
Abstract
Background
With improved survival among People Living with HIV (PLHIV), many are confronted with age associated comorbidities and geriatric syndromes. Neurocognitive impairment is one of the three most frequent conditions that affects quality of life of PLHIV despite achieving viral suppression. Healthcare providers face challenges in early identification of neurocognitive impairment, performing comprehensive assessment and managing older PLHIV.
Objectives
This paper aims to review available evidence regarding aetiology and management of older PLHIV who develop neurocognitive impairment, suggest improvements on current management and postulate future study direction.
Methods
A PubMed search for original articles and Clinical Guidelines was conducted from September 2021 to August 2022 using a combination of keywords related to neurocognitive impairment in PLHIV. The citations from all selected articles were reviewed for additional studies.
Results
Older PLHIV tend to be frailer than their uninfected counterparts, are plagued with multi-morbidity and are at increased risk of cognitive impairment. The aetiologies for neurocognitive impairment are multifactorial, multi-dimensional and complex. The management of neurocognitive impairment in older PLHIV involves identifying and optimizing predisposing factors, physical function, social and psychological health with appropriate care navigation.
Conclusion
Identification and management of neurocognitive impairment in older PLHIV through interdisciplinary collaboration among stakeholders is important. This exemplifies an integrated model of care for older PLHIV and promotes the notion of living well beyond viral suppression.
Keywords
Introduction
HIV remains a global public health issue with an estimate of 38.4 million People Living with HIV (PLHIV) today. 1 Effective combination antiretroviral therapy (cART) has transformed the care of PLHIV to that of a chronic condition, with a notable global demographic shift in the epidemiology of HIV including Singapore.2,3 The number of older PLHIV, aged 50 years and above is increasing. In the United States of America (USA), the prevalence of older PLHIV has increased from 17.4% in 2001 to 36.2% in 2010, and is estimated to reach 75% by 2030. 4 Likewise, in Singapore, its prevalence has increased from 18.1% in 2002 to 26.9% in 2021.5,6
The Joint United Nations Programme on HIV/AIDS 2020 90-90-90 sets the targets for 90% of PLHIV to be aware of their status, of which 90% to receive treatment and 90% of this same population to be virally suppressed. In addition, a good health related quality of life (QOL) among PLHIV is critical beyond viral suppression. PLHIV encounter many non-communicable diseases – including diabetes, hypertension, dyslipidaemia, chronic kidney disease, malignancy, and dementia, at a higher rate and at an earlier age compared to their non-infected counterparts. 7 Observational studies have estimated that the prevalence of select age-related comorbidities among PLHIV approaches that seen among people without HIV infection who are 5 years older, and the risk of multi-morbidity for these patients is similar to that of people without HIV infection who are 10–15 years older.8–10 Likewise, in a study of older PLHIV versus age-matched non-HIV individuals, Onen et al. found higher prevalence of hypertension, hypertriglyceridemia, lipodystrophy, and low BMD in PLHIV, which suggest that these co-morbidities are associated with HIV and treatment-related factors, and are not part of “normal” ageing. 11 Therefore, a “4th 90” which aims for 90% of all PLHIV to have a good health-related QOL is being advocated. 12
One of the commonest geriatric syndromes that plagued older PLHIV and undermines their QOL is neurocognitive impairment. A USA study reported that PLHIV are at increased risk of dementia by 58% despite receiving antiretroviral therapy (ART), and were diagnosed with dementia at an average age of 67 years compared to 78 years in those without HIV.13,14 Among PLHIV with dementia, 91% had undetectable viral load at time of dementia diagnosis. 14 Furthermore, in the AIDS Clinical Trials Group Longitudinal Linked Randomised Trials study, approximately 26% of subjects were found to be cognitively impaired at their baseline neuro-screen. 7 Therefore, neurocognitive impairment in PLHIV is a common yet under-recognised problem. Many factors contribute to neurocognitive impairment other than HIV infection alone, where the average age used for screening in the general population may not apply. Similarly, medical practitioners caring for older PLHIV may not be trained to assess nor manage specific needs of this geriatric syndrome, nor are geriatricians familiar with care of older PLHIV.
