
Abstract
Ossifying fibromyxoid tumour (OFMT) is a soft tissue neoplasm of uncertain differentiation, with potential for recurrences and metastases depending on the presence of atypical or malignant histological features. Most cases show an incomplete shell of mature bone in the periphery of the lesion. Recurrent PHF1 gene rearrangements were also recently reported in OFMTs, with the most common rearrangement involving a fusion to EP400. We report a case of a 75-year-old male that was diagnosed with an OFMT showing an unusually prominent central ossification. Further, this lesion also harboured the less commonly reported EPC1-PHF1 gene fusion, thus further characterising the morphological features that are associated with this molecular event in this entity. Differential diagnoses of lesions with prominent ossification and emerging molecular findings associated with this entity are discussed.
Introduction
Ossifying fibromyxoid tumour (OFMT) is a soft tissue neoplasm of uncertain differentiation, 1 with potential for recurrences and metastases depending on the presence of atypical or malignant histological features. 2 It was first described in 1989, in a case series of 59 cases 3 that were characterised by small, round cells arranged in nests, cords and/or sheets, within a fibromyxoid stroma. Enzinger et al. 3 also reported that 81% of these cases showed an incomplete shell of mature bone in the periphery of the lesion although bone may also be found in the fibrous septa or centrally.1,2,4 Folpe et al. 2 reported that bone was distributed randomly in 5 out of 44 (11%) OFMTs that showed ossification, while another series of 26 subcutaneous OFMTs 5 reported that woven bone was randomly distributed in a more central location of the lesion in only one case (3.8%). Of note, in the series by Folpe et al., 2 1 out of 5 OFMTs that showed a random or central distribution of bone recurred and metastasized although the relative risk compared to the more commonly reported pattern of peripheral ossification was not statistically significant.
Recently, recurrent PHF1 gene rearrangements were reported in OFMTs,6,7 with the most common rearrangement involving a fusion to EP400 in 44% of cases, and other less common rearrangements involving MEAF6-PHF1. 8 EPC1-PHF1 gene fusions were rarely reported previously.8–10 Herein, we report a case of a 75-year-old male that was diagnosed with an OFMT showing an unusually prominent central ossification, which raised differential diagnoses that had features of ossification. This lesion also harboured the less commonly reported EPC1-PHF1 gene fusion, thus further characterising the morphological features that are associated with this molecular event in this entity.
Case report
A 75-year-old male, without significant medical history, presented with a 10-years history of a right thumb lump that had increased in size progressively. It had also become painful recently and begun to affect his fine motor function. There was no history of prior trauma. On examination, this lump was located on the right thumb pulp, measured 3 cm by 1.5 cm, and was noted to be irregular and hard. The clinical impression was that of a pigmented villonodular synovitis.
A magnetic resonance imaging (MRI) was performed and showed a well-defined lobulated subcutaneous mass at the volar aspect of the thumb distal phalanx (Figure 1(a), measuring 1.6 cm by 1.5 cm by 0.9 cm. The mass showed areas of hypointense T1-weighted and T2-weighted signal with magnetic susceptibility artefact on gradient echo images indicating presence of paramagnetic substances such as calcification. Contrast enhancement was seen in the periphery of the lesion and in the non-calcified areas (Figure 1(b)). The deep aspect of the lesion was noted to abut the flexor pollicis longus tendon, but the tendon was reported to be intact with no tendon sheath effusion. The lesion also mildly displaced both the radiovolar and ulnovolar neurovascular bundles. Intra-operatively, this lesion was noted to be well-circumscribed and fleshy, located in the subcutaneous plane, corresponding to the radiological findings. The lesion did not arise from the neurovascular bundles. (a) T1 turbo-spin-echo (TSE) MRI showed a well-defined lobulated subcutaneous mass with hypointense areas suggestive of calcification at the volar aspect of the thumb distal phalanx, measuring 1.6 cm by 1.5 cm by 0.9 cm; (b) T1 TSE post contrast fat saturated images demonstrated contrast enhancement at the periphery of the lesion and in the non-calcified areas.
