
Abstract
Background
Prediction equations for resting metabolic rate (RMR) are valuable in managing patients’ weight; however, no accurate equation exists for Singaporeans.
Objective
To develop and cross-validate a predictive regression equation for RMR in Singaporeans, using indirect calorimetry as the reference method.
Methods
104 healthy Singaporeans (34.3 ± 12.2 years) participated, comprising 34 men and 70 women. Anthropometric measurements and demographics information were obtained from participants. RMR was measured via indirect calorimetry (TrueOne 2400 system). Stepwise regression analysis was used to develop the most parsimonious predictive equation. Performance of the equation was evaluated using ordinary least products (OLP) regression and Bland–Altman analysis, whilst internal cross-validation was performed by use of the predicted residual sum of squares (PRESS) method. To compare the new equation with existing ones, the performance of the Harris-Benedict equation was also evaluated.
Results
The best predictive equation takes the form RMR(kcal) = 918 + 16.5(weight)-135.7(gender) - 1152(Waist-to-height-ratio) +0.014(International Physical Activity Questionnaire Score), where gender = 1 (female) or 0 (male). OLP regression revealed no systematic bias for the new equation. Bland–Altman analysis showed that its total (systematic and random) error was 212 kcal. Internal model validation using the PRESS method revealed minimal reduction in predictive accuracy. In contrast, OLP regression showed a significant pattern of over-prediction by the Harris-Benedict equation (y-intercept = −280 kcal; 95%CI, −100 to −461 kcal).
Conclusions
Our new equation outperformed the Harris-Benedict equation in accurately predicting RMR in Singaporeans. Comprising easily obtained anthropometric and self-reported measures, we envisage its potential relevance in clinical and epidemiological settings.
Background
Knowledge of a patient’s specific energy needs allows optimal management of his or her weight and nutrition. 1 In the teeth of an emerging epidemic of diabetes, obesity and other weight-related morbidities, 2 a weight management plan that is individualized for patients is a crucial tool in the hands of the clinician. 1 Indirect calorimetry (IC), doubly labeled water (DLW), predictive equations for resting metabolic rate (RMR) and Kilocalorie per Kilogram (KPK) are some of the methods in which a clinician can obtain information about a patient’s energy needs. 3 IC is an accurate method but is costly, requires strict conditions to be met, and technical expertise to administer. 1 While portable IC machines are a cheaper alternative, they have a larger margin of error. A predictive equation for RMR is the most convenient method of choice to determine one’s energy needs. 1 However, since the development of the Harris-Benedict formula in 1919, a trend of population-specificity in predictive equations has emerged. 4 Indeed, many established prediction equations have been shown to be inaccurate for patients of varied ethnicities. 5 These inaccuracies arise mainly due to differences in body composition and physiology between different ethnic groups. 6 Hence, there is a need for population-specific RMR prediction equations.
We have previously shown that available RMR prediction equations may not be appropriate for Singaporeans. 7 Our study found that for 234 Singaporean patients, only half of RMR measurements (MedGem portable indirect calorimeter) were within 10% agreement with the Harris-Benedict and Mifflin equations. 7 As a multi-ethnic Asian community, clinicians in Singapore are in need of an RMR prediction equation that factors in the unique characteristics of the local population. A recent publication developed a Singapore basal metabolic rate equation in Chinese which is solely based on body weight and gender, 8 but took no account of the physical activity levels of the individual.
Objectives
This study aimed to develop and cross-validate a predictive regression equation for RMR in healthy Singaporeans, using indirect calorimetry as a reference method. To compare the new equation with existing ones, the performance of the Harris-Benedict equation was also evaluated.
Methods
Subjects
The study was carried out at a large tertiary hospital in Singapore. A total of 104 healthy Singaporean adults aged 34.3 ± 12.2 years were included in the study. 70 female and 34 male subjects were recruited. There were 93 Chinese, two Malays, three Indians and six of other ethnicities excluding Caucasians.
The exclusion criteria for this study were diseases that might affect metabolic rate and respiratory diseases which might have influenced the IC measurements that were based on gas analysis of each breath. Participation in the study was dependent upon having a stable weight to minimize any misleading effects on body composition and anthropometric measures.