In this review article, we categorise and discuss aetiologies for neurocognitive impairment in older PLHIV to provide greater clarity on this complex, multifactorial and multidimensional geriatric syndrome that plagued this vulnerable population. In addition, we highlight aspects and challenges in the management of HIV and neurocognitive impairment, and the need for inter-discipline collaboration to provide integrated comprehensive care for individuals ageing with HIV. 15
Neurocognitive impairment impedes quality of life
Although there are many factors that affects health related QOL of PLHIV, neurocognitive impairment is like “a fog that impacts everything”. 16 Together with its associated behaviour and psychological symptoms, neurocognitive impairment impedes one’s ability to self-care and manage instrumental activities of daily living. Subsequently it affects one’s physical and mental health, self-awareness, and self-control, and thereby reduces social connectedness. Therefore, it becomes very challenging for PLHIV to maintain employment, manage chronic medical conditions and medications. The problem is compounded with the lack of comprehensive care to meet the needs of PLHIV, resulting in poorer quality of care and health outcomes.
Aetiologies for neurocognitive impairment in older PLHIV
The aetiologies for neurocognitive impairment in older PLHIV are multi-factorial, multi-dimensional and complex (Figure 1). Potential mechanisms behind HIV-related Central Nervous System (CNS) injury have been proposed - (a) legacy effect of CNS impairment prior to cART initiation, (b) limited blood brain barrier penetration of cART drugs versus CNS Neurotoxicity of cART, (c) interaction between chronic HIV and ageing resulting in worsening inflammation, and immune activation that increases vascular disease burden and neurodegeneration, (d) co-morbidities among HIV-infected populations such as substance abuse, hepatitis C virus co-infection, mood disorders, vascular risk factors (e) persistent low levels of HIV in CNS and (f) ongoing immuno-inflammatory responses.18–20 In addition, among the co-morbidities, neurodegenerative diseases need to be considered, such as cerebral small vessel disease, vascular dementia, Alzheimer’s disease (AD), and dementia with Lewy bodies.
21

The aetiologies for neurocognitive impairment in PLHIV can be classified into (i) HIV-related factors and (ii) Individual related factors. The vulnerability of PLHIV to cognitive impairment is demonstrated in Figure 1.17,55,78
HIV related factors
HIV-Associated Neurocognitive Disorder
HIV-associated Neurocognitive Disorder (HAND) is a common cause of cognitive impairment in PLHIV. 22 HAND is diagnosed after excluding pre-existing neurobehavioral pathologies or strong confounding conditions that may affect PLHIV. 23 There are three stages of cognitive impairment namely asymptomatic neurocognitive impairment, mild neurocognitive disorder and HIV-associated dementia. 24
The pathogenesis of HAND remains incompletely understood due to the diagnostic complexity and highly variable phenotype. 25 However, HAND is likely a result of HIV entering the CNS during infection, persisting and replicating in resident immune and supporting cells, and activating host immune response and inflammation which causes cell injury. 25 Despite peripheral viral suppression from cART, chronic inflammation and viral replication in the CNS can disrupt the endothelial barrier and neuronal pathways, resulting in milder form of HAND. 26 Difference in host genetics can also alter the effectiveness of immune response and other factors, increasing the vulnerability to HAND.
HCV Co-infection, and HIV-associated CNS opportunistic infection and malignancy
HIV-associated CNS opportunistic infections (for instance, toxoplasmosis, cryptococcosis) and malignancy, as well as HCV coinfection can induce neurocognitive impairment. A recent study in Brazil revealed that individuals with HIV and HCV coinfection had highest percentage of global neuropsychological impairment in the following cognitive ability domains – executive function, processing speed, fluency, and motor.27,28
Antiretroviral therapy
Effective cART can indirectly contribute to cognitive decline via worsening hyperglycaemia, hyperlipidaemia, and hypertension, and causing cardiomyopathy, resulting in cardiovascular and cerebrovascular events.29,30 It is hard to distinguish the deleterious effects of HIV from the neurotoxic adverse effects of cART, ranging from peripheral neuropathy to neuropsychiatric and neurocognitive deficits in the CNS.31,32
An Overview of ART classes, Mechanism of action and Individualisation of ART regimen. 37

Individual related factors
Age-associated cognitive decline
The brain undergoes age-associated structural changes, with gradual atrophy in brain volumes that accelerates in old age. 38 Greater grey matter atrophy and cortical thinning occur earlier in life, whereas steeper decline in brain white matter sets in later in life at age 70. 38 Nonetheless, age-associated cognitive decline is best considered and understood using the life course approach, where the effect of early life biological, behavioural, social and psychological exposures poses risk for developing the disease state and increase rate of neurodegeneration.
