
Abstract
Background
Children commonly present at the emergency department with abdominal pain and it is challenging to identify urgent surgical conditions. An audit conducted at a tertiary children’s hospital showed that 70% of patients admitted to Department of Pediatric Surgery (PAS) for abdominal pain had non-surgical diagnoses and wide variation in management.
Objective
Our quality improvement (QI) project aimed to reduce length of stay (LOS) and unnecessary investigations performed for patients admitted to PAS with abdominal pain, without causing complications or delayed diagnosis of surgical conditions.
Methods
The QI project consists of a standardised management workflow with stringent discharge criteria. We reviewed outcome measures of LOS, number of investigations ordered, compliance to workflow and readmission within 1-week post discharge at the end of each Plan-Do- Study-Act (PDSA) cycle and iteratively improved the workflow following QI principles.
Results
61% of patients were admitted to PAS for non-surgical abdominal pain throughout three PDSA cycles conducted. The third cycle showed improved compliance to workflow (80.7%) with reduced median LOS by 1 day, reduced median number of blood, stool and urine investigations by 1 and reduced range of investigations ordered. Readmission and CE attendance rate 1 week after discharge was 1.6% (n = 3), which was comparable to audit at 2.3% (n = 4), p = 0.709.
Conclusion
The workflow reduced LOS, number of unnecessary investigations and variability in investigations ordered, without causing misdiagnosis. It improved patient experience with sizeable cost savings for the patient and the hospital. QI projects can improve patient outcomes by introducing standard protocols that aid clinical management.
Introduction
Abdominal pain is a very common complaint that accounts for approximately 5–10% of visits to pediatric emergency departments and frequent admissions to the hospital.1,2 The most common diagnoses are non-surgical conditions such as non-specific abdominal pain (40%), constipation (22%) and viral infections (13%). 3 Due to the undifferentiated presentation, it is challenging for clinicians to exclude urgent surgical conditions that require operative treatment. Diagnosis is more difficult in children compared to adults since pediatric cognitive and psychosocial development limit the information gained from history and physical examination. Clinicians try to avoid ordering potentially painful laboratory tests or imaging with radiation exposure. Hence, may choose to monitor for evolution of symptoms and signs during a period of observation. There are no established guidelines for diagnostic workup of pediatric abdominal pain which contributes to different clinician’s practices.
A baseline audit conducted in November/December 2019 at a tertiary children hospital showed that 70% of patients with abdominal pain admitted to department of pediatric surgery (PAS) from the hospital’s children’s emergency (CE) had non-surgical, non-urgent diagnoses. There was a wide variation in length of stay (LOS) and number of investigations performed during hospitalization amongst patients with the same diagnosis at hospital discharge.
After initial evaluation at CE, children with abdominal pain are admitted under PAS if there are concerns of possible surgical conditions that require urgent intervention. However, on admission, it is the minority of patients who have clear-cut surgical conditions that undergo operative treatment; most will require a variable period of monitoring and investigations until the diagnosis can be established. Diagnosis is challenging due to the overlap of presenting symptoms among different conditions; hence, patients may be hospitalized for a prolonged period of observation. This results in additional costs for patients and impacts on the utilization of hospital resources i.e., manpower, occupancy of hospital beds.
Our audit highlighted that junior rotating doctors tended to order investigations that are considered routine in adult patients. For children, blood taking and urine collection for tests may be distressing. In addition, collection of urine or stool specimens is time consuming for caregivers and nurses but has low diagnostic yield. 4
To address these problems, we embarked on a quality improvement (QI) project aiming to reduce LOS and unnecessary laboratory and radiological investigations for pediatric patients with abdominal pain admitted to PAS.
Method
We applied the 3-step QI model to understand the current situation, derive the root causes of problems before proposing possible solutions, using data to verify findings.
The target study population were paediatric patients admitted to PAS from CE with abdominal pain, whose final diagnoses were “non-surgical” conditions (e.g., gastroenteritis) or surgical but “non-urgent” conditions that could be managed as outpatient (e.g., constipation). The exclusion criteria were patients who were diagnosed with surgical conditions that required urgent intervention (e.g., appendicitis).
Data were collected from hospital’s electronic medical record system (LOS, number of investigations ordered and/or readmission if any). Compliance to workflow was evaluated by team members who read through the patients’ daily clinical notes (“Admission Notes” and “Inpatient Progress Notes”) that were documented in the electronic medical record system.
The outcomes studied were LOS, Number of Blood, Stool, Urine Investigations Ordered per Patient, Number of Radiological Investigations Ordered per Patient, Compliance to workflow, Readmission and CE reattendance rate within a week after primary discharge and Financial Savings.
