
Abstract
Background
Warfarin remains an important anticoagulant in certain patient groups. Though primarily liver-metabolised, recent research suggests renal function influences warfarin dosing. This has yet to be explored in a Southeast Asian population.
Objectives
To investigate the impact of renal impairment and ethnicity on warfarin dosing in a multi-ethnic Asian population.
Methods
A retrospective cohort analysis on patients seen at the institution’s anticoagulation clinic (ACC) between 2010 and 2019 was conducted.
Results
Among 3610 eligible patients, 70.7% had no/ mild renal impairment (eGFR≥60 ml/min/1.73m2), 24.7% had moderate renal impairment (eGFR 30 to <60ml/min/1.73m2), and 4.5% had severe renal impairment (eGFR<30 ml/min/1.73m2). Patients with moderate renal impairment required a 19% lower maintenance warfarin dose (β = 0.81, 95% CI 0.79–0.84, p < .001), and those with severe renal impairment needed a 30% lower dose (β = 0.70, 95% CI 0.66–0.75, p < .001) compared to patients with normal kidney function. Ethnically, 84.4% were Chinese, 9.5% Malay, and 6.1% South Asian. Compared to Chinese, Malays required an 18% larger maintenance dose (β = 1.18, 95% CI 1.12–1.23, p < .001), and South Asians needed an 83% larger dose (β = 1.83, 95% CI 1.73–1.94, p < .001). Compared to patients with normal renal function of the same race, South Asians with impaired renal function required a 16% lower dose, while Malay and Chinese patients needed 21% and 23% lower doses, respectively.
Conclusion
In this large multi-ethnic Asian study, renal function and ethnicity significantly affected maintenance warfarin dosing. South Asian patients required larger doses but were less affected by renal impairment compared to Chinese and Malays.
Background
Even with the advent of novel oral anticoagulants (NOACs), warfarin remains the anticoagulant of choice for prevention against thromboembolic events in selected patient groups, such as those with metallic valve replacements and Rheumatic Heart Disease-associated Atrial Fibrillation.1–4 Its narrow therapeutic index coupled with significant inter-individual variability in dosing requirements makes effective warfarin titration critical for patient safety yet uniquely challenging.
Though warfarin is primarily metabolised by the liver via hepatic cytochrome P450 enzymes, it has been described that kidney impairment is a predictor of maintenance warfarin dose in various studies done in North American, Japanese and Chinese populations showing that renally impaired patients required lower maintenance doses of warfarin to maintain target International Normalised Ratio (INR).5–8 Further, renal impairment is a risk factor for haemorrhagic complications during warfarin therapy,9–12 thereby increasing the need for careful warfarin titration in this patient group.
Racial background is another factor that has been shown to affect the maintenance dose of warfarin. For example, a Malaysian study showed that Indian patients required a significantly higher dose of warfarin to maintain target INR than Chinese or Malay patients, 13 and Chinese patients have been previously reported to require a lower warfarin maintenance dose compared to Caucasian patients. 14 On the other hand, it has been well described that Asian patients taking warfarin for atrial fibrillation have a higher risk of intracranial bleeding compared to non-Asian patients despite similar INR levels and time in therapeutic range.15,16
To our knowledge, the impact of renal function and race on warfarin dosing have not been evaluated in conjunction to see if renal impairment has the same magnitude of impact on warfarin dosing across different Asian ethnicities. This question seemed relevant to a population like Singapore’s which is multi-ethnic.
Objectives
We seek to describe the magnitude of impact of renal impairment and ethnicity on maintenance warfarin dose in a multi-ethnic Chinese, Malay, and South Asian Singaporean population, with the aim of making recommendations for adjustments to warfarin dosing by renal function and by race.
