
Abstract
Background
Late 2022, an ICU nurse discovered that Seretide™ (salmeterol/Fluticasone) Evohaler, a commonly used inhaler, did not change its dose counter when used with the inhaler connector 22M-22F. This was identified as a medication safety issue. Knowledge gaps of inhaler use in mechanically ventilated patients were identified as well.
Aims
To effectively administer metered dose inhalers to ventilated patients and increase its accuracy and safety.
Methods
We instituted education programs for healthcare professional in the ICU and introduced a new inhaler connector RTC 24-V. This was compared with the existing 22M-22F connector in a comparative study.
Results
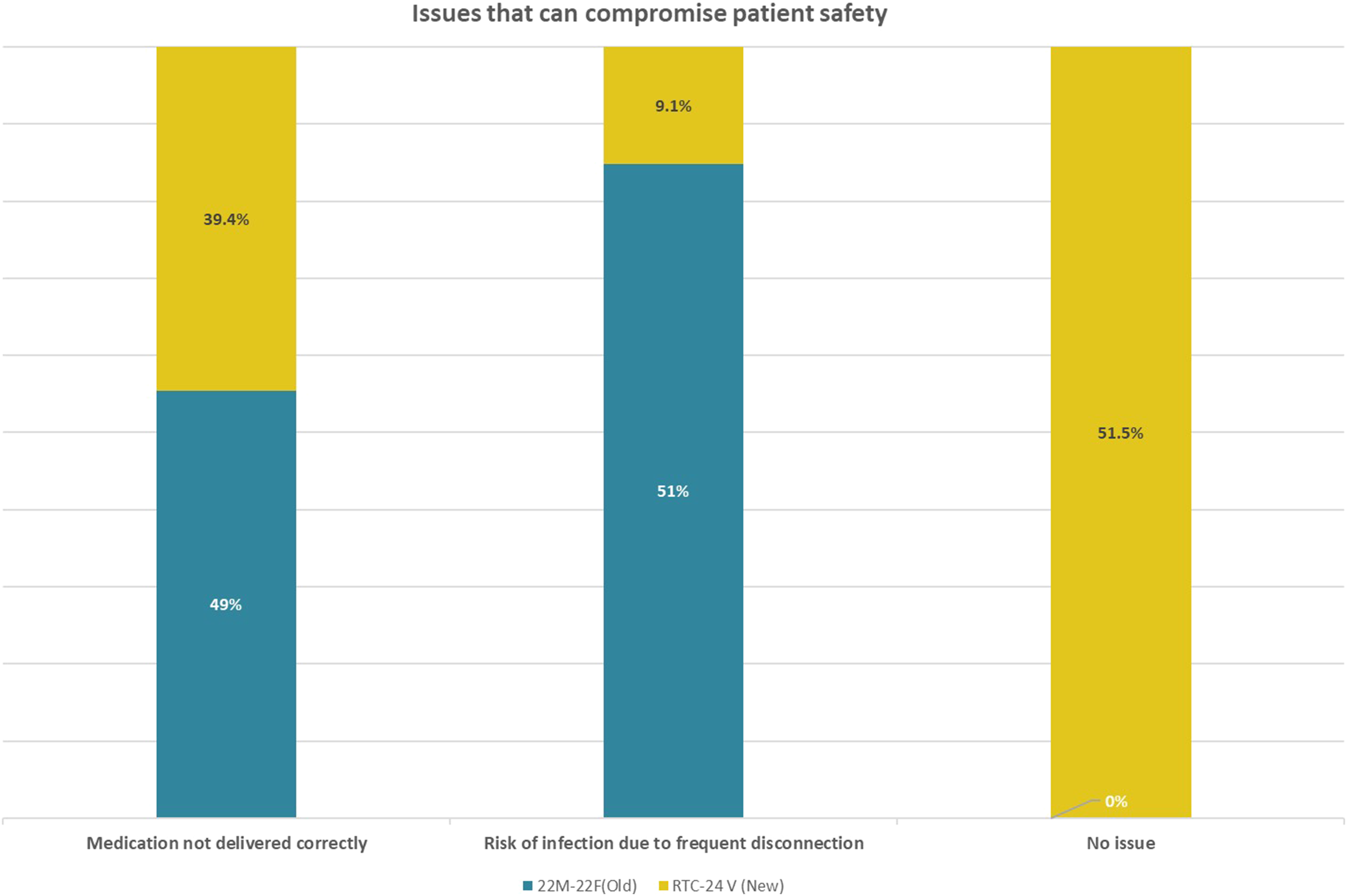
The dose counter of Seretide™ recorded prior to initiation and extubation showed an obvious drop in doses ranging from 15 to 63 in patients randomized to use RTC 24-V, compared to 0 to 2 drop in doses for patients using 22M-22F. A total of 51 pre study and 33 post study questionnaires were completed. Confidence that the accurate dose of medications was administered rose from 58.8% to 84.8% after using the RTC 24-V. Responses that there was no issue compromising patient safety rose from 0% to 51.5% and fewer staff expressed concern about disconnections causing infections, dropping from 51% to 9.1%. 93.9% of respondents chose the new RTC 24-V as the preferred inhaler connector.