Data was entered into a spreadsheet (Microsoft Excel) and analysed using the same software. Tests for statistical significance included chi-square test for categorical data and Mann-Whitney U test for continuous data. p value of <0.05 was considered statistically significant.
Baseline measurement
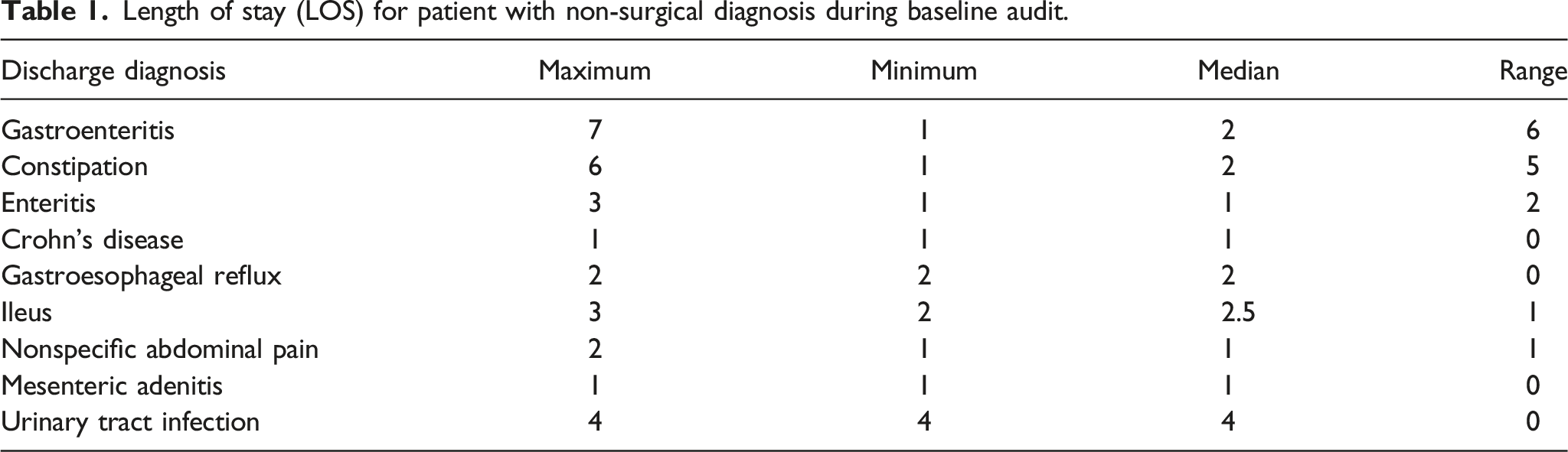
Length of stay (LOS) for patient with non-surgical diagnosis during baseline audit.
Number of blood, urine & stool investigations ordered for patient with non-surgical diagnosis during baseline audit.

Number of radiological investigations ordered for patient with non-surgical diagnosis during baseline audit.

In addition, the total number of non-surgical patients readmitted to the hospital within a week after the primary discharge was 2.4% (n = 4). Out of which, one patient was subsequently diagnosed with a surgical cause of malrotation with volvulus.
Identification and verification of possible cause for problems/opportunities
We conducted root cause analysis that identified the problems of (a) diagnostic difficulty, due to the wide variety of possible clinical conditions and (b) different clinician practices, affected by the clinician’s experience and risk tolerance. This suggested that there was opportunity to improve outcomes by introducing a standardized diagnostic and management protocol.
However, literature review showed that there was no established guideline for diagnostic workup of paediatric patients with undifferentiated abdominal pain. We consulted various stakeholders (senior and junior staff in PAS and Nursing) to create a workflow to guide management (Figure 1). The workflow accommodated hospital resource constraints and recommended the duration of observation, type and timing of investigations to order, according to the clinical presentation. It included new patient safety protocols to reduce risk of misdiagnosis (i.e., strict discharge criteria, caregiver information brochure with return advice and easy access to early outpatient review). Standardised department workflow for patients admitted with abdominal pain.
Quality improvement implementation
A QI study was conducted with three Plan-Do-Study-Act (PDSA) cycles from September 2020 to September 2021. The 5-member QI team comprised a pediatric surgical fellow, an Advanced practice nurse, a Research coordinator, a pediatric surgical consultant, and a QI Advisor.
Results
First PDSA cycle: Testing the new workflow
After designing the abdominal pain management algorithm, it was shared with all PAS doctors and their concerns addressed. Additional briefing sessions were conducted for rotating junior doctors and pediatric ward nurses to ensure all were educated on the new workflow before starting the QI project in September 2020.
Overview of patients admitted with abdominal pain.