Methods
Patient cohort
A retrospective cohort analysis was conducted on patients seen for warfarin titration at the anticoagulation clinic (ACC) of our institution 1st January 2010 to 31st December 2019. Inclusion criteria were Chinese, Malay and South Asian adult patients who had reached a stable therapeutic dose of warfarin, defined as three or more consecutive visits with INR values in therapeutic range and without a change in dose; and who had available creatinine values within one year of their index ACC visit. South Asian patients were defined as those of Indian, Bangladeshi, Pakistani, Sikh and Sri Lankan descent.
Data collection
Prespecified patient demographic and laboratory variables, as well as warfarin dispensing data were collected from electronic health records as approved by the institution ethics approval board. For laboratory valuables, the reading closest in time to the index ACC visit was used. Body surface area (BSA) was calculated using the Du Bois and Du Bois formula. 17
Renal function
Renal function was stratified based on the Kidney Disease: Improving Global Outcomes (KDIGO) 2012 Chronic Kidney Disease (CKD) guidelines, 18 which suggest that the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation is the most accurate method of estimating renal function in order to stage kidney disease. For the purposes of this paper, the updated 2021 CKD-EPI creatinine-based equation 19 was used. Patients were then assigned a CKD stage per aforementioned KDIGO 2012 guidelines and grouped into 3 categories. Patients classified to KDIGO G1 and G2 GFR categories, i.e., those with GFR ≥ 60 mL/min/1.73 m2, were considered to have normal or only mildly impaired kidney function. Patients classified to KDIGO stage G3a and G3b categories or those with GFR 30 to 59 mL/min/1.73 m2, were considered to have moderately decreased renal function. Patients in KDIGO stage G4 and G5 categories, or those with GFR < 30 mL/min/1.73 m2 and patients on long term renal replacement therapy were classified as having severely impaired renal function. Estimated Creatine Clearance (CrCl) according to the Cockcroft-Gault formula 20 was also calculated as another estimation of renal function.
Outcome definitions and statistical analysis
A patient with stable anticoagulation was defined as one with three or more consecutive ACC visits without a change in warfarin dose and with INR within target range. The maintenance warfarin dose (mg/day) was defined as the average daily warfarin dose dispensed to the patient during the period of stable anticoagulation. As many patients had doses that varied by the day of the week, the average daily dose was used, which was calculated as total weekly warfarin dose in milligrams divided by seven days. For example, in a patient whose prescription was 3 mg on Monday, Wednesday, Friday and Sunday, and 2.5 mg on Tuesday, Thursday and Saturday, their calculated daily dose would be 2.8 mg per day. Target INR was defined as the mid-point between the lower INR target limit and upper INR target limit. For example, if a patient’s target INR was between 2.0 and 3.0, their target INR was calculated as 2.5.
P-values of less than 0.05 were considered statistically significant and odds ratios were derived with 95% confidence intervals. Continuous variables are presented as median with interquartile range (IQR), and comparisons were made using Wilcoxon rank sum test for non-parametric data. Categorical variables are presented as number with percentage (%) and were compared using the Fisher’s exact test. Median imputation was used for missing values of the continuous variables of height and weight, after checking for patterns and correlations. Datasets with and without imputation were used for subsequent analyses.
Log transformation was performed on daily dose of warfarin as its distribution was skewed. Linear regression analysis was then used to evaluate the relationship between ethnicity, CKD stage and mean daily warfarin dose. Additionally, the influence of all previously mentioned pre-specified patient variables on maintenance warfarin dose was also assessed. A multivariable model was then developed using all significantly influential variables from the univariate linear regression analysis. All analyses were performed using R, version 4.1.2 (R Project, www.r-project.org).