Conclusion
The new inhaler connector RTC 24-V was assessed to have less medication errors. ICU healthcare professionals expressed greater confidence in its safety and accuracy. We will implement the use of this connector with continued medical education.
Keywords
Background
Bronchodilator therapies are commonly used in mechanically ventilated patients. 1 Bronchodilator drugs considerably reduce airway resistance both in patients with obstructive airway disease and acute lung injury.2,3 These medications are part of routine therapy in patients with obstructive lung disease (chronic obstructive pulmonary disease [COPD] or asthma) and serve a significant role in patient management.4,5 For ambulatory patients, there are many modalities available ranging from metered dose inhalers (MDIs), dry powder inhalers, soft mist inhalers, and nebulizers. In mechanically ventilated patients, bronchodilators are delivered either through systemic or inhaled route.2,5 MDIs and nebulizers were the mostly commonly used modalities of inhalation therapies.
Delivery of bronchodilators with metered dose inhalers in mechanically ventilated patients have several advantages over the nebulizer, such as reduced cost, ease of administration, less personnel time, reliability of dosing and a lower risk of contamination6,7 Furthermore, the use of nebulizers may result in patient ventilator dyssynchrony. When the flow rate of the continuous in-line nebulizer exceeds the patient’s inspiratory flow rate, the flow is incorrectly read by the ventilator as reflecting minute ventilation. This might result in severe periods of hypoventilation that are not noticed by the alarm function. 8
Inhaler connectors can be used to administer metered dose inhalers but not for dry powder inhalers. The current inhaler connector used in our Intensive Care Unit (ICU) is the Connector 22M-22F by Intersurgical. One of the metered dose inhalers commonly used in our ICU is Seretide™ (salmeterol/fluticasone) Evohaler by GSK which is a long acting beta agonist and inhaled corticosteroids (LABA/ICS) inhaler. Seretide™ Evohaler has a dose counter which decreases with each dose administered when used in its original actuator. An ICU nurse discovered in late 2022 that when used in ventilated patients, the dose counter did not decrease after each actuation using the current inhaler connector. This would potentially result in medication delivery errors due to discrepancy between the dose counter and the actual medication left in the canister. This might also affect the accuracy of the dose of the inhaler drug given.