The team amended the workflow to emphasize clinical assessment and earlier feed resumption without scans if there was low suspicion of surgical condition. The team arranged additional briefing sessions by Zoom to allow better attendance of junior doctors. A softcopy of the workflow was made available, and reminders sent on the junior doctors group chat.
Second PDSA cycle: Improved abdominal pain workflow and junior doctor training
After incorporating feedback and changes, the second PDSA cycle was run in November 2020. During this cycle, 95 patients were admitted with abdominal pain and 54 (57%) patients had non-surgical diagnoses (Table 4). There was minimal change in outcomes of LOS and investigations ordered. We noted that compliance to workflow remained low at 68.5%. Although more briefing sessions were arranged for junior doctors, some missed it due to heavy workload and call schedules.
We decided to change the timing of the briefing session; it was now the compulsory department orientation for all junior doctors start of rotation. The session duration was reduced to 15 min with detailed slides emailed for reference.
Third PDSA cycle: Measuring sustainability and effectiveness of the workflow and training
The third PDSA cycle was carried out from July 2021 to September 2021.During this cycle, 125 patients were admitted with abdominal pain and 83 (66%) patients had non-surgical diagnoses (Table 4), p = 0.07%. There was full attendance of the briefing session. The compliance with the workflow improved from 37.5% (first cycle) to 80.7% (third cycle).
There was improvement in all outcomes of interest over the baseline audit, by the third PDSA cycle of the QI project:
The median LOS reduced from 2 (range 1–7) before QI to 1 (range 0–5) after QI p < 0.001 (Figure 2). The number of blood, urine and stool investigations ordered reduced from median of 5 (range 0–11) before QI to 4 (range 0–8) after QI p < 0.001 (Figure 3). There was no reduction in the number of radiological investigations ordered but there was less variability with narrower range - median 1 (range 0–5) before QI to 1 (0–3) after QI p < 0.001 (Figure 4). Length of stay (days) per patient. Number of blood, urine & stool investigations ordered per patient. Number of radiological investigations ordered per patient.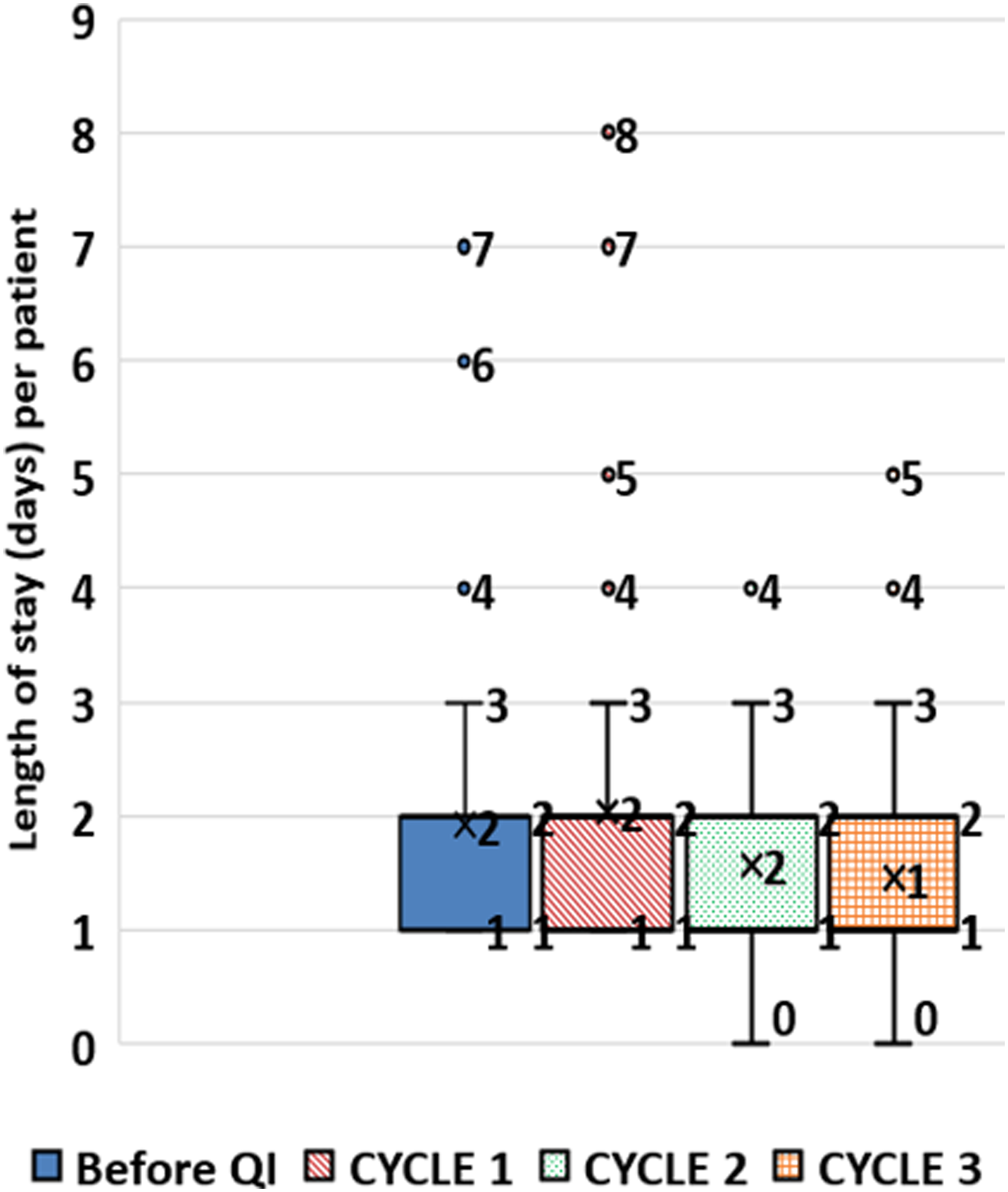


During 3 PDSA cycles conducted, 313 patients were admitted to PAS with abdominal pain of whom 193 (61%) had non-surgical diagnosis: 56 (60.2%) in 1st cycle; 54 (57%) in 2nd cycle; 83 (66%) in 3rd cycle. The total number of non-surgical patients readmitted to the hospital or re-attending CE within a week after the primary discharge was 1.6% (n = 3). This rate was similar to baseline audit at 2.4% (n = 4), p = 0.709. All the readmitted patients during PDSA cycles were subsequently discharged with non-surgical diagnoses.
Discussion
Our standardised workflow improved LOS and reduced unnecessary investigations by reducing variation in clinical practice without introducing patient morbidity. The workflow guided inexperienced junior doctors faced with clinical uncertainty to make decisions and helped them rely less on unnecessary investigations.