Results
From January 1st 2010 to December 31st 2019, 7074 patients were followed up by the ACC, with 133,703 individual consultations. 3610 patients fulfilled the inclusion criteria. See Figure 1 for the study flow diagram. Study Flow Diagram.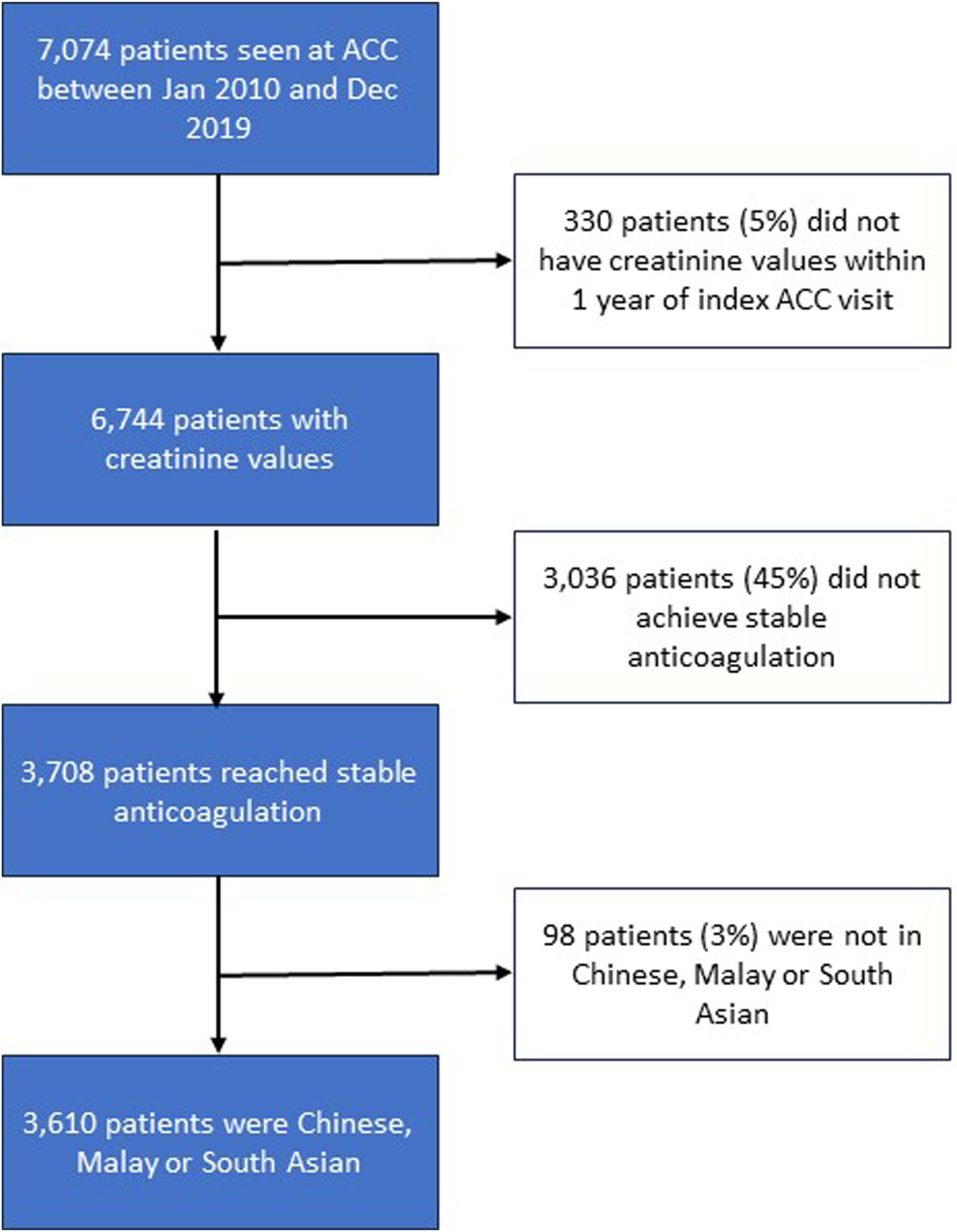
Patient Cohort Characteristics by Level of Kidney function.

