
Abstract
Physicians play a pivotal role in the management of children and adults with Down Syndrome. Achieving full developmental potential in a child with Down Syndrome depends on prompt treatment of medical complications, family support and early establishment of intervention programmes. The presence of evidence-based guidelines support the physician both in the community and in restructured hospitals to provide timely and appropriate management recommendations. It will also aid in counselling parents and caregivers. Although most co-morbidity characteristics are common for the syndrome, the prevalence of different morbidities can be region specific, hence it is useful to have recommendations tailored to suit local population. Here we share the clinical guideline for children and adults with Down Syndrome in Singapore.
Background
Down syndrome (DS) is the most prevalent genetic condition worldwide with increasing survival into adulthood. 1 Survival has improved with many living into the sixth decade because of advances in intensive care and cardiac surgical facilities. 2 This trend is also observed locally.
Adults with DS have multiple medical concerns that originate earlier than the general population due to accelerated ageing that affects most organs systems. 3 In addition, disorders such as Alzheimer’s dementia, epilepsy, mood and behavioural disorders as well as autoimmune conditions are also more prevalent, affecting 40% of those in their fifties. However, coordinated care for these patients are sadly lacking with a recent survey done in Massachusetts revealing that specialty clinics for DS adults met the needs of only 3–5% of this population. 4
The aim of this guide is to provide community physicians, as well as parents and caregivers, information and medical recommendations for the management of children and adults with Down syndrome. Availability of a readily accessible reference in the primary care setting may be helpful for community physicians to provide uniform and consistent guidance to address each individual’s specific requirement not only in infancy and childhood but also in adulthood.
KK Women’s and Children’s Hospital Down Syndrome Programme
KK Women’s and Children’s Hospital (KKH) started a dedicated Down syndrome clinic in 1997 that offers specialized services for children with DS. There are currently 400 children in this programme. They receive comprehensive care by a multidisciplinary team, based on a standardised care pathway that starts from the antenatal period and continues through infancy until early adulthood.
Our robust multidisciplinary care includes, and is not limited to, services from Ophthalmology, Otorhinolaryngology (ENT), Cardiology, Neurology, Nephrology, Haematology, Paediatric Surgery, Adolescent Gynaecology, Dermatology, Anaesthesiology, Psychiatry, Orthopaedics, Sports Medicine and Allied health services.
Health Supervision for Down Syndrome Children.

DS: Down syndrome; IQ: Intelligent Quotient; EIPIC: Early Intervention Programme for Infants and Children; TFT: thyroid function test; FBC: full blood count; CAMWS: child and adolescent mental wellness service; LPA : Lasting Power of Attorney.
KK Women’s and Children’s Hospital Down Syndrome Adult Transition Checklist.

Based on our experience, 30% of DS patients in the outpatient clinic are lost to follow up as they grow older (unpublished hospital data). This group of patients may approach community physicians for support, as shifts in healthcare environment have resulted in primary care physicians taking on a greater role. Hence, it is important that community physicians are comfortable managing this cohort of patients, and this includes supporting their emotional and physical needs as well as providing basic medical surveillance.