Study design
The study was explained to subjects before informed consent was taken for participation or the questionnaire filled in. Subjects arrived between 0800 h and 1000 h to have their measurements taken. All assessments were done on subjects who in the previous 10 h (i) fasted from food, caffeine and alcohol, and (ii) refrained from smoking and vigorous physical activity. 9 Height, weight, waist, hip and neck circumferences were measured, followed by RMR using a TrueOne 2400 metabolic cart (Parvo Medics, Sandy, UT).
Anthropometric measures
Height (cm) and weight (kg) were measured in bare feet and after voiding. Height was measured using a wall chart, and weight and body mass index (BMI) were measured using a Tanita body composition analyzer (TBF-300A). Waist, hip and neck circumferences were taken using a tape measure. Waist circumference was measured with the tape measure horizontal at the midpoint between the 12th rib and the anterior superior iliac spine, on complete exhalation with abdominal musculature as relaxed as possible and subject’s arms by their side. 10 Hip circumference was measured over the maximal circumference of the gluteal region, with the subject’s feet together and the tape measure horizontal. Waist to hip ratio (WHR) 11 and waist to stature ratio (WSR) 12 were calculated. Neck circumference was measured just under the larynx, with the tape measure perpendicular to the long axis of the neck. 13
Resting metabolic rate
Resting metabolic rate was measured using indirect calorimetry. TrueOne 2004 metabolic cart analyzed the gas in the breath of each subject as they breathed into a ventilated hood. The TrueOne system was chosen because it is valid for RMR and respiratory exchange ratio when compared to Deltatrac Metabolic Monitor, a gold standard in IC, and it also displays low within subject coefficient of variation. 14 The metabolic cart was calibrated daily according to the manufacturer’s instructions. Subjects lay still for 30 min in a supine position. Participants were instructed to breathe normally, and those who fell asleep or moved were excluded from data analysis. From the last 20 min of data, a 5 min windows with less than 10% coefficient of variation (CV) for oxygen consume (VO2) and carbon dioxide produced (VCO2) was selected to calculate an average RMR value for that subject. 9 Subjects whose VO2 and VCO2 showed greater than 10% CV were excluded from data analysis.
Questionnaire
Each subject filled out a questionnaire that collected information about their socioeconomic background, medical history and dietary habits. The IPAQ short-form, a questionnaire to assess physical activity with good test-retest reliability, 15 was incorporated into our questionnaire. Questions about intensity, duration and frequency of physical activity were asked so that weekly metabolic equivalents (METs), IPAQ scores and IPAQ categories (low, moderate, high) for level of physical activity could be elucidated. The prescribed protocol calculating IPAQ scores for the IPAQ short-form questionnaire was followed closely.
Methods comparison
Descriptive results are expressed in terms of group means ± standard deviations (SD) whilst IPAQ scores are presented as medians and interquartile ranges. 4 The criterion measure for the method comparison was resting metabolic rate derived from IC (RMRIC). Method-comparison analysis was performed in two stages. First, we used ordinary least product (OLP) linear regression equation between RMRIC values and RMR predicted by the Harris-Benedict equation (RMRHB) to determine the presence of fixed bias. 16 Specifically, if the 95% confidence interval (95% CI) limits for the y-intercept excluded 0, fixed bias is present. Next, total error – the aggregate of both systematic and random errors – for the Harris-Benedict method against the criterion method was determined by use of the Bland and Altman (B-A) plot. 17
RMR prediction model
Multivariable stepwise regression analysis was performed to identify a new predictive equation for RMR in Asian Singaporeans. RMRIC was the dependent variable. Independent variables were (i) demographics variables (sex, age, and ethnicity which was dummy coded as “1” for Chinese and “0” for non-Chinese), (ii) anthropometric variables (height, weight, BMI, waist circumference, hip circumference, WHR, neck circumference, WSR), and (iii) physical activity level as indexed by the IPAQ. In the final regression model, the coefficient of determination (R2) was estimated whilst possible multi-colinearity amongst the retained predictors was assessed by use of the variance inflation factors (VIF). A VIF less than or equal to four was taken as an acceptable cut-off.
18
Internal model validation was performed by using the Predicted Residuals Sum of Squares (PRESS) statistics.