Cognitive ageing with HIV
Chronic low-grade inflammation is characteristic of both ageing and HIV disease. In PLHIV, persistent inflammation and systemic immune activation cause premature ageing by driving excess activation and proliferation of T cells, leading to telomere shortening, oxidative stress and immune-senescence with resultant age-related co-morbidities. 39 Therefore, chronic inflammation in the CNS which is mediated through residual viral replication, dysregulation of infected cells, continuous production of viral proteins, and positive feedback loops of chronic inflammation results in brain injury. 40 Moreover, persistent inflammation and immune activation is enhanced by sustained chronic antigenic stimulation from low level viremia and viral protein released from reservoirs, antiretroviral treatment, coinfections by persistent pathogens including CMV, hepatitis B and C virus, and environmental factors – namely, central fat accumulation with resultant inflammatory cytokine production by expanded adipose tissue and smoking. 39 The interaction between ageing and HIV disease translates to earlier manifestation and higher frequency of geriatric syndromes – of note multi-morbidity, neurocognitive impairment, polypharmacy, and frailty – which is not usually seen in non-HIV individuals until later in life. Neurocognitive impairment when present reduces function and QOL.15,41
Other chronic medical conditions
PLHIV have an increased number of age-associated chronic medical conditions relative to those without HIV as seen in Figure 1.29,30 The Veteran Ageing Cohort Study in PLHIV showed a 1.17-times increased risk of stroke at all ages despite viral suppression. 42 Age-associated co-morbidities, namely visual and hearing impairment, neurodegenerative diseases, falls with traumatic brain injury kidney disease, cerebrovascular disease, coronary heart disease (CHD), and their risk factors may compromise normal cognitive functioning.30,32,43 CHD and its vascular risk factors also predisposes PLHIV to cognitive impairment via systemic atherosclerosis and cerebral hypo-perfusion, due to impaired cardiac function or infarcts from cardiogenic emboli to the brain. 44
Sleep disorders
There is higher prevalence of sleep issues among PLHIV up to 73% as compared to 30% of the general population, with symptoms including poor sleep quality, daytime somnolence, and fatigue. 45 Sleep disturbances (poor sleep quality, quantity and or sleep disordered breathing) have been associated with cognitive impairment and the co-occurrence of sleep disturbance with dementia may lead to a more rapid decline. 46 Furthermore, sleep disturbances impact QOL, increases risk of cardiovascular and metabolic diseases as well as neurodegeneration and cerebrovascular pathology. 47 Obstructive sleep apnoea, the commoner clinical sleep disorder, is associated with up to six times greater risk of neurocognitive disorder regardless of retroviral status. Despite the high prevalence among PLHIV and its significant morbidity, sleep disorders tend to be underdiagnosed. 48 Furthermore, co-existing depression and polypharmacy, both common among PLHIV, may drive the above associations between sleep and cognitive impairment.46,49 Therefore, sleep disorders, depression and polypharmacy should be sought and treated during follow up to prevent further cognitive decline.
