (PCNs) to consolidate resources and secure better prices with pathology and diagnostic labs. Fair prioritisation of GPFirst patients is also emphasised at this level, with recommendations for further triaging of LAA patients by referral source and appropriately directing GPFirst patients to a dedicated ED queue, established exclusively for them. At the macro-level, emphasis can be placed on expanding the capabilities of GPs through financial and structural support for ground initiatives aimed at upskilling them. Additionally, a streamlined referral pathway could be introduced to facilitate a direct and efficient route into specialized outpatient clinics for urgent same-day care. A comprehensive review of current fees and subsidies for EDs and GPs by relevant authorities could be performed to ascertain if changes to current pricing models are required. These strategies are directed by different entities, with the CGH GPFirst Programme Team and regional health systems overseeing micro and meso-level initiatives, while the Ministry of Health and regional health systems will guide the macro-level interventions. Our findings may also apply to comparable health-seeking initiatives in Singapore, such as NurseFirst, managed by Woodlands Health,
32
where trained nurses offer advice to residents with urgent but non-life-threatening medical conditions through the NurseFirst helpline. Recommended strategies for GPFirst according to the micro, meso, macro framework.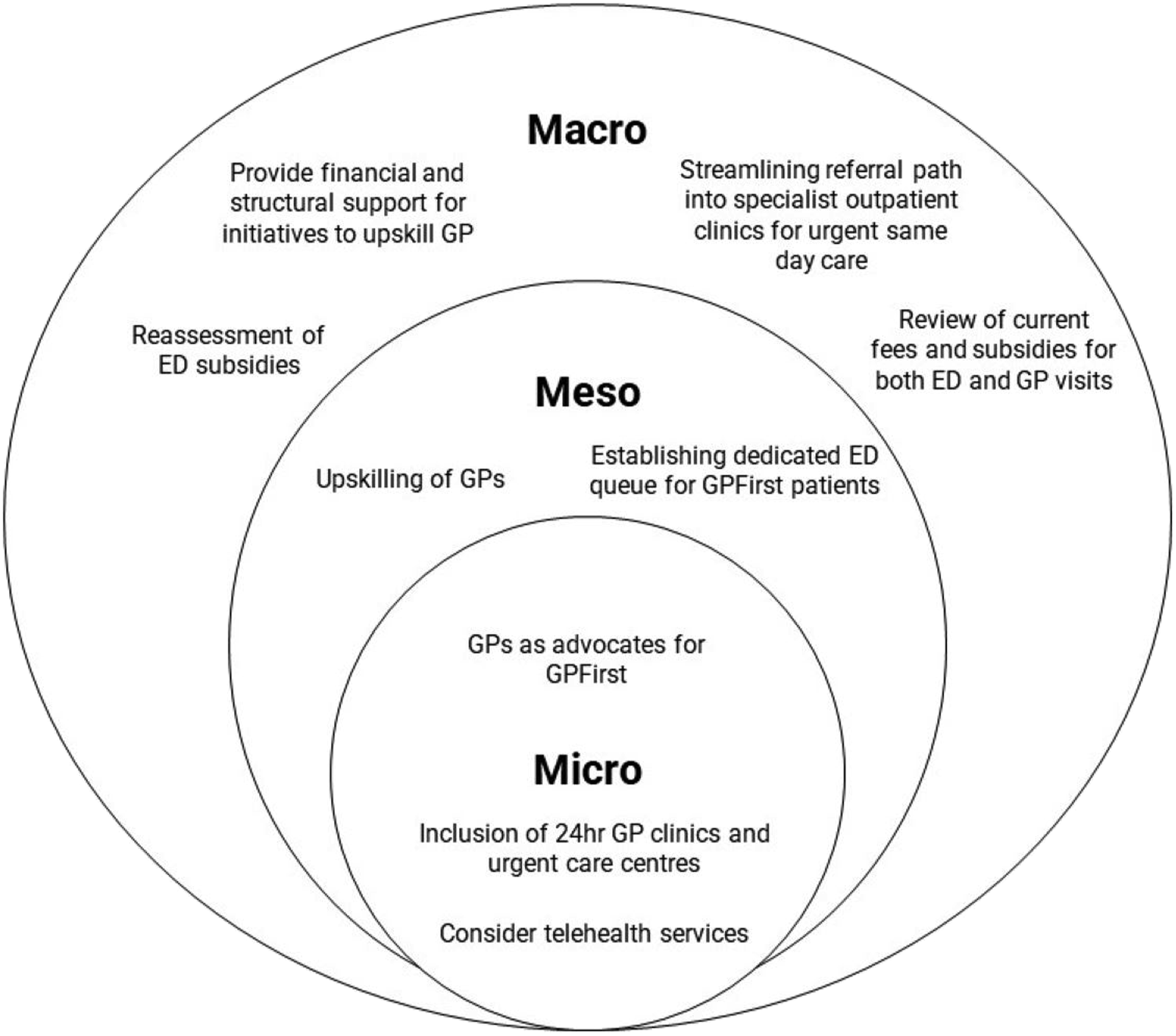
Strengths and limitations
Our study’s strength lies in addressing the research gap on GPFirst participants’ experiences, crucial for a nationwide programme rollout. The use of maximum variation purposive sampling enhanced the depth of our findings. Nevertheless, our study does have limitations. The absence of data saturation does not diminish the value of our findings, as the presence of widely prevalent themes suggests essential aspects of participants’ perspectives have been captured, offering valuable insights on GPFirst. The inclusion of only English-literate patients, coupled the relatively small sample size, may have limited the diversity of perspectives, which could affect the applicability of the results in Singapore’s multicultural society. Conducting remote interviews presented challenges in rapport-building and assessing non-verbal cues. However, this method was preferred by participants for its convenience.