19
When calculating the PRESS, one observation from the original dataset was removed and the regression model based on the resultant dataset – comprising n-1 observations – was used to compute a predicted value for the excluded observation. This procedure was repeated for each observation, and the PRESS statistics is defined as the sum of the squared differences between the predicted value and the observed value.19,20 To assess model adequacy, the PRESS statistics was used to determine the multiple co-efficient of determination (R2) and the standard error of the estimate (SEE) based on the following formulae:


Another method of validation involving assessment of pure error (PE) was utilized:

Finally, total error for the RMRNEW was assessed using the B-A plot as outlined earlier. 95% levels of agreement (LOA) were calculated to assess the agreement between the criterion and predicted RMR. All statistical analyses were performed using Statistical Package for Social Sciences 17.0 (SPSS, Chicago, IL), with statistical significance set at p < 0.05.
Ethical statement
Ethics approval was received from the Singhealth Centralised Institutional Review Board. All patients gave written informed consent before participating.
Results
Primary analysis
Subject characteristics including metabolic data.

aPercentages are of the total number of subjects for that column.
bIPAQ scores are reported as median with interquartile ranges.
BMI: Body mass index; WHR: waist circumference to hip circumference ratio; WSR: waist circumference to stature ratio; IPAQ: International Physical Activity Questionnaire; MET: metabolic equivalent; RMRHB: Resting metabolic rate predicted by Harris-Benedict equation; RMRIC: resting metabolism rate predicted by indirect calorimetry; VO2: oxygen consumed during indirect calorimetry; VCO2: cardon dioxide produced during indirect calorimetry; RQ: respiratory quotient.
RMRHB versus RMRIC
The mean RMR was 1454 (SD 235) kcal based on the Harris-Benedict equation and 1323 (SD 259) kcal based on IC. Accordingly, the 95% CI for the mean difference between methods (fixed bias) of 131 kcal was 108–155 kcal. Only 50.5% of RMRHB values were within 10% agreement of RMRIC values. Using OLP regression, the presence of fixed bias for the RMRHB was further confirmed (intercept = −280 kcal; 95%CI, −461 to −100 kcal). The total error (i.e., mean bias and random error) for the Harris-Benedict method is shown in the B-A plot (Figure 1).
17
Specifically, the total error ranged from an overestimation of 375 kcal to an underestimation of 113 kcal. Bland–Altman plot representing comparisons between Harris-Benedict (HB)- and Indirect Calorimetry (IC)-derived resting metabolic rate (RMR) values. Fixed bias and random error lines (95% limits of agreement) are included.
RMR prediction model

Regression model and internal cross-validation for the prediction of resting metabolic rate (RMR).
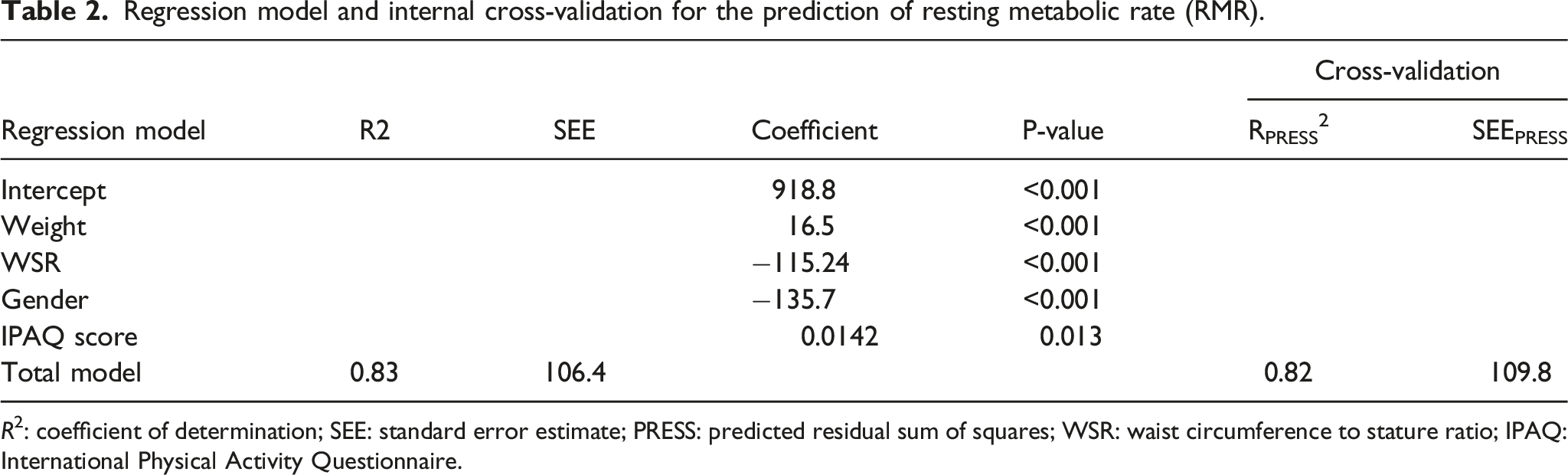
R2: coefficient of determination; SEE: standard error estimate; PRESS: predicted residual sum of squares; WSR: waist circumference to stature ratio; IPAQ: International Physical Activity Questionnaire.
