
Abstract
Breast carcinoma is one of the most common carcinomas among women around the world. Most of the women with breast carcinoma will present with signs and symptoms of breast problems to the health facility. Upper limb swelling is one of the rare initial presentations although it is rather common in patients as a sequelae of breast carcinoma treatment. We herein would like to report a case where a post-menopausal female presented with left upper limb swelling with initial history suggestive of traumatic injury of biceps muscle. Subsequent investigations of ultrasound, mammography, biopsy sample of the left breast found that the left upper limb swelling was due to a newly diagnosed invasive lobular carcinoma of the breast, staging of cT4cN2Mx which caused a rapidly progressing stage 2 lymphedema of the left upper limb. Lymphedema of the upper limb is a common complication of breast carcinoma treatment, especially those who require axillary lymph nodes clearance. Breast carcinoma with initial presentation of lymphedema of the upper limb is rare. Due to the rare presentation, diagnosis of breast carcinoma can be delayed. Clinicians should have high awareness to exclude breast cancer when a patient presents with unilateral upper limb swelling.
Introduction
Breast carcinoma is one of the most common carcinomas among women around the world. 1 With effective public education on self-breast examination, cases are presented in the early stage of disease. Most of the women will present with suspicious findings in screening mammograms or signs and symptoms of breast problems to the health facility for assessment. Other non-breast related presentations can also be the sole complaint of the patients. Upper limb swelling is one of the rare presentations although it is rather common in patient as a sequelae of breast carcinoma treatment. Incidence of lymphedema is four times higher in patients with breast carcinoma that underwent axillary clearance. 2 Lymphedema that present preoperatively would result in the development of a much severe lymphedema following axillary lymph nodes clearance. 3 The upper limb lymphedema is expected to persist or worsen unless effective treatment is initiated. We herein would like to report a case where a patient first presented with lymphedema that led to the diagnosis of breast cancer.
Case report
A 54-year-old, postmenopausal female presented with a history of left upper limb swelling for a duration of six weeks. The swelling was preceded by strenuous activity after she lifted pails of water from outside the house due to water shortage. She went for a traditional massage for the swelling, however, instead of improving the swelling, which initially involved only the arm had progressed to involve the whole upper limb and affected her daily activities. The patient was then admitted to the orthopaedic ward with the working diagnosis of biceps muscle rupture.
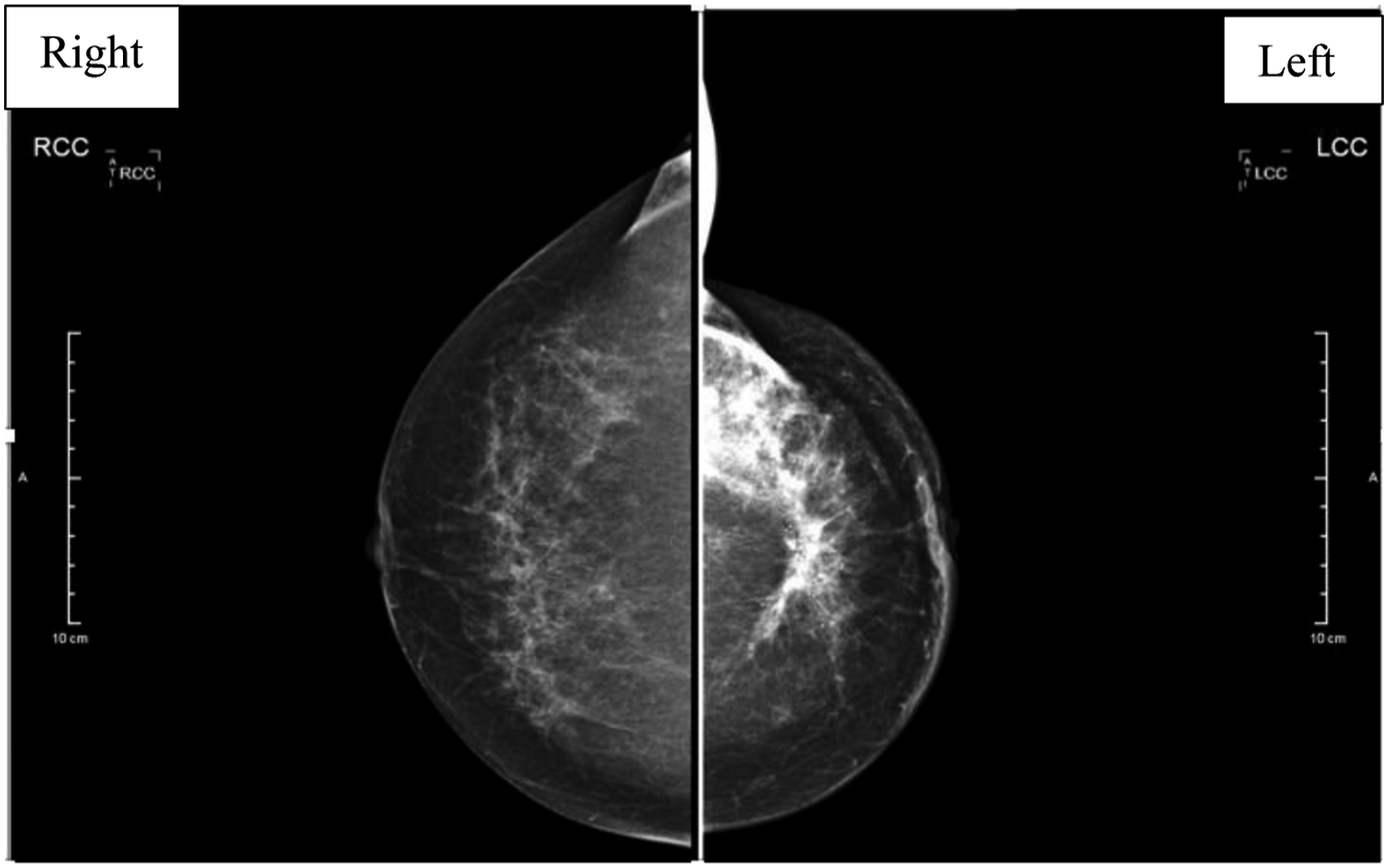