Polypharmacy
Among PLHIV aged ≥65 years old, the prevalence of polypharmacy increases with age and duration of HIV infection.41,50 Polypharmacy increases the risk of drug-drug interactions and adverse effects that may cause cognitive injury. For instance, usage of anticholinergic drugs (e.g. amitriptyline, chlorpromazine) to treat comorbidities in PLHIV is associated with reduce brain volumes and microstructural integrity, thereby resulting in poorer cognitive functioning. 51
Using Medichec, an online tool to evaluate the anticholinergic effect of drugs on cognition can improve the safety and quality of prescribing medications in older PLHIV. Medichec informs clinicians on the choice of medicines and any changes which may result in cognitive impairment in older people, along with the size of the effect for different medicines individually and in combination.17,52
Substance use and mental health disorder
Substance use (including nicotine, alcohol, cocaine, and amphetamines) and mental health disorders like depression, anxiety and psychosis are common among older PLHIV, who face significant stigma, fear of rejection by family and friends, disease and death, financial insecurity, and dependence.53,54 As these disorders affect cognitive functioning, and increase non-adherence to medication and suicide rates, they should be addressed and treated early to achieve recovery or at least remission.
Social determinants of health
Social Determinants of Health (SDOH) are the conditions in which people are born, grow, live, learn, work and age.55,56 Although they are non-medical factors, SDOH affect and influence health and QOL outcomes.55,56 SDOH can be classified under the following categories of (a) Economic stability (based on socioeconomic status, employment, and food security, (b) Education level, (c) Health and health care, (d) Environmental factors (including access to food, quality education, physical activity and job opportunities, and healthcare, as well as safe housing without high risk of violence and trauma) and (e)) Social and community context. 57 These SDOH have a major impact on one’s health status, risk, behaviors, opportunities, patterns of social interaction, overall well-being, and QOL. The relationship between various SDOH and their effect on cognition are complex and highly interlinked, especially in PLHIV.17,55 For instance, malnutrition results in vitamin deficiencies which affects cognitive function across one’s lifespan.55,58
Furthermore, lower socioeconomic status, low levels of literacy and/or limited educational opportunity are associated with more rapid age-related cognitive and functional decline, and higher incidence of AD and related dementias – a possible contributing or confounding factor to the diagnosis of HAND.55,57 Likewise, early life adversity (childhood trauma) was also associated with higher risk of AD in later life.
59
However, higher number and levels of social engagement carries a protective effect towards the development of AD and related dementias in later life.
54
Therefore, as depicted in Figure 2, social connectedness promotes social and emotional resilience against cognitive decline. The 3P Framework for optimizing management of older people living with HIV who develop neurocognitive impairment during their life course. 
Management of neurocognitive impairment in older PLHIV
Caring for the older PLHIV with neurocognitive impairment is complex and these individuals would benefit from integrated clinical management. Principles of neurocognitive impairment management involve screening for cognitive decline, and accurate assessment, diagnosis and staging of cognitive decline which would guide goals of care and treatment. Following that, it is essential to identify predisposing factors as detailed above before drafting a patient centric treatment plan, to optimise management of reversible causes as well as chronic medical conditions and risk factors, by utilising both non-pharmacological and pharmacological management.
Non-pharmacological management would entail patient and caregiver education, post diagnostic support services (includes psycho-emotional and social support), and social prescription of behaviour and lifestyle changes to address various predisposing factors for neurocognitive impairment. This would include smoking cessation counselling and support with nicotine replacement therapy as well as prescribing cART with fewer side effects. Furthermore, a referral of patients to mindfulness training workshops and dementia day care may improve their overall well-being, facilitate cognitive stimulation, and enable meaningful social engagement.
Pharmacological management would include the use of cognitive enhancers and antidepressants to optimise the individual’s cognitive, behavioural, and psychological symptoms, overall QOL and care. Among commonly used cognitive enhancers for the treatment of alzheimer’s disease, Rivastigmine, an acetylcholinesterase inhibitor, has been shown to decrease brain damage in HIV patients with mild cognitive deficits. 60 However, Rivastigmine did not provide significant cognitive benefits among HIV patients with predominantly mild neurocognitive disorder, despite positive trends seen in the domains of information processing speed and executive functioning. 61 Therefore, further studies on acetylcholinesterase inhibitors and Memantine, an NMDA antagonist cognitive enhancer, are required to confer their effectiveness among this population. 62 Nonetheless, identifying the aetiologies of neurocognitive impairment specific to the individual will guide appropriate patient-specific pharmacological management.