Based on the standardized beta-weights of the final regression model, body weight (β = 0.92) wielded the strongest influence on RMRIC, followed in order by WSR (β = −0.27), gender (β = −0.25), and IPAQ score (β = 0.11). The VIFs amongst the predictors were less than 4, indicating relatively low collinearity. Internal model validation of the prediction model using the PRESS statistics (16) revealed minimal shrinkage in predictive accuracy (R2 = 0.83 vs 0.82 and SEEp = 106.4 vs 109.8 kcal) (Table 2). The pure error for the new prediction model is 103.8 kcal.
RMRNEW equations versus RMRIC
Using OLP regression, RMRNEW showed no fixed bias (intercept = −122 kcal; 95%CI, −246 to 1.6 kcal) or proportional bias (slope = 1.09, 95%CI, 0.99–1.19). Figure 2 shows the B-A plot for the new equation method and its total error was a symmetrical over and underestimation of 212 kcal. 80% of RMRNEW values are within 10% agreement of RMRIC values. Bland–Altman plot representing comparisons between new equation- and indirect calorimetry (IC)-derived resting metabolic rate (RMR) values. Fixed bias and random error lines (95% limits of agreement) are included.
Discussion
The new regression model we have formulated appears to be well suited for use in healthy adults, primarily Chinese Singaporean women, as it offers several advantages over the Harris-Benedict equation. Specifically, it comprises easy-to-calculate variables that have a strong physiological link to RMR, has a sound statistical basis, and is free of the substantial fixed error inherent in the classical Harris-Benedict equation.
Variables in the equation: physiological links to RMR
Because the relationship between RMR and the variables of gender and weight is well established in the published literature, we focus our discussion on the more novel predictors of RMR – namely, the WSR and IPAQ scores. Furthermore, there are growing evidence that waist circumference is a better predictor of chronic diseases in Asians .22,23 The WSR is a surrogate measure of visceral adipose tissue that accounts for stature. 24 To the extent that the WSR may act as an index for body composition, 25 it seems reasonable to argue that in two individuals sharing the same weight but different WSR, the individual with the higher WSR has greater adipose tissues and hence, a lower RMR. For this reason, unlike previous predictive equations, including WSR (along with body mass) in the new equation provides greater accuracy as the equation considers body composition – an important determinant of RMR.
The IPAQ score reflects the individual’s level of physical activity. A chronic level of physical activity elevates RMR and prevents loss of fat free mass (FFM). 26 A larger proportion of FFM increases RMR. 26 As physical activity has such a strong bearing on RMR, the new equation has the advantage over other equations of incorporating the IPAQ score. As with WSR, the IPAQ score is a value that is easily obtained for use in predicting the patient’s RMR.
The new equation was unbiased and precise in predicting RMR for Asian Singaporeans with regards to the psychometric properties. Specifically, a high adjusted-R2 and low SEE value were obtained, and the slopes and intercept for the OLP regression did not significantly differ from the line of identity. There were no significant mean differences between observed and predicted RMR, and a relatively narrow LOA were found. Internal model validation by PRESS statistics yielded a high RPRESS2 and low SEEPRESS. Data splitting was avoided through use of the PRESS method, which allows the whole sample to be used for validation. PRESS statistics usually generate less promising estimates of an equation’s capability, 19 which highlights the reliability of the newly developed equation.