On gross pathological examination, it was a nodular tissue measuring 1.8 cm in greatest dimension Cut sections show extensively calcified areas, occupying approximately 80% of the lesion (Figure 2). Microscopic examination showed a circumscribed and encapsulated lesion with bone interspersed with lesional cells (Figure 3(a)). The lesional cells were arranged in sheets, cords and trabeculae, within a fibromyxoid stroma (Figure 3(b)). These cells showed bland ovoid and elongated nuclei that contain fine dispersed chromatin and small distinct nucleoli (Figure 3(c)). Centrally, extensive areas of mature bone with irregular cement lines and adipocytic marrow were present (Figure 3(d)), mimicking a bone-containing lesion. Osteoid formation and cystic degeneration with spaces filled with mucoid matrix were also noted. Small nodules of neoplastic tissue were within the fibrous capsule. No high-grade cytological atypia, increased cellularity, necrosis, increased mitotic activity, or multinucleated giant cells were identified. Areas of ossification, occupying approximately 80% of the lesion, with only very focal (arrow) lesional cells seen. Microscopic examination showed (a) a circumscribed and encapsulated lesion with bone interspersed with lesional cells; (b) the lesional cells were arranged in sheets, within a fibromyxoid stroma; (c) These cells showed relatively bland ovoid and elongated nuclei that contain fine dispersed chromatin and small distinct nucleoli. (d) Centrally, extensive areas of mature bone with adipocytic marrow were present.

On immunohistochemistry, there was strong nuclear and cytoplasmic positivity for S100 (Figure 4(a)). Smooth muscle actin (Figure 4(b)) and CD10 (Figure 4(c)) were also positive. Negative immunohistochemical stains include SOX10, desmin, SAT-B2, GFAP, CD34, CD57, MNF116, CAM 5.2, EMA, and PR. INI-1 was retained. This case was sent for the Archer FusionPlex Pan-Solid Tumour Next-Generation Sequencing (NGS) Assay at the Department of Pathology and Laboratory Medicine at KK Women’s and Children’s Hospital, Singapore. This test has been validated for clinical use, and the test accuracy and precision were established and verified according to consensus guidelines described by the Association for Molecular Pathology and College of American Pathologists.
11
Subsequently, a gene fusion between EPC1 on exon 7 and PHF1 on exon 2 was detected, with 145 fusion transcript reads detected (more than 5 reads constitutes strong evidence) and 52 unique start sites (more than 3 constitutes strong evidence). (Figure 5) This case was eventually reported as OFMT with prominent ossification. (a) strong nuclear and cytoplasmic positivity for S100; (b) positivity for smooth muscle actin; (c) positivity for CD10. Archer FusionPlex Pan-Solid Tumour Next-Generation Sequencing (NGS) Assay results, showing a gene fusion between EPC1 on exon 7 and PHF1 on exon 2, with 145 fusion transcript reads detected and 52 unique start sites.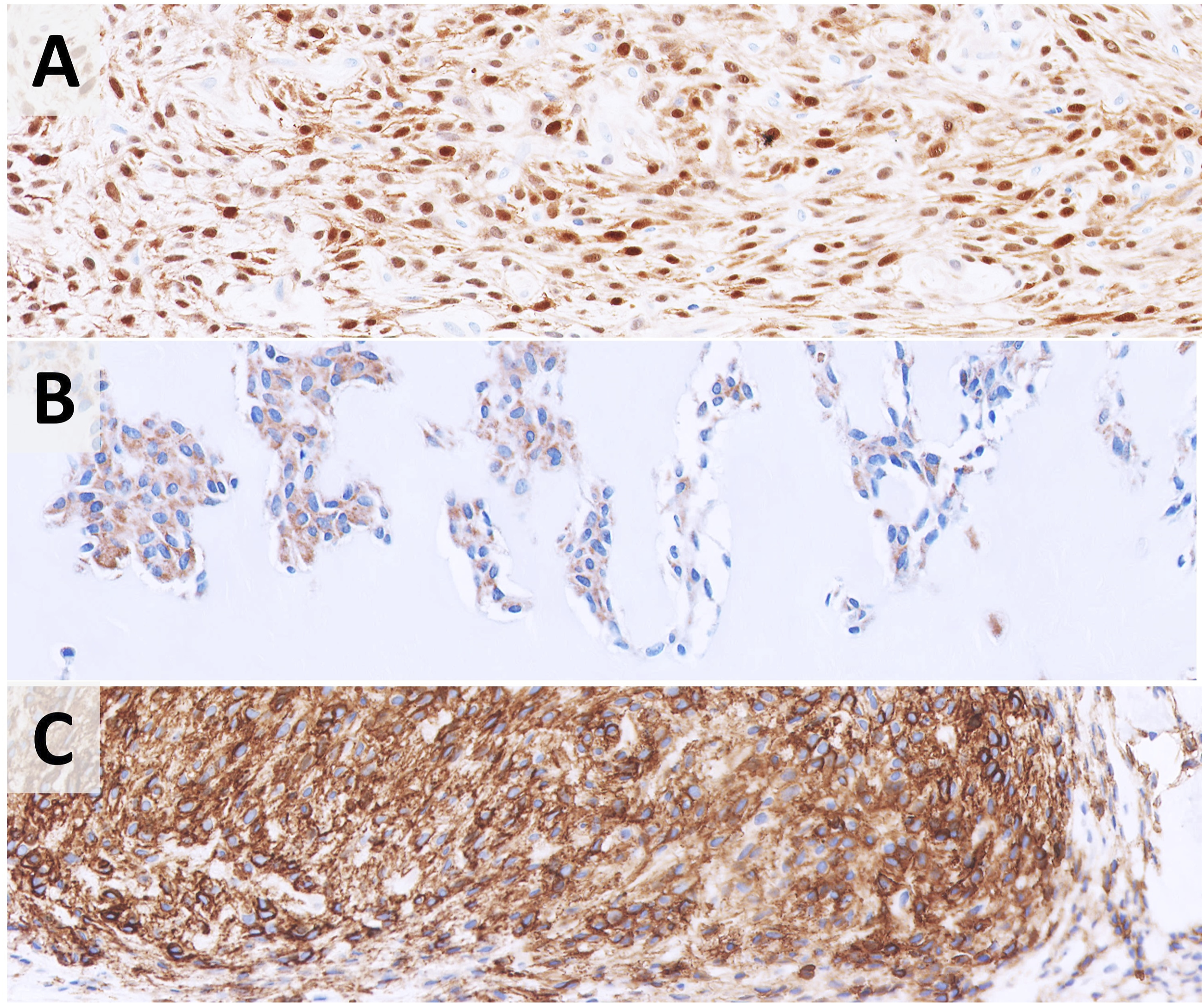

