
Abstract
Base of penile abscesses are uncommon genitourinary tract infection. We present a case of a 31 years old man with poorly controlled diabetes mellitus, whom presented with scrotal pain and scrotal swelling for 1 week duration. Physical examination revealed a bulging mass at the base of penis. A high index of suspicion is needed to look for possible causes such as extension of abscess from perineum or anorectal, sexually transmitted disease, tuberculosis, history of penile instrumentation or injection and trauma. A large abscess at the base of penis was diagnosed by magnetic resonance imaging. He was successfully treated with transperineal incision and drainage, systemic antibiotic therapy, wound care and strict diabetic control. To the best of our knowledge, this is the first report of isolated base of penile abscess. The description of case, comprising the clinical presentation and management, is discussed in detailed with emphasis on the treatment approach.
Keywords
Introduction
Penile abscesses are uncommon genitourinary infection. 1 While many penile abscesses are spontaneous and do not have definite aetiology.2–5 A comprehensive literature review of 23 reported cases of penile abscess by Dugdale et al. 1 reckoned that over one-third of reported cases were spontaneous, and diabetic patients accounted for 25% of all reported cases. Some cases have been reported in association with intracavernousal injection therapy,6,7 foreign body, 8 priapism, 9 perirectal, 10 intra-abdominal abscess extension 11 and trauma. Standard treatment consists of incision and drainage in addition to systemic antibiotics. We present a case of spontaneous base of penile abscess in a patient with uncontrolled diabetes mellitus treated by transperineal incision and drainage, and systemic antibiotic therapy.
Case report
A 31-year-old man with poorly controlled Type II diabetes mellitus presented to Emergency department with worsening bilateral scrotal pain, swelling and fever for past 2 weeks. He had history of gluteal abscess underwent incision and drainage 3 years ago, subsequently recovered uneventfully. He had poorly controlled diabetes mellitus in which he defaulted oral hypoglycaemic medications and follow-ups for past 2 years. He had no history of prior genitourinary surgery, instrumentation, trauma, urinary tract infection, penile discharge or erectile dysfunction. He was treated with one course of oral antibiotics but did not show signs of improvement. On physical examination there was a 5 x 4 cm tender, fluctuating mass at the base of penis, at middle and posterior to scrotum (Figure 1(a) and (b)). Scrotal wall was indurated, no discharges, bilateral testes and penis normal. Digital rectal examination revealed no significant finding. (a) and (b) showed a bulging mass over base of penis (black arrows) with the scrotum lifted superiorly.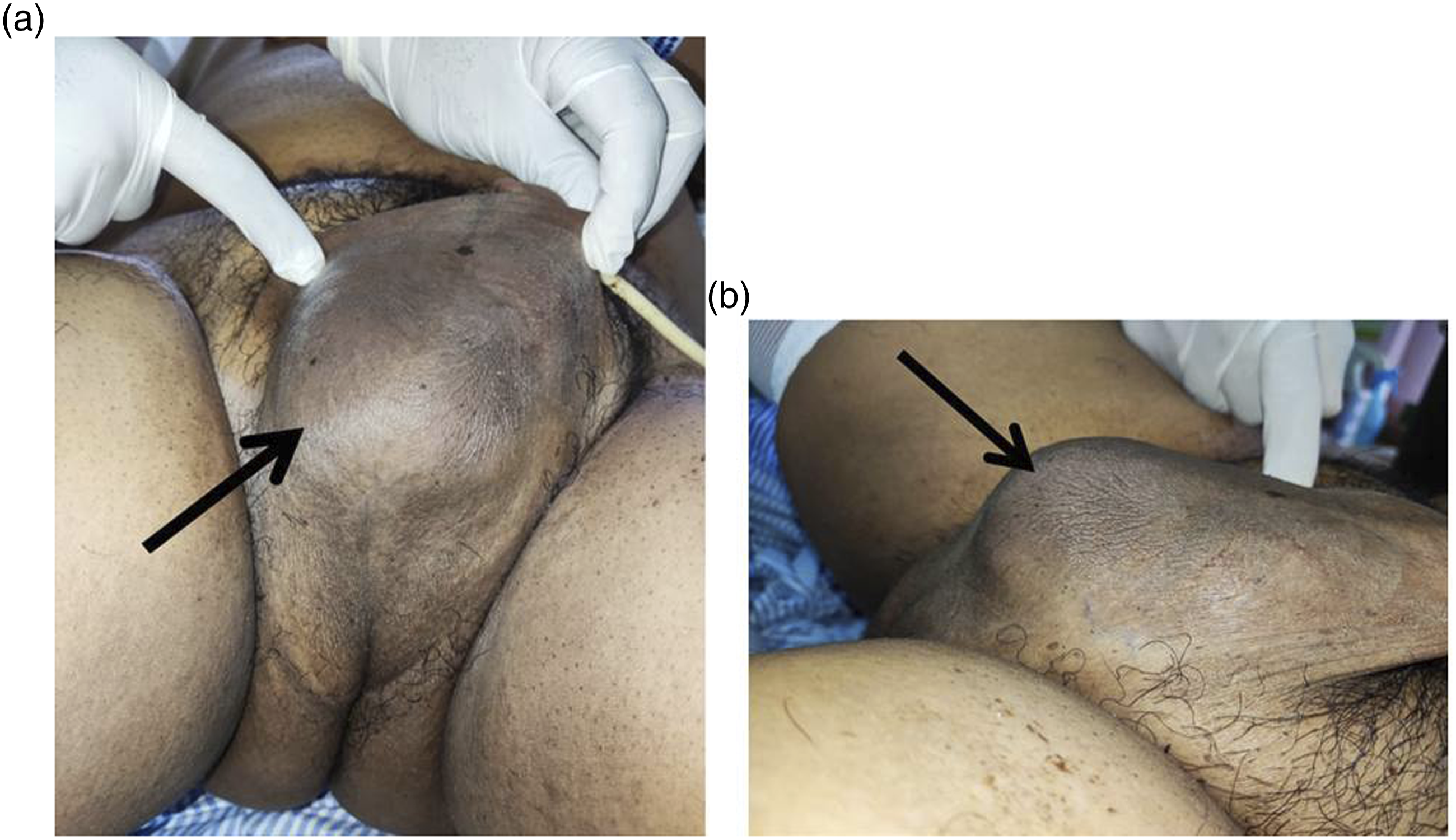