In addition, early commencement of cART is key to protect brain health and cognitive reserve, as effective cART has been shown to reduce progression of mild neurocognitive disorder to HIV-associated dementia, and a change in antiretroviral regime may be considered in the presence of CNS viral escape. 17,63 Individualised cART regime from different pharmacological classes is essential to achieve viral suppression while minimizing adverse effects on comorbidities, improving medication adherence and overcoming drug resistance. 64 Nonetheless, polypharmacy should be minimised with the aim to improve medication compliance, reduce drug interactions and CNS side effects.
Current practice and challenges in Singapore
In current local practice, in addition to managing HIV disease and opportunistic infection, Infectious Disease (ID) physicians also perform annual screening of chronic diseases for older PLHIV and ensure appropriate vaccination in accordance with local and international guidelines. Referrals to cognitive specialist are made when PLHIV themselves, their families or physician, complain of cognitive difficulties. However, there are significant challenges in the management of neurocognitive impairment in the older PLHIV.
Firstly, it is challenging to integrate screening for neuro-cognition and psychiatric conditions, with limited consultation time and resources for the primary clinician. Secondly, aetiological factors as discussed above need to be assessed, which is also time consuming. Thirdly, older PLHIV are a unique population with multiple comorbidities and complex management issues. They tend to present with multiple geriatric syndromes, including impaired cognition and mental health, which complicates the management of any condition in this population. 65 These individuals would benefit from comprehensive assessments, referral to other services as required, case management, further health investigations and in-clinic advice. 66 Comprehensive assessment allows early identification of geriatric syndromes, clinicians to anticipate how patients will respond to environmental stressors and situational challenges, and direct necessary resources to support these vulnerable patients to age in place. 67
Finally, these issues that plagued this population is under-recognised among non-ID healthcare professionals. 15 This is due to the lack of awareness among medical and allied health professionals to understand HIV disease trajectory, frailty status and the experience of PLHIV as a chronic condition, and the complex challenges they face. Moreover, the ability to provide effective, efficacious, and seamless clinical care to ageing PLHIV with varying healthcare needs is impeded by a lack of interdisciplinary awareness cum collaboration, and a structured framework for an integrated care model. Therefore, more can be done for PLHIV with collaboration among physicians of various specialties and settings to optimise their QOL.
Strategies to overcome the challenges
In Singapore, there is a need to increase awareness among healthcare providers, allied health, community healthcare partners and policymakers about neurocognitive impairment, mental health and other common age-associated comorbidities that plagued older PLHIV. With increased awareness we could then rally stakeholders and policymakers to collaborate and develop nationwide initiatives and services that would mitigate the unique challenges faced by ageing PLHIV. Such collaboration facilitates integrated care, allows smoother transitions in care, and avoids or delays hospitalization and institutionalised care. Furthermore, interventions can be better designed around patient’s needs and resources and can be achieved through coordinated and collegial case discussions, in which different specialists contribute their own expertise and background. 68 Therefore, strong collaboration between healthcare disciplines across various settings (i.e., physicians, nurses, allied health professions and community partners) is essential to better evaluate individuals and improve health outcomes of this vulnerable population as a society. 68
Likewise, additional training and development of practice-based competencies to extend roles of nurses, allied health workers and specialists can help equip healthcare providers with the skills, knowledge and confidence to support care for ageing people with HIV. 69 The overall goal is to promote successful ageing for PLHIV–that is to support treatment adherence, health preservation and delay disease progression. Nonetheless, further work is required to develop referral criteria and pathways. In addition, the diagnostic processes and treatment offered should consider and address the multifactorial aetiology of neurocognitive impairment in PLHIV, for effective assessment and management.66,70