On the other hand, the Harris-Benedict equation over-predicted RMR in Asian Singaporeans adults and is therefore may not be suitable for use in our local clinical dietetics practice. Presumably, an over-prediction of RMR resulted because for the same gender, weight, height and age, Caucasians in the study of Harris and Benedict had higher lean body mass and lower body fat percentage than did Asian Singaporean adults in this study. 27 This over-prediction of RMR in Asians by equations derived from Caucasian data is consistent with other studies in the field.28–31
Predictors not included in the new equation
It is noteworthy that common RMR predictors such as age and FFM were not included in the new equation. While there is an age-related decline in RMR independent of changes in FFM, 32 age may not have been a significant predictor of RMR in this study possibly because of the small number of older subjects (17% of subjects were older than 50 years of age). In some prediction equations FFM is the strongest predictor, 4 while in others it is not. 33 In clinical practice, it may be difficult to gain an accurate measure of FFM; in particular FFM from bioimpedance analysis may not be precise. 34 Hence FFM was not included in regression analysis of the final prediction model. However, the new equation does not fall short in this area as body composition is taken into account in the form of WSR.
Study Limitations and further research
The majority of the subjects were female, Chinese and aged between 21 to 40 years old. The effects of race and advanced age may only have been marginally taken into account, especially since the final equation does not include either as independent variables. For the same BMI, Singaporean Chinese have lower body fat percentage than Singaporean Indians. 35 The BMI cutoff for obesity in Singaporean Indians is 26 kg/m2 rather than the 27 kg/m2 recommended for Chinese Singaporeans. 35 Some caution may be needed in applying this equation to Indians, due to the differences in body composition between ethnicities.
Another limitation of the study is that it did not restrict measurements of RMR based on the female subjects’ menstrual cycle. The menstrual cycle increases energy expenditure by up to 6.1% (standard deviation 2.7%) during sleep, 36 and this may have led to changes from the normal level of energy expenditure in female subjects. The measurements of neck, waist and hip circumferences may also be subjected to measurement errors due to clinicians’ clinical experiences despite specific body landmarks are used.
Finally, the equation is limited in its applicability to the critically ill, the obese and the elderly. Critical illness can cause the patient’s metabolism to deviate from normal, 37 and the predictive equation would no longer be accurate for them. Up to 15% daily variability in critically ill patients can be expected, and indirect calorimetry is a more accurate method for establishing RMR. 4 In obese patients, energy expenditure varies greatly, and the best method to determine their caloric needs is still controversial. 4 The accuracy of predictive equations in obese adults compared to non-obese is lower, and the rate of individual errors is higher. 5 In the elderly, predictive equations tend to underestimate RMR. 38 This underestimation in the elderly, in combination with the small pool of older subjects and the lack of age as a predictor in this study’s equation, merits caution in the use of the equation in older Singaporeans.
Further research needs to be done on how well RMR is predicted for other ethnicities in Singapore, especially Malay and Indians. More studies could be done on predicting RMR in critically ill, obese or elderly Singaporeans. An investigation on how direct body composition measures can predict RMR in Asian Singaporeans would also be appropriate.
Conclusions
The Harris-Benedict equation was shown to over-predict RMR by 9.9% in Asian Singaporean adults, specifically by 7.0% in men and 11.8% in women. A new RMR predictive equation was developed for Singaporeans and was internally validated using PRESS statistics. The new equation displayed accuracy in its predictions as high RPRESS2 and low SEEPRESS were obtained and variables had strong physiological links to RMR. There was no bias between methods as the mean of paired differences between observed and predicted RMR was not significantly different from zero. This new equation provides a practical and convenient method for accurately predicting RMR in Singaporean patients, mainly Chinese females, in aid of their weight and nutrition management with the inclusion of novel predictors, namely waist circumference to stature ratio as well as physical activity.
Footnotes
Acknowledgements
We thank the staff at the Department of Physiotherapy and Department of Endocrinology, Singapore General Hospital for their assistance in conducting this study. In addition, we thank the research subjects for volunteering their time.
Author contributions
We acknowledge HCK’s contribution to study design and implementation, TNFMX’s work on data analysis and drafting of the manuscript, as well as NLWC and TKW’s input to revisions of the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.