Laboratory investigations revealed raised total white cell count of 15000/mm3 and C-reactive protein 100 mg/L. Urine analysis nitrite and leucocyte were negative. Urine and blood cultures revealed no organism growth, penile swab no Neisseria Gonorrhoeae isolated. A MRI pelvis and penis showed a peripherally enhancing collection at the base of penis, measuring 7.5 (AP) x 4,0 (W) x 2.8 (HT) cm, this collection pools just beneath the penis with no evidence of fistulous connection to the penile urethra or peri-rectal or to subcutaneous layer (Figure 2(a) and (b)). (a) Axial T2-weighted Fat saturated shows a high signal collection (red arrow) at the right inferior aspect of the penis. (b) (Sagittal): Post contrasted T1 Fat saturation shows an irregular thick enhancing wall of the collection (rim enhancing) showed by red arrows.
He was then underwent debridement through midline perineal incision. Intra-operatively noted abscess 6 cm x 5 cm adjacent to the bulbar urethra (Figure 3(a)), pus evacuated and cavity washed thoroughly with povidone and normal saline. Bulbar urethra was not involved, no fistulous tract seen. A corrugated drain was placed post-operatively (Figure 3(b)). Finally the wound is closed loosely with several stiches of non-absorbable suture and cavity packed with saline soaked gauze. Post-operatively blood glucose levels were controlled and daily dermasyn dressing done over the wound. Corrugated drain was removed prior to discharge from hospital. The perineal wound was allowed to heal by secondary intention with weekly wound inspection in outpatient clinic. At 2-month follow-up, the perineal wound well-healed, patient has no experience of erectile dysfunction, no penile deviation, or recurrent abscess. Intra-operative pus culture grew Klebsiella Pneumoniae, no acid fast bacilli (AFB) seen and negative for Mycobacterium Tuberculosis culture. (a): Intraoperative photograph of fluctuating abscess at base of penis (black arrow). Pus aspiration sent for culture and sensitivity test. (b): Intraoperative photograph showing the abscess cavity post debridement and washout (solid arrow). Corrugated drain (dotted arrow).
Discussion
To our knowledge, our case is the first report of isolated base of penile abscess. There was no identifiable aetiology for this spontaneous base of penile abscess. Examination of genitalia and perineum showed absence of bite mark, no signs of abrasion or trauma and no open wound seen. Source of bacteria inoculation remains unknown. However, he had poorly controlled diabetes mellitus which can be considered a risk factor causing him to be prone to infection. A comprehensive literature review of 23 reported cases of penile abscess by Dugdale et al. 1 reckoned that over one-third of reported cases were spontaneous, and diabetic patients accounted for 25% of all reported cases. Strict control of diabetes mellitus is crucial for control of infection in our patient, and minimise recurrence in the future.