Conclusions
This qualitative study provides invaluable insights into Singapore’s GPFirst programme. Experiences varied, with intrinsic motivation and positive relationships with family doctors playing a key role. Participants highlighted the need to reevaluate programme elements like ED fee subsidies and prioritization. Prolonged ED waiting times, even for GPFirst participants, raise concerns about the programme’s advantage. To advance GPFirst’s objectives, collaborating with stakeholders beyond CGH is vital to address these issues and enhance GPFirst adoption. Initiatives like Healthier SG offer potential avenues for change. We have outlined strategies within a micro-, meso-, and macro-level framework to facilitate this process. Additionally, further exploration of GPFirst providers’ perspectives could provide insights pertinent to implementation factors.
Supplemental Material
Supplemental Material - Patients’ perspectives on a programme to reduce emergency department use for low acuity conditions
Supplemental Material for Patients’ perspectives on a programme to reduce emergency department use for low acuity conditions by Wan Xi Goh, Rebecca Ong Hui Shan, Salome Antonette Rebello, Priscilla Goh Sook Kheng, Atikah Ahmad, Choon How How, Mohan Tiruchittampalam, Hong Choon Oh and Hoon Chin Steven Lim in Proceedings of Singapore Healthcare
Supplemental Material
Supplemental Material - Patients’ perspectives on a programme to reduce emergency department use for low acuity conditions
Supplemental Material for Patients’ perspectives on a programme to reduce emergency department use for low acuity conditions by Wan Xi Goh, Rebecca Ong Hui Shan, Salome Antonette Rebello, Priscilla Goh Sook Kheng, Atikah Ahmad, Choon How How, Mohan Tiruchittampalam, Hong Choon Oh and Hoon Chin Steven Lim in Proceedings of Singapore Healthcare
Supplemental Material
Supplemental Material - Patients’ perspectives on a programme to reduce emergency department use for low acuity conditions
Supplemental Material for Patients’ perspectives on a programme to reduce emergency department use for low acuity conditions by Wan Xi Goh, Rebecca Ong Hui Shan, Salome Antonette Rebello, Priscilla Goh Sook Kheng, Atikah Ahmad, Choon How How, Mohan Tiruchittampalam, Hong Choon Oh and Hoon Chin Steven Lim in Proceedings of Singapore Healthcare
Footnotes
Acknowledgements
We extend our appreciation to Ms Lee Yi Ru and Ms Eunice Tong for their invaluable assistance with research administration. Additionally, our heartfelt thanks go to all the participants who dedicated their time to this study.
Author contributions
GWX, SAR, OHC, LHC, planned and conceived the study design. GWX, SAR, OHC, ROHS were involved in the literature review. GWX, SAR, OHC were involved in obtaining ethical approval. SAR, OHC, LHC were involved in supervisory responsibilities. GWX was involved in participant recruitment and data collection. GWX, OHC, ROHS and SAR were involved in data analysis and interpretation. ROHS wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the NUS SSH-SPH Practicum Student Fund.
Ethical approval
Ethical approval for this study was obtained from the Singhealth Centralised Institutional Review Board (Ref: 2022/2691).
Trial registration
Not applicable because this study is not a clinical trial.
Data availability statement
The datasets generated and/or analysed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.