Post-operatively, the patient regained full active range of motion of hand without any post-operative complications. He was given an open appointment for follow up.
Discussion
In this case report, we report a 75-year-old male with an OFMT that showed an unusually prominent central ossification, with EPC1-PHF1 gene fusion identified on NGS. Although ossification in random locations and fibrous septa of OFMT has been well-reported, to the best of our knowledge, this case likely represents the first case of an OFMT with a prominent central ossification, which raises important differential diagnoses, particularly bone-forming lesions. Furthermore, only a few cases of OFMT with EPC1-PHF1 fusion has been reported in the literature 8–10 and this case further characterises the clinical and histopathological findings of OFMTs associated with this gene fusion.
In this case, there were areas that showed the typical morphological appearance seen in an OFMT, with bland cells arranged predominantly in cords, trabeculae, and sheets, within a fibromyxoid stroma. The key differential diagnoses for such an appearance include myoepithelial tumours, nerve sheath tumours and their epithelioid counterparts, and low-grade fibromyxoid sarcoma. Morphological and immunohistochemical differences between OFMT and relevant differential diagnoses have been summarised previously.4,12 Bone in the form of osseous metaplasia can be present in 10–15% of myoepithelial tumours and they tend to be present within the tumour as opposed to the peripheral location seen in OFMT. 4 The prominent ossification also raised the suspicion of an extraskeletal osteosarcoma, as well as other benign bone-containing lesions such as osteoma and osteophyte, which were excluded radiologically with the absence of connection to the underlying bone in this case. Our case showed immunohistochemical positivity for S100, CD10 and desmin. Although characterised by S100 positivity, 3 there is more recent evidence that OFMTs harbouring different gene fusions may show different immunohistochemical profile, which will be discussed subsequently. More importantly, it was negative for SOX10, cytokeratins and EMA, which ruled out myoepithelial tumours and nerve sheath tumours. Negativity for MUC4 and SATB2 also ruled out low-grade fibromyxoid sarcoma and extraskeletal osteosarcoma respectively. The other differential diagnosis was a soft tissue chondroma with extensive ossification, but no cartilage was identified in this case.
