
Abstract
A giant inguinoscrotal hernia is typically associated with a low risk of bowel obstruction or strangulation. When the hernia is complicated with acute gastric perforation, it is an exceedingly rare clinical entity. The operative strategy may be definitive at the index surgery or staged. The technical challenge is the severity of the peritoneal contamination contradicting mesh placement, coupled with the loss of domain. Herein we report a 58-year-old man with a long-standing right giant inguinoscrotal hernia, who presented with strangulation with a 1 day history. An urgent midline laparotomy access revealed a large tear over the lesser curvature of the stomach, attributable to choking at the hernia neck. Furthermore, there was severe contamination with total bowels herniation into the sac. We performed a complete reduction of hernia content, primary repair of stomach perforation, and primary closure of midline access and hernia neck repair with posterior wall reinforcement using prolene via an inguinal incision. The patient made an uneventful recovery and was discharged well. The perioperative clinical events and technical strategies are discussed in the current report.
Introduction
A giant inguinal hernia refers to an inguinal hernia that extends below the midpoint of the inner thigh when the patient is in a standing position. 1 It may commonly present with large groin swelling with discomfort, rather than with acute complications such as strangulation or organ perforation, due to its large neck. The operative difficulties in this entity are mainly due to the loss of domain and sequelae of abdominal compartment syndrome (ACS), which can be devastating. 2 In the current case, we described a male with acute strangulation of giant inguinal scrotal hernia with choked gastric perforation, which was successfully operated by an acute care surgeon. We adopted a single-stage procedure and planned a relook with a slow weaning strategy. A detailed description of the clinical course and operative steps are discussed in the report, with a comparison appraisal of previously reported cases.
Case presentation
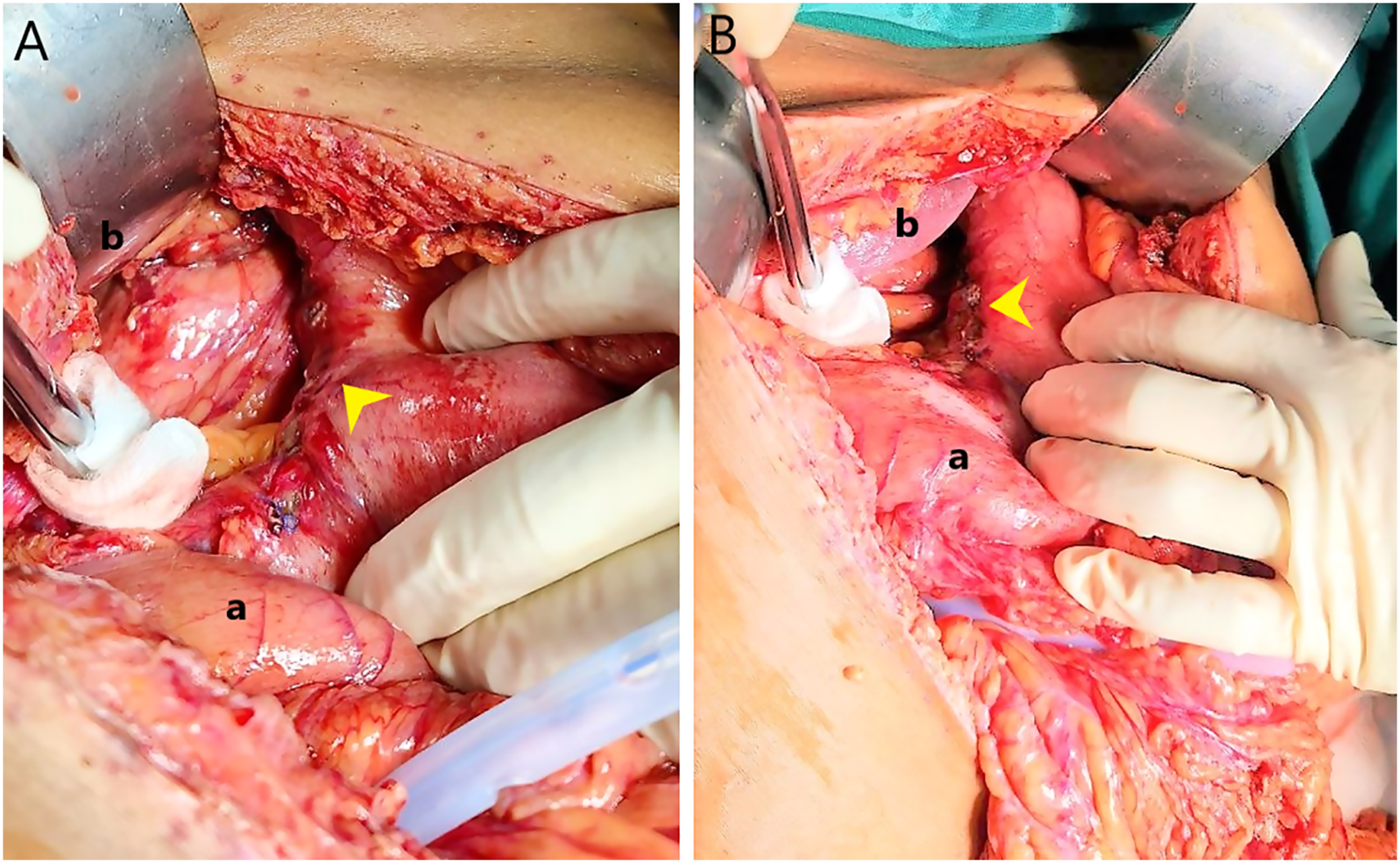
A 58-year-old male visited the emergency department and presented with sudden severe abdominal pain, nausea and vomiting for 1 day. He had a long-standing right inguinoscrotal hernia for over 20 years, which he refused to repair since it was asymptomatic. He was in pain and tachycardic, with a heart rate of 110 bpm, but normotensive. His abdomen was tender but not distended. There was a giant right inguinoscrotal hernia extended up to the lower third of the thigh, with erythematous shiny scrotal skin (Figure 1). Blood investigation showed leucocytosis and metabolic acidosis with acute kidney failure. An erect plain chest radiography revealed air under the diaphragm (Figure 1). Following fluid resuscitation and broad-spectrum antibiotics, emergency surgery was performed with initial access via a midline laparotomy. There was massive gastric content contamination from an 8 cm tear along the lesser curvature of the stomach (Figure 2). The right-sided colon and entire small bowels were trapped within the scrotal hernia sac. The gastric perforation was seen to be choked at the hernia neck. The edge of the stomach wall at the perforation site was unhealthy with slough. Following the reduction of bowels from the hernia sac and mobilization of the stomach, a primary repair of the lesser curve perforation was performed with a monofilament double-layered suture. The hernia defect was repaired from an inguinal incision with prolene suture plication for reinforcement. A midline fascial closure was achievable without tension, despite bowel reduction into the peritoneum, as the groin hernia was large and tense due to gastric content pooling, and together with adequate abdominal muscle paralysis (Figure 3). Postoperatively, a joint discussion with the anesthetist team led to the decision of gradual weaning and a planned relook laparotomy to check the stomach repair due to the extent of initial contamination and the unusual site of gastric perforation with the concern of vascularity at the repair site, A fluid restrictive together with multimodal strategies were done to avoid the occurrence of abdominal compartment syndrome, and if it happened, we need to identify it early. He had an uneventful planned relook at 72 h, and was extubated after a week in the ICU. He was discharged well on day 10, though complicated with nosocomial sepsis. (a) A giant right inguinoscrotal hernia extended up to his lower third of the thigh with erythematous shiny scrotal skin. (b) Erect plain chest radiography revealed air under the diaphragm (arrowhead). Intraoperative photo (a, b) revealed a linear tear along the lesser curvature of the stomach with primary repair done (arrowhead). a: transverse colon; b: liver. Abdominal closure achieved without tension.