Methods
Assessment of problem
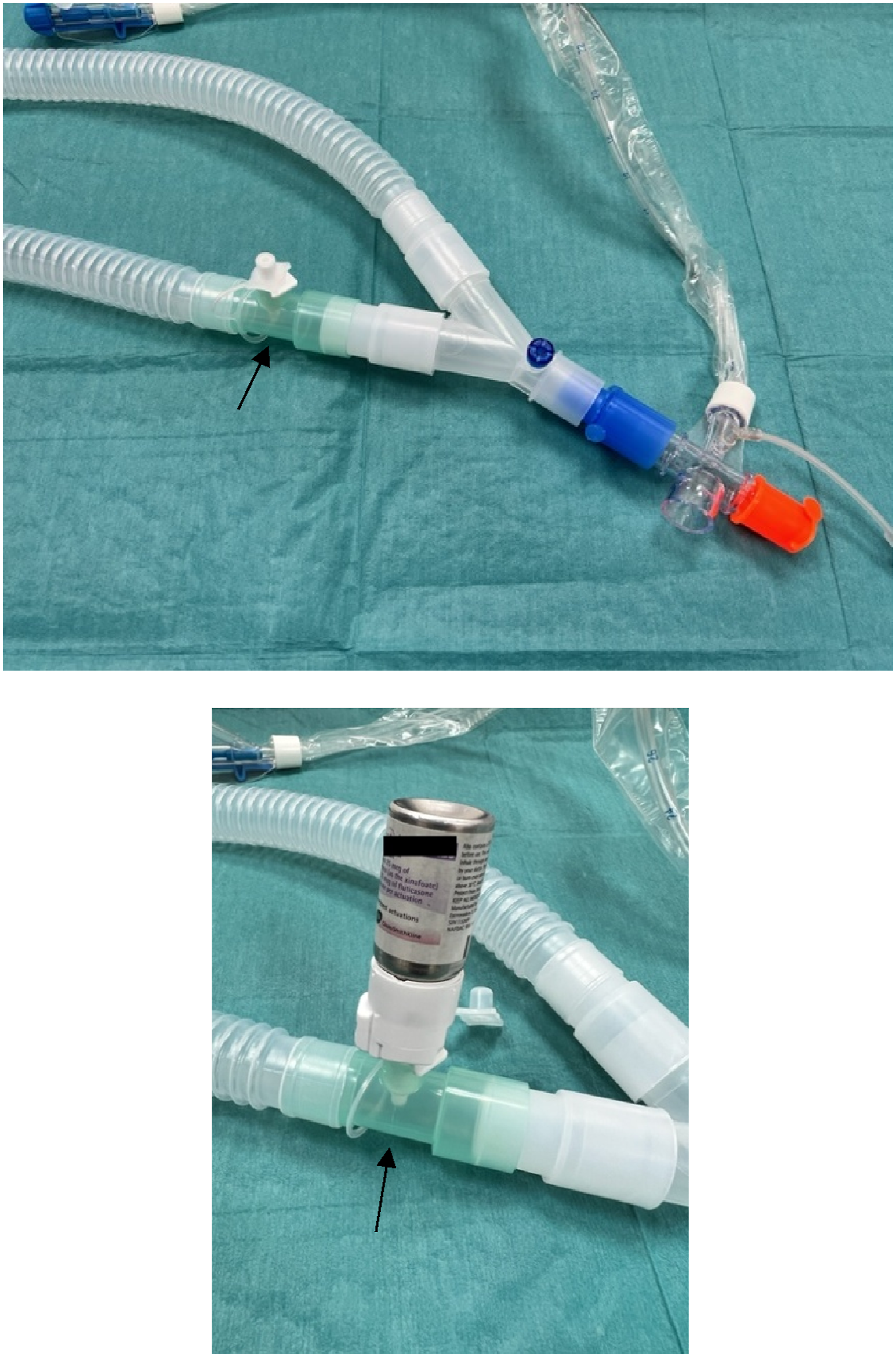
Investigations into this issue and inhaler use in the ICU were looked into. A few issues were identified, including that of equipment, processes and knowledge gaps amongst healthcare professionals in the ICU. This is analysed and displayed in Figure 1. One major concern was that of the inhaler connector 22M-22F by Intersurgical (Figure 2), which was the only connector available in our ICU for delivery of MDIs. When using this connector, the dose counter of the MDI did not register a change following the actuation of the MDI. This was likely due to the fact that these MDIs had to be removed from its actuator to be used directly with the inhaler connector and the connector lacks a spike that can change the dose counter. There were also knowledge