At present, studies on older PLHIV use an age threshold of 50 years and above as compared to 65 years and above for general population. This is backed by evidence of high prevalence of age-associated comorbidities among PLHIV from 50 years onward, that usually presents later in the general population and is in keeping with an accelerated ageing seen in PLHIV.8–10,14,71 Becker et al. found that PLHIV, above 50 years old has three-fold increased risk of developing cognitive disorder compared to HIV negative controls. 72 Therefore, after an initial diagnosis of HIV infection, patients aged 50 years and above should be screened for symptoms of cognitive associated with functional decline, preferably prior to starting ART to provide baseline data for longitudinal testing. 73 Alternatively, clinicians may screen for frailty to identify pre-frail/frail PLHIV for cognitive screening, as these individuals are at increased risk of neurocognitive impairment and worse health outcomes. 74
In theory, an interdisciplinary clinic for PLHIV can address the clinical, social, and psychological needs of PLHIV with progressive cognitive decline both seamlessly and efficiently, by providing assessment, management, and advice on care. The nurse assistant can conduct brief depression and cognitive screening with PLHIV, their family or caregivers, to determine if further cognitive or mental health assessment is required. Subsequently, corroborative history taking to evaluate for confounding conditions, such as substance use, CNS opportunistic infection or diseases, or mental health disorders, followed by a detailed cognitive assessment can be performed by a trained nurse clinician, using Montreal Cognitive Assessment (MoCA) prior to the cognitive specialist consult.63,75 Once the cognitive decline is deemed unrelated to confounding conditions or these are optimally managed, and the impairment still persists, objective neuropsychological examination should be carried out by the neuropsychologist. 63 Likewise, neurological examination cum MRI brain imaging will be evaluated by the cognitive specialist to characterise the neurocognitive impairment. 64 Cerebrospinal fluid assessment may be done to assess for CNS escape. 63 Thereafter, the diagnosis of neurocognitive impairment would be made upon fulfilling the Diagnostic Statistical Manual-5 Criteria for respective categories of neurocognitive disorders or the Frascati Criteria for HAND. 76 These cases will be discussed at inter-disciplinary meeting for further optimization with investigations and referral to other speciality services when required.
Over the course of one day, patients at the clinic would have had a comprehensive assessment by a team of HIV physician, HIV nurse clinician, dementia specialist, which will provide a diagnosis and develop a management plan. 60 The inter-disciplinary management approach is associated with improved outcomes that are gleaned from the comprehensive assessment and successful implementation of multifaceted, evidence-based, patient centred interventions. 67 These targeted interventions seek to optimise the individual’s medical issues, functional status, and social support, prevent more complex problems from developing, and empower patients to lead an improved QOL beyond viral suppression.
Figure 2 reflects our proposed 3P framework for optimizing management of older PLHIV who develop neurocognitive impairment during their life course. This framework consists of three main pillars of management namely – protect brain health and cognitive reserve, preserve physical function and promote social and emotional resilience to prevent complications of functional decline and complete dependence, where institutionalization may be required.17,77 In addition to protecting brain health and preserving cognition with interventions as alluded to previously, proactive management and optimization of all potential aetiological factors for cognitive impairment is crucial to prevent concomitant detrimental effect. Furthermore, early screening and addressing functional decline is key to preserve and optimise physical function. Lastly, the social determinants of health (as depicted in Figure 1) should not be neglected because it may affect social and emotional resilience, which is essential for cognitive health.