Values shown are as median (interquartile range) or number (percentage). values for continuous variables are based on Kruskal-Wallis rank sum test; P values for categorical variables were calculated Fisher's exact test.
aHeight and weight data for 420 (11.6%) patients was not available. 10.6% of patients with normal renal function did not have height and weight measurements recorded. The corresponding percentage for patients with moderately and severely impaired renal function was 14.3% and 12.2% respectively.
bOther indications include thrombophilic condition, thromboembolic event (not PE/DVT), ACHD etc.
cTarget INR was defined as the midpoint between lower and upper INR targets. For example, if a patient's lower INR target limit was 2.0 and upper INR target limit was 3.0, INR target was calculated as 2.5.
Abbreviations: ALT, alanine transaminase; AST, aspartate transferase; BMI, body mass index; BSA, body surface area; DVT, Deep Vein Thrombosis; eGFR, estimated glomerular filtration rate; PE, pulmonary embolism.
The target INR for the cohort was 2.50 (IQR 2.50, 2.50) and the actual achieved median INR was 2.40 (IQR 2.19, 2.60). Target INR and achieved INR did not differ significantly between the different categories of renal function, nor between the different ethnic groups.
Maintenance warfarin dose was significantly and positively correlated to estimated glomerular filtration rate (p < .001). Figure 2 shows median warfarin average daily dose requirements stratified by kidney function. Compared with patients with normal kidney function, patients with moderately impaired kidney function required a 19% lower (β = 0.81, 95% CI 0.79 to 0.84, p < .001) daily dose of warfarin to achieve stable anticoagulation; and patients with severely impaired renal function required a 30% (β = 0.70, 95% CI 0.66 – 0.75, p < .001) lower daily maintenance dose. After isolating for all other variables, the correlation between renal function, as measured by eGFR, and warfarin dose was still significant (p < .001). In the multivariate analysis, patients with moderately impaired and severe impaired kidney function required 9% (β = 0. 91, CI 0.89 – 0.94) and 21% (β = 0. 79 CI 0.75 – 0.85) lower doses compared to patients with normal renal function. Estimated creatine clearance, another measurement of renal function, was also significantly (p < .001, r2 0.16) and positively correlated with daily maintenance warfarin dose (see Figure 3). Median Daily Warfarin Maintenance Dose Stratified by Level of Kidney Function. Estimated creatine clearance and maintenance warfarin dose.

Maintenance warfarin dose was significantly correlated with race (p < .001), as seen in Figure 4. Compared with Chinese patients, Malay patients required a 17% (β = 1.17, 95% CI 1.13 – 1.23) larger warfarin dose and Indian patients required an 82% (β = 1.82, 95% CI 1.73-1.93) larger warfarin dose, to achieve stable, therapeutic anticoagulation. After controlling for all other variables, race was still significantly correlated with warfarin dose, with Malay patients requiring an 8% (β = 1.08, 95% CI 1.04-1.13) higher dose, and Indian patients needing a 73% (β = 1.73, 95% CI 1.64-1.82) higher dose than Chinese patients. Median Daily Warfarin Maintenance Dose Stratified by Race.
The impact of renal impairment on maintenance warfarin dose was directionally consistent between the races. Figure 5 shows maintenance warfarin dose stratified by race and renal function. Chinese patients with renal impairment (eGFR < 60 mL/min/1.73 m2) required 0.6 mg or 21% less warfarin per day (95% CI 0.20 to 0.22) to maintain therapeutic anticoagulation compared to patients with normal renal function (eGFR ≥ 60 mL/min/1.73 m2). The corresponding difference in daily maintenance dose was 0.8 mg per day for both Malay and Indian patients, or 23% (CI 0.22 to 0.24) and 16% (CI 0.15 to 0.17) respectively. Difference in median values between all six groups were statistically significant. The difference between the group with the highest average daily warfarin maintenance dose and lowest average daily maintenance dose, i.e. South Asian patients with normal renal function versus Chinese patients with impaired renal function, was 2.8 mg per day or 55% (95% CI 0.53 to 0.57). Median Daily Warfarin Maintenance Dose Stratified by Race and Renal Function.