deficits amongst healthcare professionals with respect to which inhalers could be administered in mechanically ventilated patients and also on how to administer them. An example of this was some doctors prescribed soft mist inhalers and ICU staff had been seen administering them directly via the endotracheal tube opening. Fishbone diagram: cause and effect analysis of possible causes of inaccurate delivery of inhalers in ventilated patients. 22M-22F inhaler connector (arrow).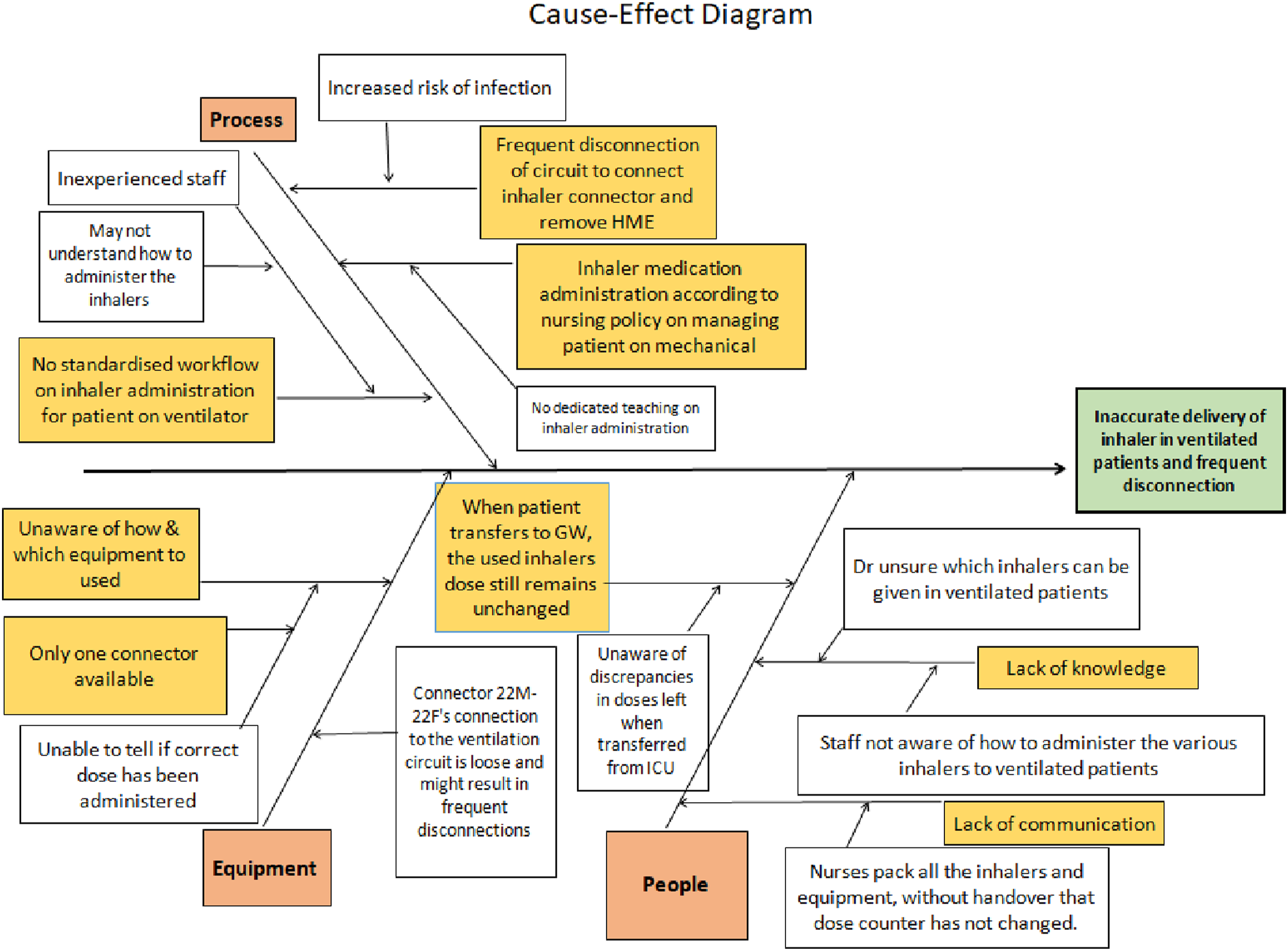
QI objectives
Our objective was to improve the effective delivery of inhalers in our ICU by assessing appropriate inhaler connectors and educating personnel. Our aim was to effectively administer metered dose inhalers to ventilated patients and increase its accuracy and safety by 100% within 3 months.