77
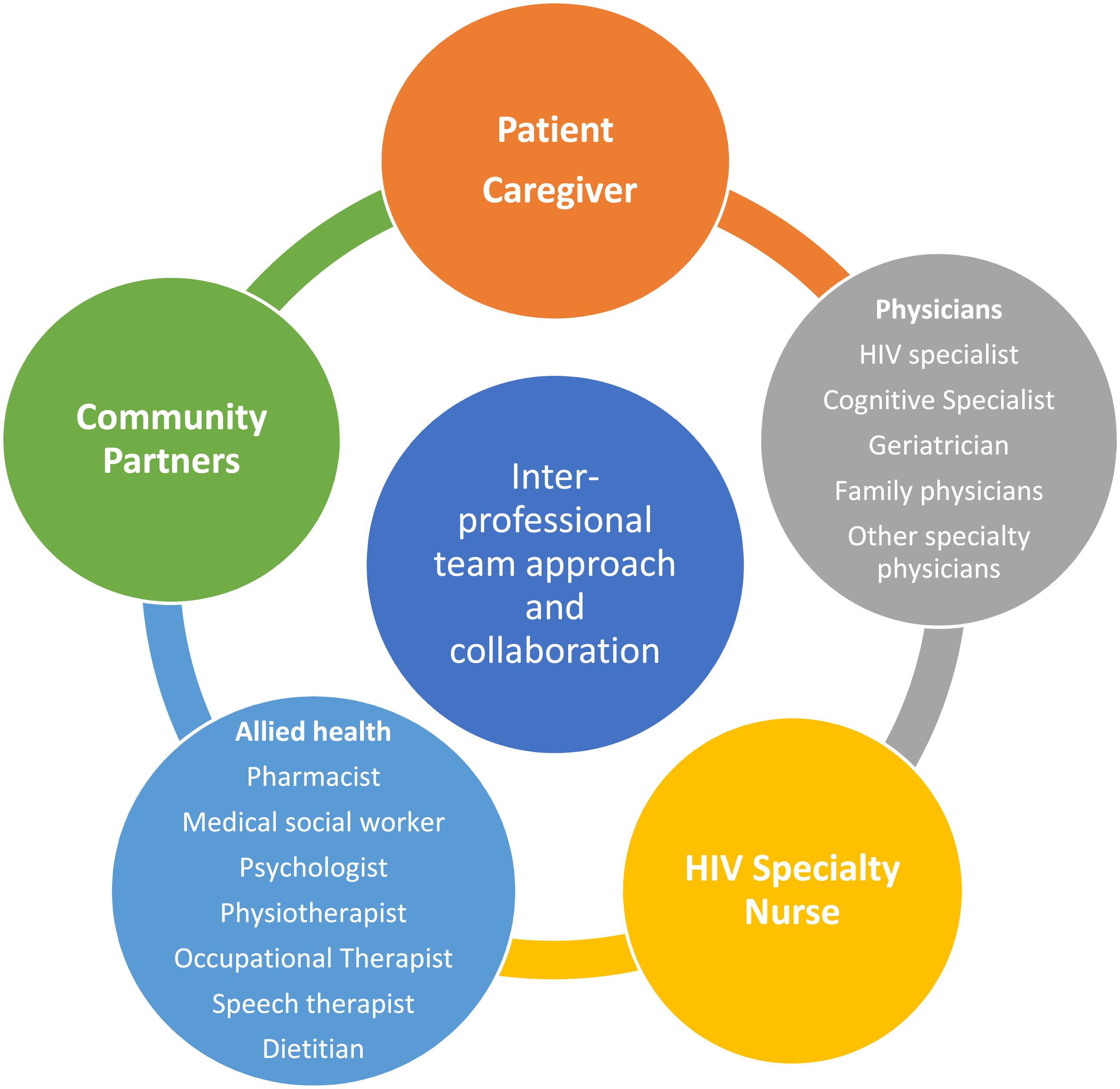
This management framework is best executed with an inter-disciplinary team approach consisting of medical and allied health professionals as well as community partners as illustrated in Figure 3. Integrated model of care for the older PLHIV with neurocognitive impairment involves inter-professional team approach and collaboration.
15
Conclusion
Unique challenges in managing the health of older PLHIV include greater incidence of health complications, comorbidities, and frailty. There is a need for greater awareness (and when necessary, training) on neurocognitive impairment, mental health and comorbidities that plagued older PLHIV among healthcare providers, allied health, community healthcare partners, caregivers, and policymakers. In addition, education, research, and collaboration among physicians from different specialities (such as Infectious Disease, Geriatric Medicine, Neurology, Psychiatry, and Family Medicine), HIV specialty nurses, allied health professionals and community partners would enhance diagnostic processes and treatment pathway, resulting in better management of neurocognitive impairment in older PLHIV. By incorporating collaboration between ID physicians and geriatricians to deliver comprehensive, integrated person-centred care, we aim to improve health outcomes and overall wellbeing beyond viral suppression, in a seamless, cost effective and efficient manner.
Footnotes
Author contributions
RN researched literature, conceived the study, and wrote the first draft of the manuscript. RN, KF, YE reviewed, edited the manuscript, and approved the final version of the manuscript.
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this articles.
Data availability
Data sharing is not applicable to this article as no datasets were generated or analysed during the current study.