Physical examination showed the whole left upper limb lymphedema extending up to the lateral side of the chest wall and breast. The shoulder is held adducted with the elbow in a 70-degree flex position (Figure 1). She could not move the shoulder, elbow and her hand due to stiffness. Otherwise, no mass or lymph nodes were palpable. X-Ray of the left arm and forearm did not show any significant finding other than increased soft tissue shadow. Ultrasound of the left upper limb showed diffuse subcutaneous tissue oedema with loss of normal muscle striation and a small hypoechoic intramuscular collection. Overall, the ultrasound findings are suggestive of left upper limb cellulitis with a small intramuscular collection. Intravenous antibiotic was prescribed for a week but did not show improvement. Breast examination showed peau d’orange over the upper inner quadrant of the left breast with a mass measured 6x6 cm fixed to the underlying muscle. There was no retracted nipple, wound, or discharge. It was unable to check for axillary lymph nodes due to limited range of motion over the left shoulder. In view of her family history of breast carcinoma, mammography (Figure 2) and breast ultrasound (Figure 3) were ordered with the intention to rule out inflammatory breast cancer as a cause of her lymphedema. Both the imagings were highly suspicious. The subsequent biopsy confirmed a diagnosis of left breast invasive lobular carcinoma. Staging computed tomography (CT) of the thorax, abdomen and pelvis showed axillary lymphadenopathy but there was no distant metastasis, with staging of cT4cN2M0. Her left upper limb swelling corresponded to lymphedema late stage 2 (Table 1). Patient was referred to the occupational therapist for limb massage and application of compression garment. The lymphedema was not responded well with physical therapy and compression garment during the early phase of treatment. At the same time, the oncology team started her on neoadjuvant chemotherapy. Her left upper limb lymphedema significantly reduced after two months of physical treatment and chemotherapy. Upon completion of a total six cycles chemotherapy, the patient underwent left mastectomy with excision of pectoralis major muscle and axillary dissection. Unfortunately, the lymphedema of the left upper limb progressively worsened after the surgery and did not respond well to physical therapy. Patient’s left upper limb swelling. Mammogram showed left breast mass (diagram at the right) at retroareolar and left upper inner quadrant with involvement of underlying pectoralis muscle) and multiple cluster of mircrocalcifications. Highly suspicious of malignancy. BIRADS
5
Ultrasound of the left breast showed ill-defined irregular hypoechoic mass with posterior shadowing seen at the left breast retroarelar region, measuring approximately 3.2x5.0x7.2 cm. No intralesional vascularity. There is another hypoechoic mass seen at left upper inner quadrant of the breast, measuring approximately 2.7x5.9 cm. No intralesional vascularity. The mass has no fat plane with underlying left pectoralis muscle. A lymph node with thickened cortex (0.6 cm) is seen in visualized left axilla. International society of lymphology classification of lymphoedema.