Figure 6 lists the median warfarin dose requirement stratified by race and CKD stage in a dose “heatmap”, as an example of how race and renal function combine to influence warfarin dosing. A pair-wise test of the individual median values was not statistically significant. Heat Map of Median Warfarin Dose Stratified by Race and Renal Function.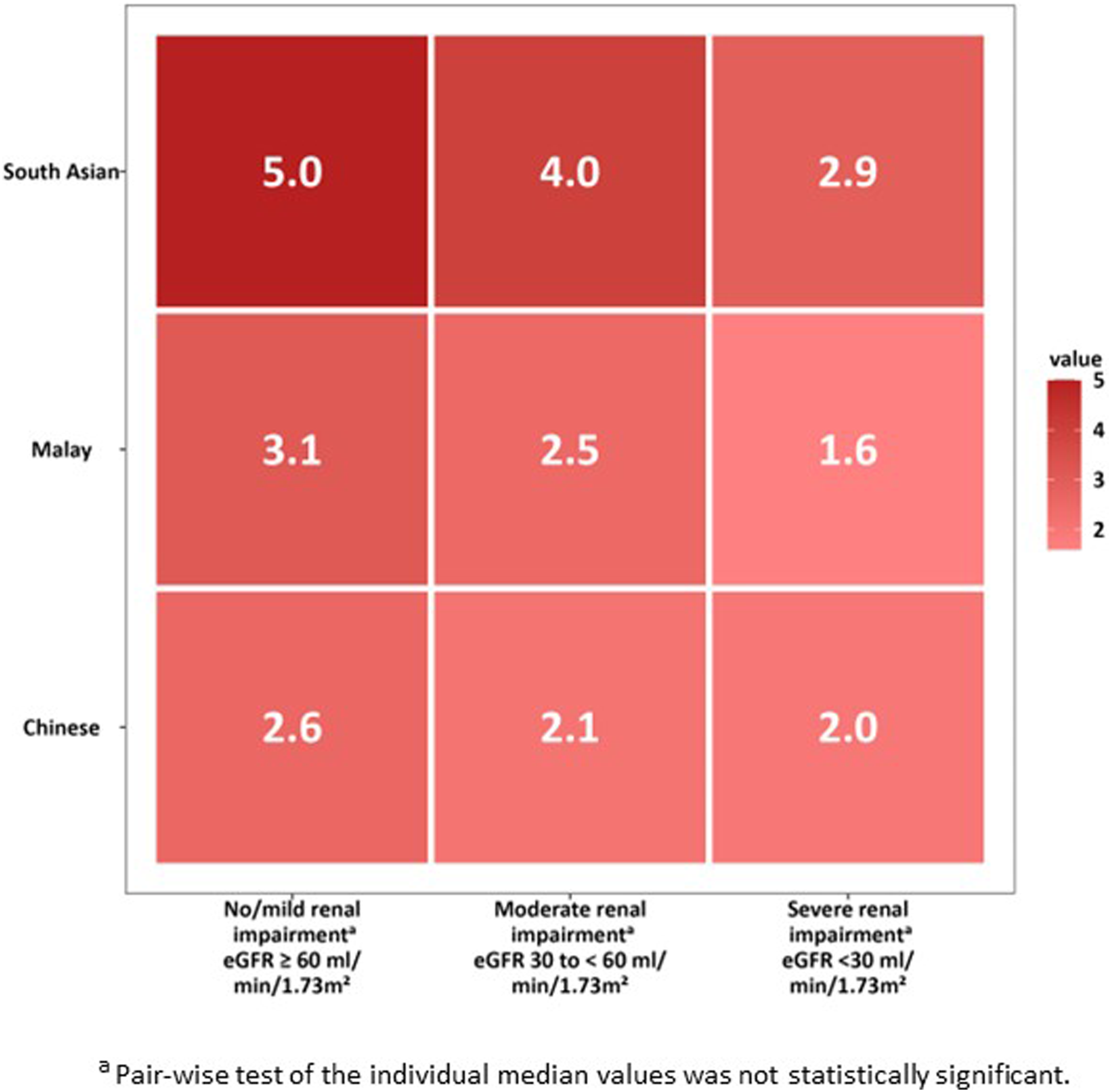
Univariate and multivariate linear regression.