Participating in QI activities empowers clinicians to make changes in their healthcare system that improves care for their patients. 5 Our QI project improved patient experience by reducing hospital stay and reducing the number of unpleasant tests. The patient also pays less. The cost savings for reduced number of investigations ordered (from 5 to 4) and reduced LOS (from 2 days to 1) adds up to approximately 678 SGD per patient, at hospital full charges rate in 2022. Given the hospital average of 2016 patients per year admitted to PAS with non-surgical/non-urgent abdominal pain, this translates to annual cost savings of approximately 1,366,848 SGD. Due to our public hospital setting with partially subsidised healthcare, this results in sizeable taxpayer savings.
A major challenge faced by the QI team was that frequent rotation changes of junior doctors affected compliance to the workflow. It required adjustment of briefing session to accommodate work schedules, providing electronic reminders and references to effect change in behaviour. Another challenge was junior doctors’ documentation as it affected data collection about compliance. The team sought to overcome incomplete documentation by triangulation with other electronic medical records such as nursing notes and timestamping of investigation orders.
Stakeholders buy-in is crucial at all stages of QI. 5 Before implementation, some PAS seniors were worried about missing surgical diagnoses with the proposed management algorithm, so the team created additional safeguards of strict discharge criteria, return advice brochures for caregivers and simplified patient access to get early outpatient PAS reviews. The QI audit confirmed that no patient had delayed diagnosis nor was readmitted for surgical condition within 1 week after their initial hospitalisation discharge. This has reaffirmed departmental support for this workflow.
The next aim for our QI team is to further reduce unnecessary investigations. During the QI audit, we found that urine culture tests although frequently ordered, have shown low yields for patients without urinary symptoms. This finding is shared as part of workflow training sessions to enhance compliance to workflow.
Conclusion
Our standardised management workflow tailored to our context reduced LOS, number of unnecessary investigations and the variability in investigations ordered, without causing misdiagnosis. It has improved patient experience with cost savings for the patient and the hospital. QI projects can improve patient outcomes by introducing standard protocols that aid clinical management.
Footnotes
Acknowledgements
We would like to thank the department of paediatric surgery and nursing team for adhering to the implemented changes. Special thanks to Mr John Wong Chi Keong for guiding us in the application of the Quality Improvement P-D-S-A Cycle model in our project.
Author contributions
HA developed the workflow with HL under the mentorship of CO. All the authors were involved in the implementation of the project. HA, HL, CSC and CO analysed the data. HL wrote the first draft of this manuscript. All authors reviewed, edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
According to institution guidelines, a formal application for ethical approval is not applicable as this study was a quality-improvement project.
Informed consent
According to institution guidelines, informed consent was not sought for the present study because this is a quality-improvement study and only anonymised patient data were collected.
Availability of data and materials
The datasets generated and/or analysed during the current study are available from corresponding author.