4



Discussion
Lymphatic system is distributed throughout the whole body. Their function is to collect protein rich fluid from interstitial space and return it to the blood stream to maintain its homeostatic pressure gradient. Lymphatic fluid will pass through lymphocyte rich lymph nodes where it will be filtered. Regional lymphadenopathy can be due to infection or malignancy of the drainage zone. However, generalized lymphadenopathy is usually due to haematological malignancy. Lymphedema is an abnormal collection of protein-rich fluid in the interstitial tissue due to obstruction of lymphatic drainage. Protein rich fluid will retain more water and cause swelling of the interstitial tissue. Progressive fibroblast proliferation in the interstitial tissue will organize the retained fluid and cause irreversible swelling of the affected area. The severity increases as the lymphedema progresses. Classification of lymphedema showed in Table 1. 4
Lymphatic from the breast primarily drain into the axilla with small proportion to extra-axillary sites. Metastatic spread to the axilla occurs in up to 32.1% of patients with breast carcinoma. 5 Despite high incidence of axillary lymph nodes metastasis, breast carcinoma that presents with upper limb lymphedema is rare. The incidence of breast carcinoma presenting with upper limb swelling accounts for only 0.2% of the patients out of 2316 patients. 6 Atypical presentation (non-breast complaint) maybe responsible for the late diagnosis of patients with breast carcinoma due to different pathway of investigations undertaken to come to the final diagnosis. In this case, the patient was referred to the orthopaedic team for management of orthopaedic related causes when she sought treatment for her upper limb swelling. It is rare for breast carcinoma to first present with upper limb swelling.
Breast cancer treatments consist of surgery, radiotherapy, chemotherapy and hormonal therapy. Collectively, multimodal therapy has shown to improve patient survival. However, the treatments are associated with adverse effects. Lymphedema is strongly associated with breast cancer related therapy especially axillary lymph nodes clearance.3,4,7 Evidence has shown that axillary dissection, morbid obesity, and mastectomy are risk factors that increase the rate of lymphoedema. 2 Lymphedema that present preoperatively will much worsen following axillary lymph nodes clearance. 3 Hence, it is not hard to foresee our patient will suffer from more severe lymphedema after the mastectomy and axillary lymph nodes resection.
Upper limb lymphedema is associated with heaviness, reduced range of motion as well as distorted body image. Treatment of lymphoedema can be divided into conservative and surgery. The two stages combined physical therapy is the preferred conservative technique due to its effectiveness. 4 First stage consists of skin care, manual lymphatic drainage via massage, range of motion exercise and compression of the limb via multi-layered bandage. Second stage is to conserve and optimize the results obtained in stage 1, consists of elastic compression stocking and continue on the effort in stage 1. 4 Proper fit of compression stocking is essential and need to tailor as the size of lymphedema reduce with treatment. Patient’s understanding and compliance to the treatment and most importantly a dedicated team of therapists plays an important key to success. Surgical treatment of lymphedema includes liposuction, lymphaticovenous anastomosis and lymph node transfer operations in properly selected patients. 4 Surgical treatment can be offered to our patient in view of worsening left upper limb lymphoedema after her breast carcinoma treatment. However, the risk and benefit of the procedure had to be further explored.
Conclusion
Breast cancer is common in women. Clinicians should have a high index of suspicion in atypical presentation of breast carcinoma particularly upper limb edema to prevent delay in diagnosis and treatment.
Footnotes
Acknowledgements
We would like to thank the Director General of Health Malaysia for his permission to publish this article.
Authors’ contributions
YHN: data acquisition, patient management, conception, writing up and critical review. IS: patient management, conception, writing up. YCC: initial draft, literature search, writing up and critical review. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Availability of data and materials
Data sharing is not applicable to this article as no datasets were generated or analysed during the current study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This case report is registered under the National Medical Research Registry (NMRR) of Malaysia with registration number of NMRR-22–00,128-XGC.
Funding
The authors did not receive any specific grant from any funding agencies in the public, commercial, or not-for-profit sectors.
Informed consent
Written informed consent was obtained from the patient for her anonymised information to be published in this article.