Introduction and evaluation of a new inhaler connector
Sourcing for a different inhaler connector was initiated and a different connector was found. Universal inline MDI adapter RTC 24-V by Instrumentation Industries was found to be able to change the dose counter on Seretide™ Evohaler when used (Figure 3). Samples were obtained and trouble shooting was done to connect the inhaler connector RTC 24-V to our ventilator circuit (Figure 4). Additionally we found out that the RTC 24-V had a tighter fit to the ventilator circuit when compared with the existing connector 22M-22F. This resulted in a change in practice. The RTC 24-V was left in the circuit during the entire duration of ventilation and there was no need to disconnect it from the ventilation circuit after administration of the MDIs. RTC 24-V inhaler connector (arrow). How to connect the RTC 24-V to inhalation limb of ventilator circuit.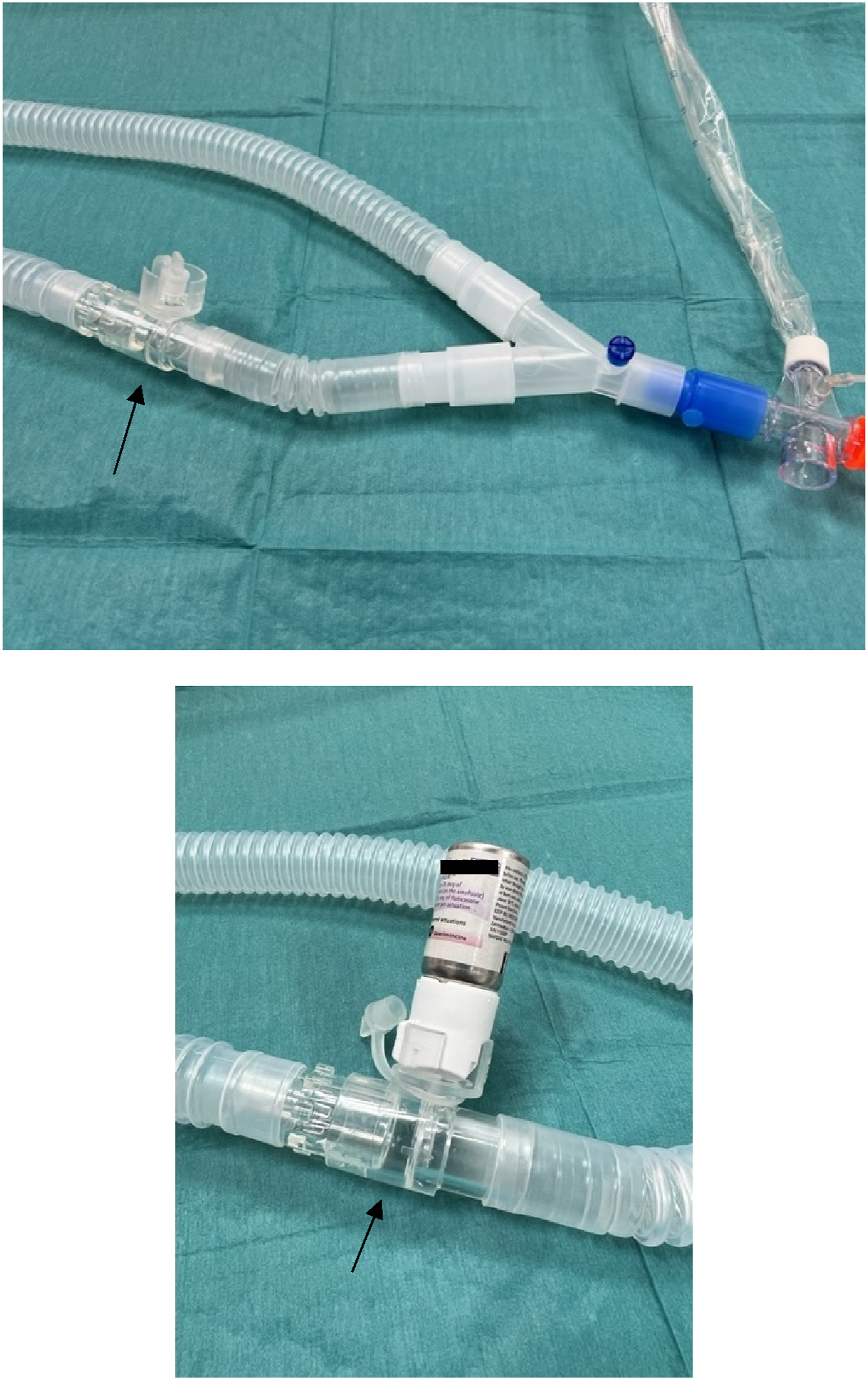

Education
Doctors were updated on the different types of bronchodilators and which inhalers can be safely given in mechanically ventilated patients. They were advised on which LABA/ICS inhalers can be prescribed as well. Nurses and Respiratory Therapists (RT) received training as well. They were empowered to escalate to doctors if inappropriate inhalers had been prescribed. The new inhaler connector RTC 24-V was introduced to all medical personnel in the ICU and they were taught how to connect it to the ventilator circuit. The healthcare professionals were also taught how to use it to administer MDIs. The nurses and RTs were told to leave the RTC 24-V in circuit and monitor for accidental disconnections.
Study
A comparative pilot study was done to compare the old connector 22M-22F with the new RTC 24-V. The study was carried out using purchased RTC 24-V connectors. We decided to recruit eight mechanically ventilated patients who had been started on Seretide™. The patients were randomized to either using the old inhaler connector 22M-22F or the new RTC 24-V inhaler connector. Nurses and RTs were told to draw cards with photos of either connector from an envelope, which indicated the group they are randomized to.