The majority of OFMTs shows recurrent gene fusions while the remaining 15% lacks a recurrent gene fusion. 8 PHF1 gene rearrangements occur in 49%–80% of OFMTs,7,8 with EP400-PHF1 fusion being the most common fusion, accounting for 44% of cases. 8 EPC1-PHF1 fusion was first reported to be implicated in malignancy in a case of an endometrial stromal sarcoma. 13 It has been postulated that with the EPC1-PHF1 fusion observed in OFMT, these genes implicated in acetylation and methylation may play a role in the pathogenesis of OFMT. 8 In a series of 39 OFMTs by Antonescu et al., 8 two cases of OFMTs showed EPC1-PHF1 fusion, with the first case being a 69-year-old male with a benign OFMT without ossification and the second case being a 49-year-old female with a malignant OFMT with ossification. S100 immunostaining was negative in these two cases. 8 In a more recent case series by Sbaraglia et al., 10 EPC1-PHF1 fusion was reported in a 29-year-old male with a tumour that showed a morphology compatible with sclerosing epithelioid fibrosarcoma and was negative for S100 but positive for MUC4 immunostaining; the diagnosis of a malignant OFMT was made after the gene fusion was reported. The patient subsequently had a local recurrence at 9 months from first onset but was reported to be disease free at last follow-up. 10 In another case series of 37 typical, atypical, and malignant OFMTs, 9 EPC1-PHF1 fusion was reported in one case although further information was not reported. Although malignant cases of OFMT harbouring EPC1-PHF1 fusion have been reported, it remains undetermined whether this fusion is actually associated with a malignant behaviour, considering that cases that had thus far showed a benign prognosis, including the current case, have been reported.
There is also emerging evidence of novel gene fusions in OFMT, with some reported to occur more frequently in malignant OFMTs. In particular, PHF1-TFE3 fusion has been reported in malignant OFMT.14–16 In the series of five OFMTs harbouring the PHF1-TFE3 fusion by Suurmeijer et al., 14 all cases did not show peripheral ossification and three cases met the histological criteria for malignancy. S100 immunoreactivity also tend to be negative in OFMT harbouring PHF1-TFE3 fusion.14,15 The malignant OFMTs harbouring PHF1-TFE3 fusion subsequently developed metastases.14,16 Other novel gene fusions that have been reported also include MEAF-SUZ12 17 and ZC3H7B-BCOR 15 fusions.
Conclusions
In conclusion, we report a novel case of an OFMT with an unusually prominent central ossification harbouring an EPC1-PHF1 fusion. Although peripheral ossification is expected in OFMT, prominent central ossification can be rarely encountered in OFMT. While most OFMTs harbour the EP400-PHF1 fusion, EPC1-PHF1 fusion has also been reported in both benign and malignant OFMT. Further clinical and pathological characterisation of OFMT harbouring this gene fusion is warranted.
Footnotes
Acknowledgements
We would like to acknowledge Dr Lai Peng Chan from the Department of Diagnostic Radiology, Singapore General Hospital, Singapore for her assistance in the radiology input, and Mr Chik Hong Kuick from the Department of Pathology and Laboratory Medicine, KK Women’s and Children’s Hospital, Singapore for his assistance in the obtainment of molecular results.
Author contributions
SHL and KS were the reporting pathologists of this case. THC, SHL and KS contributed to the conception of this study, writing of manuscript and approved the final version of manuscript for publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data
All data reported in this study is available in the manuscript.