Discussion
A giant inguinoscrotal hernia presenting to an outpatient clinic is technically easier to handle, as peri-operative strategies can be preplanned. In the current case of gastric perforation, the operative procedures were complicated due to severe contamination, septic shock, and loss of domain. A previous case reported that a two-step approach in which the hernia was repaired after a second surgery has resulted in less morbidity and mortality. 2 Contrary to that, we repaired the hernia during the first surgery, together with the stomach repair. He had a good recovery and both the stomach repair and hernia defect could be reassessed when a planned relook was performed.
A search of the literature only identified two other similar cases with gastric perforation in a giant hernia.2,3 It was reported this was due to the downward pulling force exerted by the heavy hernia content. 2 Both cases were operated in a two-staged manner. One of the cases involved a distal gastrectomy rather than primary repair. Both patients had a full recovery.2,3
Due to the large size of the groin hernia and sac, excision of a portion of the indirect sac may be necessary to prevent seroma formation and recurrence. However, exploring the sac during the procedure may result in contamination. While there is evidence supporting the use of mesh in a clean-contaminated surgical field, 4 the author opted for a fascia repair with prolene sutures to avoid the risk of mesh infection.
The chronic loss of domain may contribute to intra-abdominal hypertension or ACS, and this is associated with high mortality and morbidity rates. 2 Reducing the hernia content back to the peritoneal cavity and post-surgery ileus can cause an increase in intra-abdominal and intra-thoracic pressure, leading to cardiopulmonary compromise, renal dysfunction, and cerebral or gastrointestinal dysfunction hypoperfusion. 5 In the current case, we opted to reduce the hernia content completely and repair the abdominal wall and hernia defect in the same setting, as we predict the risk of an abdominal compartment would be low due to a false giant hernia as a result of gastric fluid pooling. The patient had a slow weaning with adequate sedation in order to improve abdominal wall compliance, hence avoid the rise of intra-abdominal pressure. Besides, we adopted multimodal measures following guidelines from the world society of abdominal compartment syndrome. 4 Intraluminal contents is evacuated by using a nasogastric tube, and at the same time, early initiation of parenteral feeding while enteral feeding is minimized in the acute stage. Furthermore, adequate sedation and analgesia are provided to improve abdominal wall compliance, concomitantly with judicious and goal-directed fluid resuscitation. 4 The planned relook laparotomy allows a complete assessment of the stomach repair, hernia defect and the return of normal bowel quality from oedema.
Conclusion
Emergency repair of a giant inguinal hernia complicated with gastric perforation may be performed in a single-stage setting (i.e. repair of gastric perforation, together with the hernia repair), with no adverse outcome. If in doubt, a two-step approach (i.e. repair hernia during the second surgery) is a good bail-out option to avoid mortality from abdominal compartment syndrome.
Footnotes
Acknowledgements
We would like to thank all the efforts provided by general surgery team and ICU team from Hospital Sultanah Aminah, Johor Bahru.
Author contributions
Jun Sen Chuah wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Hospital Sultanah Aminah Johor Bahru does not require ethical approval to case report because standard management was given to patient, written consent was obtained from patient, and this case is not included in any clinical trials.
Informed Consent
Written informed consent was obtained from the patient(s) for their anonymised information to be published in this article.
Availability of data
Data sharing is not applicable to this article as no datasets were generated or analysed during the current study.