Health Supervision for Down Syndrome Adults.
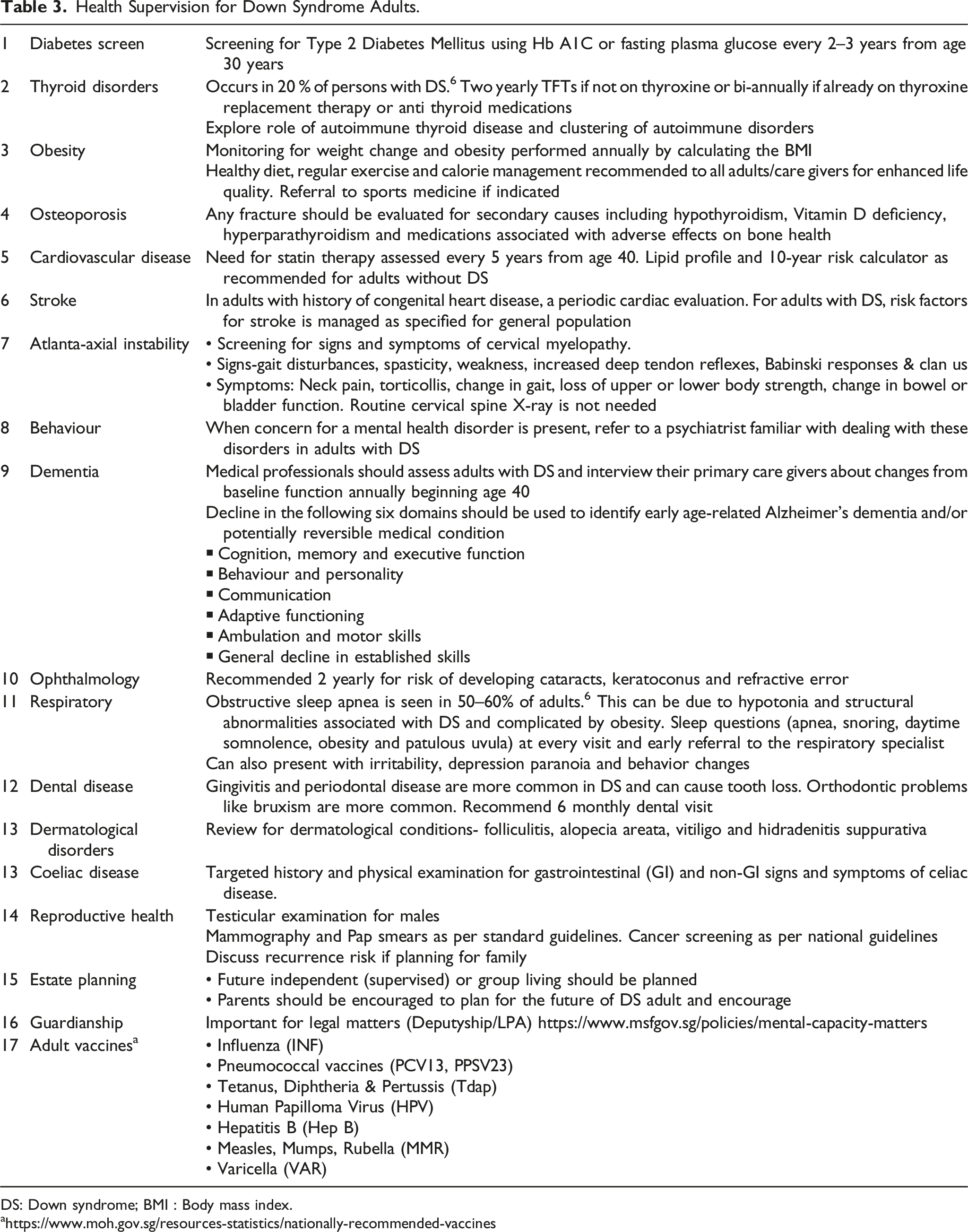
DS: Down syndrome; BMI : Body mass index.
In addition to literature review, the development of this guideline also involved expertise consensus from the multidisciplinary team of specialists who are involved in the medical care and follow up of these children in KKH. Consideration was given to established local prevalence of comorbidities in this group of patients based on our cohort of 176 patients (unpublished data).
Professional expert opinions from physicians in Sengkang General Hospital, who care for adults with disability, were sought and incorporated into this set of local guidelines. The aim is to ensure uniformity in care delivery for these DS adult patients in the outpatient setting, whether in tertiary institutions or in the community.
The KK Women’s and Children’s Hospital Down Syndrome Clinical Care Path
Standard care plan for mothers early in the pregnancy include routine screening for Hepatitis B, HIV status and Syphilis as well as an early dating scan. All mothers are offered Down syndrome screening at 11–13 weeks of pregnancy. The first trimester screening involves an ultrasound alone or in combination with a blood test. The ultrasound alone (to look for nuchal translucency) has a detection rate of about 80% and a combined test (including a blood test) has a detection of well above 90%. 8 The blood tests measures free beta human chorionic gonadotropin and placenta associated protein A. A more sensitive test, the Non Invasive Pregnancy Test is also offered at the first and second trimesters where fetal cells from maternal blood is extracted and analyzed for chromosomal defects. This has the highest detection rate of 99%. If screening tests reveal the baby has high risk for aneuploidy then a chorionic villus sampling or amniocentesis is offered for confirmatory diagnosis, after counselling by a genetic counsellor.
A second trimester screening ultrasound scan is scheduled at 20 weeks. If there is suspicion of structural anomalies, the fetal medicine specialist verifies the findings and the relevant medical or surgical specialists will be involved in the family conference with the support of the medical social worker (MSW). At this stage, information about DS and any co-morbidities, treatment options, recurrence risk, short and long term prognosis and community support services are discussed with parents in detail. Comprehensive birth plans must be in place should parents decide to continue the pregnancy. In the event they choose to terminate the pregnancy, they should get the necessary support.
Postnatal karyotyping is necessary when there is clinical suspicion of DS or when a definitive antenatal diagnosis was not established through amniocentesis. The baby is admitted to a level 2 care facility for monitoring and comprehensive assessment, including haematological and radiological tests, for possible associated co-morbidities, in addition to a thorough physical examination. 7
These include: 1. Full blood count and peripheral blood film to screen for leukemoid reactions, transient myeloproliferative disorder, thrombocytopenia and polycythemia, which are relatively common in infancy and is seen in 10% of this population.