Nurses and RTs were given a short education session on metered dose inhalers and the current connector 22M-22F prior to the study period. They were then asked to answer a survey questionnaire. After completing the initial survey, they were introduced to the new inhaler connector RTC 24V. They were taught how to connect it to the ventilator circuit and how to administer the metered dose inhalers using the new connector. The change in practice of leaving the inhaler connector RTC 24-V in circuit for the entire duration of ventilation was also highlighted to them.
During the study period, nurses and RTs identified mechanically ventilated patients who were prescribed Seretide™ to be included in the study and randomized. Ethics approval and patient consent was not sought as this is a quality improvement project with minimal risk to the patients. Advice was given to ward nurses if discrepancies between dose administered and dose counter readings arose. The number on the dose counter of Seretide™ was recorded prior to the initiation of drug administration via the inhaler connector and also after the patients were extubated. The nurses who were caring for patients randomized to the new RTC 24V inhaler connector were given a post survey questionnaire to understand the user satisfaction and preferences after using the new connector. When indicated, the patients also received salbutamol and ipratropium bromide MDIs via the inhaler connector that the patients were randomized to.
Results
A total of seven patients were recruited with eight sets of results as one of the patients was re-intubated and randomized to a different inhaler connector. Each duration of mechanical ventilation ranged from 2 to 4 days. Four were in patients with COPD and four others in patients with asthma. All the patients were subsequently discharged from the ICU and subsequently from the wards with no inpatient mortality. All the above patients were on Seretide™ Evohaler 25/125 mcg with dosing ranging from 2 to 8 inhalations twice a day.