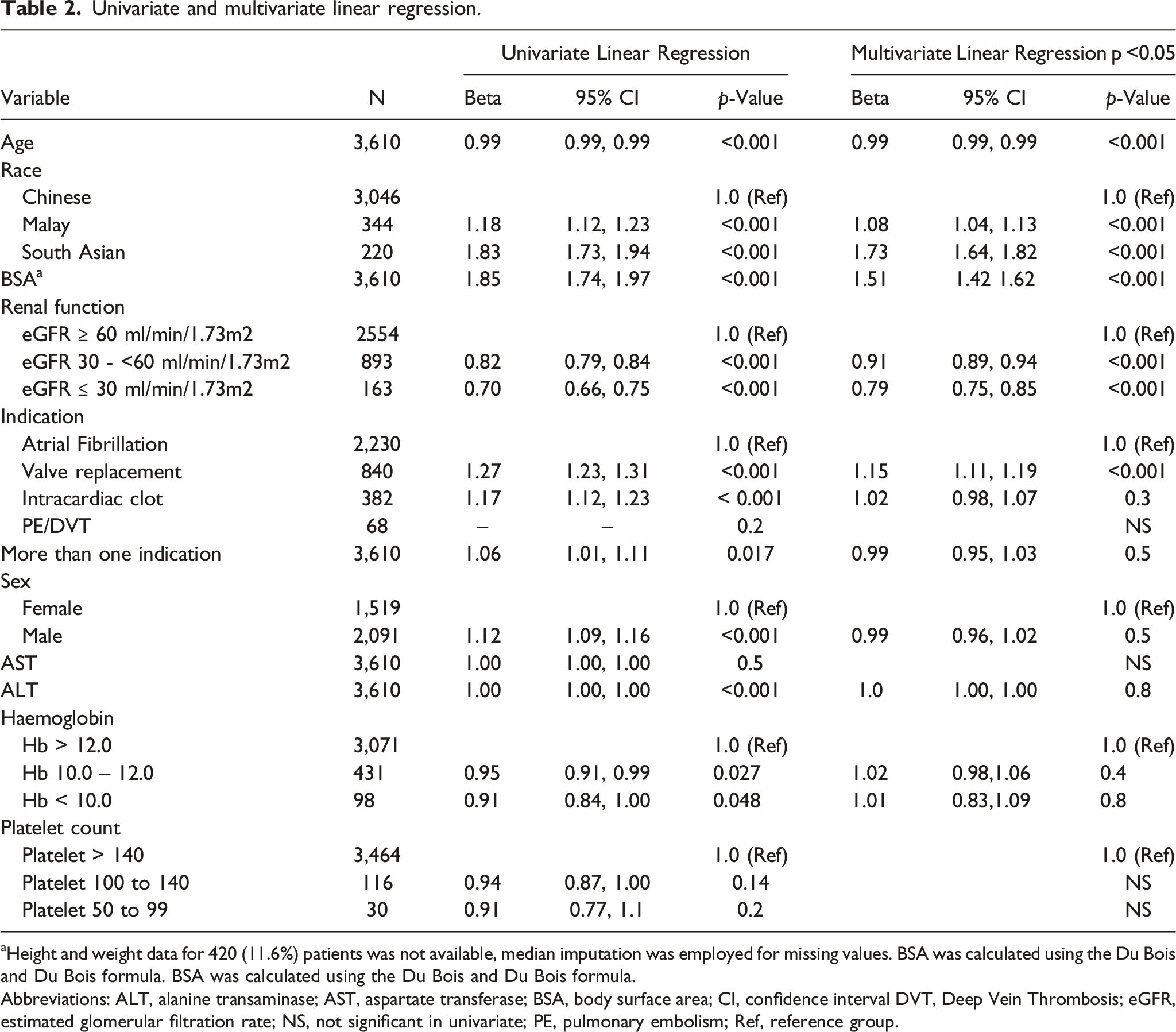
aHeight and weight data for 420 (11.6%) patients was not available, median imputation was employed for missing values. BSA was calculated using the Du Bois and Du Bois formula. BSA was calculated using the Du Bois and Du Bois formula.