7
2. These infants have a 1% risk of congenital hypothyroidism and deranged thyroid levels are common in infancy.
7
This is much higher than the reported incidence of 0.025–0.05%
9
among the general population. Further evaluation with a thyroid function test (TFT) is often needed till adulthood. 3. Cardiac assessment with two-dimensional echocardiogram. 50% of infants may have an abnormal echocardiogram and hence require a review with the cardiologist.
7
Commonly associated cardiac abnormalities identified within our cohort are Ventricular septal defect, Atrial septal defect, Atrioventricular septal defect, Patent ductus arteriosus and Tetralogy of Fallot. 4. Gastro-intestinal disorders include imperforate anus, duodenal and ileal stenosis/atresia and meconium peritonitis. These abnormalities if missed may be life threatening hence imaging is required. 5. Renal evaluation is also important. Associated conditions include horse-shoe, dysplastic kidney and vesicoureteric reflux. 6. Common endocrine disorders noted in or cohort include hypothyroidism (28%) and hyperthyroidism (2.5%). Frequent TFT will be required. 7. Major intestinal and renal abnormalities may be missed if the infant did not have an early fetal screening scan. 8. Universal newborn hearing screening assessment is done on all infants before discharge home to identify congenital hearing loss. 9. Feeding assessment by the speech therapist is important if clinically indicated as a proportion may have feeding difficulties due to hypotonia.
7
10. Physiotherapy services should commence during the birth admission to equip caregivers with the skills in handling and stimulating the infant with marked hypotonia.
The MSW continues to support the family postnatally by providing support to the family with emotional support as well, and to assist with resources for financial support, if required. The MSW usually helps to facilitate enrolment into the Early Intervention Programme for Infants and Children (EIPIC) centres during infancy and coordinate school placement at 5–6 years of age. They play an important role in introducing families to various community services like the Down Syndrome Association of Singapore, Family Service Centre and Social Service Centre.
Once a diagnosis of DS is made, a family conference is held while the infant is still in-patient, and the overall care plan until adulthood is explained and discussed with the family, to provide clarity regarding long-term follow-up. In this meeting, the need for continued follow up with the primary team, ophthalmologist, otolaryngologist, subspecialty teams as required and therapists is emphasized. Our cohort showed over 60% of eye and ENT disorders each (unpublished data). Hence, long term surveillance for refractory errors, movement disorders of the eye, cataracts, otitis media, hearing loss & chronic ear infections are highlighted.
The first specialist clinic visit is within 4–6 weeks of hospital discharge during which results of investigations done in the ward are explained and questions from parents are answered. Feeding and growth assessments are performed and routine vaccinations can be administered. Referral to the community EIPIC program 10 is made at this juncture as the waiting time may be up to a year for some centres. Some parents opt to enrol their child in private intervention centres, integrated child care programme or home based therapies (either from private therapists, or by the Down Syndrome Association). Either choice will be supported and the child’s progress monitored by the primary team of doctors. Once the child has secured a place for intervention, they are advised to continue therapies until school placement.
A psychological assessment is undertaken to evaluate the child’s cognitive functional level and understand the child’s weaknesses and strengths, in order to provide suitable recommendations for school placement. In addition, it is also to exclude underlying behavioural disorders, such as Autism. Special education placement requires an Intelligent Quotient (IQ) assessment to be done by a psychologist, by age 6, as school placements vary according to level of intellectual disability.
The child continues medical surveillance yearly at KKH until age 18. The process of transition to adult care is guided by the checklist given in Table 2.
Adults with DS have multiple medical issues that develop at an earlier age compared to their peers without DS. Table 3 gives an overview of the morbidities and the need for continuing surveillance by an adult physician.
Referral to the KKH Down syndrome clinic can be via a written referral from any polyclinic or private clinic in Singapore.
Footnotes
Acknowledgments
The authors would like to thank Dr Bhavani Sriram who established this clinic in 1997. She is fondly remembered by her patients and the department for her legacy in advocating holistic care for these children and adults. We also extend our gratitude to A/Prof Dr Angeline Lai, A/Prof Dr Teoh Oon Hoe, Ms Mavis Teo, Ms Mak Wei Lan, Prof Henry Tan and Prof Audrey Chia of KK Women’s and Children’s Hospital for their support and contributions to this clinical guideline. We also thank the physicians in KKH who helped us with collection of data needed for our local cohort data. Our gratitude also to all the physicians who have received our adult patients for continuing care and to the Down Syndrome Association for supporting the patients and caregivers.
Author Contributions
Dr Kavitha Sothirasan researched literature and conceived the study. Dr Kavitha Sothirasan and Dr Amudha Jayanthi wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Data Availability
Data sharing is not applicable to this article as no datasets were generated or analysed during the current study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Not applicable.