For the patients randomized to the inhaler connector 22M-22F, the dose counter of Seretide™ recorded prior to initiation and extubation showed a reduction in number from 0 to 2 doses, whilst those randomized to the RTC 24-V showed an obvious reduction in dose counter ranging from 15 to 63. Dose accuracy was determined by comparing predicted dose using documented drug dosing regimens versus actual dose counter change by the 2 inhaler connectors (Figure 5). The new RTC 24-V inhaler connector led to a dose counter change with almost 100% correlation to that of the predicted dose administered, while the inhaler connector 22M-22F barely changed the dose counter of Seretide™ Evohaler. On enquiry with the nurses in charge, the drop in dose counter for patients using the connector 22M-22F was due to either priming or testing the Evohaler when still in the original actuator. Comparisons of predicted dose using documented drug dosing regimens versus actual dose counter change.
A total of 51 pre study and 33 post study questionnaires were completed. Significant differences were noted in the confidence level amongst healthcare professionals that the accurate dose of medications was administered; rising from 58.8% to 84.8% after using the RTC 24-V (Figure 6). Healthcare professionals felt more confident with the RTC 24-V and responses that there were no issues compromising patient safety rose from 0% to 51.5% (Figure 7). Fewer nurses and respiratory therapist felt worried about disconnections causing infections, decreasing from 51% to 9.1% (Figure 7). No reports of accidental disconnection with RTC 24-V was received despite it being left in circuit for the entire duration of mechanical ventilation. 93.9% of respondents chose the new RTC 24-V as the preferred inhaler connector with reasons ranging from stability of the connection to the more accurate reflection of the dose delivered. Confidence level of ICU staff in the accuracy of metered dose inhalers administration using the 2 different connectors. Comparisons of issues that can compromise patient safety when using the 2 inhaler connectors.
Discussion
This quality improvement project was initiated with the discovery of the problem that the pre-existing inhaler connector 22M-22F for ventilators did not facilitate the change in the dose counter reading on Seretide™ Evohalers following actuation of the device. Currently, this connector is being used by many ICUs in Singapore to deliver MDIs to mechanically ventilated patients. Seretide™ Evohalers are one of the few LABA/ICS combination inhalers that can be administered safely and accurately in ventilated patients. It has also been shown in a small study that its administration in patients with COPD can improve lung mechanics. 9 Despite the above, a pubmed search did not reveal any studies on the problem that we identified.
After a cause and effect analysis (Figure 1), we identified two main problems which were knowledge gaps amongst healthcare professionals in ICU and equipment issues pertaining to MDI connectors in the ventilatory circuit.
We conducted education sessions for healthcare professionals in the ICU on the proper use of MDIs in mechanically ventilated patients and introduced the use of the new inhaler connector RTC 24-V.
Our comparative study revealed that the new RTC 24-V inhaler connector does decrease the dose counter when actuated with little discrepancies between expected dose reduction and the dose counter change. On the contrary, when the 22M-22F inhaler connector was used, there was a big difference in expected dose reduction and the dose counter change (Figure 5). The small reduction in the dose counter might be due to priming of the Seretide™ Evohaler prior to actuation in the ventilatory circuit.
The QI team felt that this was very important clinically as there would be potential patient safety issues. Firstly, as the dose counter did not register a drop in number when using with 22M-22F inhaler connector, we will not be sure if the actual intended dose of medication was delivered thus impacting on accuracy of delivery. There might be discrepancies in the dose counter readings and the actual doses of medications left in the canister. This might lead to subsequent patient safety issues, if the patient continues to use the inhaler after extubation when there are actually no medications left in the canister despite the dose counter showing otherwise. As the new RTC 24-V changes its dose counter with every actuation, we will be confident of the accuracy of dose delivery and be able to trust the dose counter on the remaining doses. The small discrepancy in the dose counter in the RTC 24-V arm is postulated to be due to variability on the first and last day of the ICU stay as admission and discharge timing could affect the total number of doses delivered on those 2 days.