Abbreviations: ALT, alanine transaminase; AST, aspartate transferase; BSA, body surface area; CI, confidence interval DVT, Deep Vein Thrombosis; eGFR, estimated glomerular filtration rate; NS, not significant in univariate; PE, pulmonary embolism; Ref, reference group.
Discussion
Warfarin dose and renal function
To our knowledge the impact of renal impairment on maintenance warfarin dosing has not been described in a multi-ethnic Asian population. Moreover, this is the largest study of the impact of renal impairment on warfarin maintenance dosage that we are aware of. Our retrospective study showed that renal function was an important determinant of warfarin dosing in a Southeast Asian population. Compared to patients with normal kidney function, patients with moderate and severe renal impairment required significantly lower maintenance warfarin doses of 9% and 21% less respectively after controlling for other significant variables.
These findings are similar to two previously published studies from different geographies. A prospective North American study of 980 European American and African American patients showed that patients with moderate and severe kidney impairment required 11% and 21% less warfarin respectively to achieve stable anti-coagulation. 6 Similarly, a recent prospective Japanese study of 137 patients showed that patients with moderate and severe kidney impairment required lower warfarin maintenance doses of 19% and 34% respectively, when compared to patients with normal renal function. 5 The definition of moderate and severe renal function impairment was the same in these two studies as in our study. While warfarin dosing is known to be subject to individual variability, to our knowledge this is the first local study that highlights how dosing requirement may differ across the spectrum of renal impairment.
Although the mechanism of how renal impairment affects the pharmcokinetics of non-renally cleared drugs has not been definitively elucidated, animal models have demonstrated the down regulation of hepatic cytochrome P450 in chronic renal failure. One study has also shown demonstrated that the S-Warfarin enantiomer which is exclusively eliminated by CYP2C9 is significantly increased in end stage renal failure, suggesting a decrease in hepatic CYP2C9 activity in renal failure. 21
Warfarin dose and race
It is well established that race is also an important variable in warfarin dosing. A prospective Malaysian study of 100 patients (55 Chinese, 19 Indians, and 26 Malays) showed that Indian patients required a significantly higher daily warfarin dose (6.9 mg) compared to Chinese (3.6 mg) and Malay (3.2 mg) patients. 13 Like the Malaysian study, our study showed that Indian patients required a significantly higher daily maintenance dose of warfarin when compared to Chinese and Malay. Indeed, LASSO analysis identified South Asian race as the most significant variable in the multivariable analysis. In our study however, the maintenance dose for South Asians was lower at 4.8 mg per day (IQR 3.6 – 6.0) compared to 6.9 mg in the Malaysian study. Further, unlike the aforementioned Malaysian study, this study showed a significant difference in the maintenance warfarin dose of ethnically Malay and Chinese patients, with Malay patients requiring a higher maintenance dose of 3 mg per day (IQR 2.2 - 4.0) compared to 2.5 mg per day in Chinese patients (IQR 2.0 - 3.3).
The influence of race on the impact of renal impairment on warfarin dosing
Directionally, the impact of renal function on warfarin dosing was similar amongst the races in this study, with impaired renal function reducing maintenance warfarin dose in all three races. We further attempted to evaluate whether the magnitude of impact of renal impairment on maintenance warfarin dosing differed between the races. Although the quantum of reduction in daily warfarin dose from renal impairment was similar between the races (0.6 mg to 0.8 mg per day), the percentage difference in maintenance dose using patients with normal renal function as a baseline comparator, was significantly different, with Indian patients less impacted by renal impairment compared to Malay patients (16% vs 21%), who in turn were less impacted than Chinese patients (21% vs 23%).