For patient presenting with penile discharge, scrotal pain or swelling, we should not miss out on performing digital rectal examination, as it was too often neglected by clinicians. Weizberg et al. 10 reported a case of penile abscess from anorectal abscess extension. Digital rectal examination is pivotal in identifying anorectal abscess, prostate abscess and fistulae.
A pelvic MRI done revealed a T2 fat saturated hyperintense subcutaneous collection along the right inferior penile gland to the right perineum. On Post contrast T1 fat saturated acquisition, the collection demonstrates a thick irregular enhancing wall. On diffusion weighted imaging (DWI), the lesion appeared bright due to the restriction of diffusion. A low signal was seen on the apparent diffusion coefficient (ADC) map. Although in close proximity with the penis and adjacent muscles, the collection does not demonstrate extension into these structures, and it is confined to the subcutaneous fat without any fistulous connection to the adjacent skin.
Functional urological assessment such as uroflowmetry and post-void residual urine measurement are important to assess possible undiagnosed urethral stricture which could be predisposing factor for development of base of penis or periurethral abscesses.
In view of the deep location and extent of the abscess on pre-operative imaging, less invasive intervention such as imaging-guided aspiration and drainage will not be feasible and inadequate to evacuate and wash the cavity effectively. Our goals in the management of this patient were to completely debride all infected and unhealthy tissue, thorough washout of the cavity, and to minimise functional impairment after wound healing. Transperineal incision and debridement of penile cavernousal abscess has been described by Bradley. 2 Open transperineal incision favoured sufficient exposure of perineal pouch, as well the bulbar urethra and cavernousal bodies, which allowed for extensive debridement of involved tissue and more accessible space for repair of urethra if required. An indwelling urinary catheter was inserted prior to surgery to aid in identification and protection to urethral intra-operatively. A corrugated drain was placed as it showed lower incidence of abscess recurrence and fistula development post-operatively. 12 Corrugate rubber drain is a type of open passive drain which causes less pain to the patient, is effective in eliminating dead space, with rubber inducing intense reaction allowing tract formation, help appose skin and quick wound healing. 12 In a retrospective study by Patel et al. 13 described corrugated drain as easy to use, inexpensive and readily available, which also proved significant reduction of wound complication, increased patient compliance, and reduced length of hospital stay.
There were literature references showing that less invasive intervention techniques may render lower risk of long term sequalae such as erectile dysfunction, cavernousal fibrosis and penile deviation. Thanos et al. 14 reported a case of cavernousal abscess that was successfully treated with CT-guided aspiration and pigtail drainage, which performed under local analgesia, and patient recovered from complete resolution of the abscess. However in our reported case, given the deep location and size of abscess, plus concern of abscess recurrence from incomplete debridement, open incision and drainage remains the mainstay of management.
Klebsiella pneumonia was isolated from the pus culture which was sensitive to our empirical antibiotic therapy. Infections with K. pneumoniae are usually hospital-acquired and occur primarily in patients with impaired host defenses (eg: diabetes mellitus, alcoholism, renal failure, malignancy). Common associated site of infection includes urinary tract, pulmonary, liver and bloodstream. 15 In a literature review of 23 case reports of penile cavernousal abscess by Dugdale et al. 1 noted that typical causative organisms include Staphylococcus aureus, Streptococci, Bacteroides and Enterococci. While Klebsiella was identified to be the causative organism in only 1 of the 23 reported cases.
Conclusion
Penile abscess is uncommon infection with potential for serious morbidity. A high index of suspicion is needed to look for possible causes such as extension of abscess from perineum or anorectal, sexually transmitted disease and tuberculosis. Apart from imaging, functional urological assessments are important to further determine the predisposing factors of penile abscess. Surgical drainage and debridement is the standard management with systemic antibiotic therapy. Pre-operative patient counseling is crucial with regard to the post-operative erectile function and appearance of genitalia. Proper diabetic education plays a vital role in treating and minimizing recurrent infection.
Footnotes
Acknowledgements
The authors would like to thank the Director-General of Health Malaysia for the permission to publish this article.
Author contributions
Lian Thai Lee wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Availability of data
The data and information of this case report are available from main author Lian Thai Lee.
Ethical approval
Hospital Sultanah Aminah does not require ethical approval to case report because standard management was given to patient, written consent was obtained from patient, and this case is not included in any clinical trials.
Informed Consent
Written informed consent for this paper (including images, case history and data) were obtained from the patient for publication of this paper, including the accompanying figures