Apart from the clinical safety aspect, the healthcare professionals in our ICU found the new RTC 24-V connector to have a tighter fit to the ventilator circuit. Previously, when the 22M-22F connector were used, the inhaler connector will be removed once the inhaler is administered as the connection to the ventilatory circuit is quite loose and accidental disconnections have been documented. With the RTC 24-V connector, it can be left in the inhalation limb of the ventilator circuit and used whenever it’s required. Despite leaving the connector in the circuit for the entire period of mechanical ventilation, no accidental disconnections were found during the study period. Additionally, the RTC 24-V connector does not add to apparatus dead space of the ventilator circuit as it is placed beyond the Y-piece of the breathing circuit. 10 As the RTC 24V is left in circuit throughout the period of mechanical ventilation, there will be less disconnections which might contribute to decreasing ventilator associated infections as well as making the administration of inhalers easier.
The survey done pre and post study also revealed an increase in confidence of the ICU healthcare professionals when using the RTC 24-V (Figure 6). Significantly fewer healthcare professionals found issues with the administration of inhalers using the RTC 24-V and a great majority of them preferred the RTC 24-V over the existing 22M-22F inhaler connector. Usage of the new RTC 24-V not only addressed the patient safety aspect of inaccurate dose reflection and dose delivery, but it has increased the confidence level of healthcare professionals in the administering of MDIs in the ICU.
Compatible inhalers and connectors should be used for mechanically ventilated patients. There was an advisory from New South Wales, Australia that certain inhaler connectors do not activate the dose counter of salbutamol MDIs (with dose counters) and it did mention the same connector as in our study, inhaler connector 22M-22F. 11 They advised that assessments be conducted to determine the most appropriate MDI adapter for the ventilation circuit.
We reviewed the inhalers available in our hospital and found that the only LABA/ICS MDI with in-built dose counter that is compatible with RTC-24V inhaler connector was Seretide™ Evohaler. The dose counter of the other LABA/ICS MDI will not change when actuated using the RTC 24-V inhaler connector. We have thus mandated that apart from MDIs without dose counter, which will include salbutamol, ipratropium bromide and inhaled corticosteroids, only Seretide™ Evohaler can be administered in mechanically ventilated patients.
As more inhalers with different modalities of delivery are introduced, our team will continue to evaluate and ensure appropriate inhaler connectors are used. One possible future evaluation will be a connector for Respimat® devices. 12 This will enable the delivery of long acting muscarinic antagonist (LAMA) to mechanically ventilated patients.
Sustainability
In view of the above findings, our team would like to propose an evaluation of all the inhaler connectors used in Intensive Care Units in Singapore. We recommend using appropriate ventilator circuit inhaler connectors that are compatible with the MDI and register accurately the dose delivered to the patient. We would also recommend using only inhalers that are compatible with these inhaler connectors. Knowledge gaps amongst healthcare professionals in the ICU should be addressed with educational programmes with respect to the administration of MDIs in mechanically ventilated patients.
Conclusion
The use of RTC 24-V inhaler connector demonstrated several advantages when compared with the 22M-22F inhaler connector. It was better for patient safety as it reflected more accurate dose delivery and was found to be sturdier when used in the ventilator circuit. It was also found to be well received and much preferred by our ICU healthcare professionals. Together with continued education to all staff on the appropriate use of MDIs and how to use the inhaler connectors, we hope that there will be an improvement in the effectiveness and accuracy of bronchodilator administration in the ICU. We will aim to continually reassess our practices and look for new compatible inhaler connectors as newer inhaler devices are introduced.
Footnotes
Acknowledgements
We thanked the department of ICU and Respiratory medicine for helping us with the study. We also thanked the nurse whom discovered this issue.
Author contributions
The QI team was led by Dr. QH J Ye and consisted of APN Toh HP, Sis LM Nathan, Ms A Cunanan, Ms QW Leo and Dr. K Sharma. Dr. HY J Tan supported as the head of respiratory medicine and with editing. Dr. G Kalyanasundaram helped with literature search and the writing of the paper.
Declaration of conflicting interests
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated and analysed during the current study are available.