This study highlights the significant differences in maintenance warfarin doses between races that is further attenuated by renal function. It is common practice for healthcare institutions to have warfarin initiation protocols that may take into consideration clinical factors such as age, size of the patient, liver function etc., followed thereafter by dosing based on individual patient’s INR. 22 After the initiation period, there is usually a phase of intensive INR monitoring during which warfarin dose is titrated and a maintenance dose is established. Our study seeks to provide guidance on an eventual maintenance dose. For example, in our study, Indian patients with normal renal function required a median maintenance dose of 5.0 mg per day, whereas Chinese patients with impaired renal function only required a median maintenance dose of 2.1 mg per day. It is thus conceivable that when faced with patients who have been initiated on warfarin but are still at subtherapeutic INRs, a larger warfarin dose should be ordered for an Indian patient compared to a Chinese patient, and smaller warfarin doses should be ordered for patients with impaired renal function compared to those with preserved renal function. Figure 5 provides median maintenance doses by race and renal function.
Limitations
This study has several limitations. Firstly, it is a retrospective study with its inherent limitations. However, the retrospective nature of the study allowed for a large sample size of 3610 patients, and of the original cohort, only 5% of patients did not have an associated creatinine value.
Another important limitation is the lack of information on co-administration with other drugs and a lack of specifics on patient’s diets (e.g vegetarian or otherwise). It is well established that warfarin has significant drug-drug interactions and drug-diet interactions which were not evaluated in this study. 23
Further, this study did not include information on genetic factors. Genetic variation is now widely accepted to be a significant contributor to warfarin dosing variability,24–28 with multiple published warfarin titration algorithms incorporating the presence of certain vitamin K epoxide reductase complex (VKORC1) and CYP2CP single nucleotide polymorphisms as key variables in their algorithms. While the inclusion of genetic variables has been shown to improve the predictive ability of warfarin titration algorithms, the clinical application of these algorithms in randomised controlled trials have not been conclusively shown to improve time in therapeutic range.24,25,29 As the goal in our current study was to look at factors that would be readily available in the clinical setting, it was not considered feasible or appropriate to examine genetic variables.
Finally, while studies have shown that renal impairment is a risk factor for haemorrhagic complications during warfarin therapy, 9–12 adverse outcomes data was not available for our study cohort to evaluate if there are any differences in the incidence of haemorrhagic adverse events between the races at therapeutic INR, which could help to further guide how warfarin dosing should be managed our local multi-ethnic setting.
Conclusion
This large retrospective cohort study of Chinese, Malay and South Asian patients showed that renal function and race were both important determinants of maintenance warfarin dosing, with impaired renal function correlated with lower warfarin maintenance doses. While South Asian patients required a markedly larger maintenance warfarin dose than Chinese and Malay patients, the magnitude of impact of impaired renal function on warfarin dosing was less pronounced in South Asian patients compared to their Chinese and Malay counterparts.
Footnotes
Author contributions
OT researched the literature, conceived the study, oversaw the data analysis and wrote the first draft of the manuscript. HJS and ML assisted in data gathering and checking the integrity of the data. LYH was involved in data gathering, data analysis and producing the charts and tables. TC and FJM were involved in reviewing and editing the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Informed consent
Informed consent was not sought for the present study as approved by the Institutional Review Board as retrospective data used was de-identified and anonymised before analysis was performed. All data collected, given it’s retrospective nature, was derived from clinically indicated practices that had already occurred and thus was not expected to affect clinical decisions about an individual’s care nor cause inconvenience, discomfort or harm to the individual.
Data availability statement
The datasets generated and/or analysed during the current study are available from the corresponding author (OT).