
Abstract
Background
The clinical education of medical students relies on having direct patient experiences, which can be challenging when the patient population speaks multiple languages. In Singapore, students regularly encounter patients with whom they do not speak the same language.
Objective
The purpose of this study was to examine the role of student–patient language discordance (SPLD) on students’ clinical education experience.
Methods
In this sequential mixed-methods study, medical students who have completed at least 1 year of clinical education at the Duke-NUS Medical School in Singapore were asked to complete an online survey to obtain their self-reported language proficiency in local languages, experiences interacting with patients who do not speak English, and perceptions of the impact on clinical learning. A follow-up interview with selected participants was conducted.
Results
Overall, 35.9% of eligible students responded to the survey. Demographic analysis of respondents adequately represented the school’s overall student population. Non-Mandarin-speaking respondents reported that learning medicine in a multilingual environment negatively impacts clinical learning due to significantly more frequent challenges to clerking patients and feeling hindered from learning from doctors due to language barriers. However, no difference was observed in the performance on clinical exams of the three groups. Qualitative interviews uncovered possible reasons for the confounding results and two interrelated themes that highlight clinical learning experiences and challenges in a multilingual environment.
Conclusion
Students perceive SPLD as a hindrance toward their clinical education experience. Follow-up interviews uncovered the quandary of using translators and how language discordance impacts student’s professional identity formation.
Introduction
Medical education consists of both pre-clinical and clinical phases. During the pre-clinical phase, medical students learn from textbooks, lectures, and oftentimes simulated patient experiences. During the clinical phase, medical students consolidate knowledge from the pre-clinical phase and apply it in real-life by interacting with patients and clinicians. The development of a student’s clinical acumen can be impacted by many factors, including personal characteristics (such as social and communication skills), the instructional methodology, simulated practice, and real-life patient-care experiences.
While pre-clinical instruction can be more easily standardized, clinical education can be much more variable for students. One reason for this variability is related to the patient population that students are exposed to, given the various medical conditions that present to different hospitals and at different times, and by population heterogeneity as a whole. For example, in communities with a high prevalence of patients that do not speak the predominant language of the community, students must learn to adapt in order to learn from their patients and in order to contribute to providing safe and high-quality clinical care.1,2 This requires effective communication skills, which is why communication skills training is a major part of clinical education. 3 In addition to the formal training, medical students further learn communication skills by observing the communication styles and practices of other healthcare workers and students, and most importantly, by interacting with patients and having real-life experiences communicating with patients in the wards and clinics. For students that do not speak many of the languages of a diverse community, this represents a significant challenge. Anecdotally, students often suggest that communicating with patients that speak different languages is challenging, time consuming, and limits the quality of their learning.
Although some studies have been done on how classroom learning in one language but delivering care in another language affects medical students’ confidence in their history-taking ability, 4 no substantive data is available to suggest the effect of clinical education given student–patient language discordance (SPLD), where a medical student encounters a patient with whom they do not share a common language.
Therefore, the objective of this research is to examine the role of SPLD on medical students’ clinical performance and educational experience. The central hypothesis for this research is that medical students who often encounter SPLD will be negatively impacted in their clinical learning, as demonstrated on their clinical work-based assessments and end-of-first clinical year final summative clinical performance exam.
Methods
Singapore is a polyglot society and has four national languages: English, Mandarin, Tamil, and Malay. According to the census of population conducted by the Singapore Department of Statistics in 2000, 5 and a more recent Singapore General Household Survey of 2015, 6 the top five languages most frequently spoken at home besides English were (in descending order): Mandarin, Malay, Hokkien/Teochew, Cantonese, and Tamil. Approximately 32–37% of households use English as the main language spoken at home, while the majority of the population continues to primarily speak in the other languages mentioned above. English at home is more prevalent among younger residents and those with university degrees. In contrast, older Singaporeans, those aged 65 years old and older, predominantly speak Chinese dialects or other native tongue besides English at home.
An email invitation was sent to all eligible students with a participation information sheet and a link to complete the 10-minute self-administered questionnaire to determine students’ perceptions of how or if SPLD has impacted their clinical education during their first year of clinical clerkships. Students had to enter their name and student ID number prior to consenting and completing the survey or opting out. A reminder email was sent a week later to eligible students who had not completed the survey and had not opted out of the study. At the end of the online survey, students who were willing to participate in an in-person in-depth interview were asked to provide their consent for future follow-up.
Data representing students’ clinical learning in the first clinical year was compiled, including work-based assessments completed by supervising physicians throughout the year of the students’ Accreditation Council for Graduate Medical Education (ACGME) competencies 3 : history-taking skills, physical examination (PE) skills, analytical skills, communications skills, medical knowledge, management skills, interprofessional skills, and professionalism. Finally, data from the summative end-of-year clinical performance exam (CPX2) was obtained. The CPX2 is conducted in-school with standardized patients and includes history taking, physical examination, and procedural stations.
In alignment with the conceptual framework of this study, the survey data was paired to student’s demographic information, pre-matriculation and pre-clinical grade information, and clinical performance grades as described above. We compared all quantitative data using appropriate nonparametric tests (e.g., chi-square tests, the Kruskal–Wallis test) or parametric (e.g., independent samples t-tests) where appropriate. All quantitative data was analyzed using SPSS version 26 (IBM Corp, Armonk, NY, USA) and Microsoft Excel 2016 (Microsoft Inc, Redmond, WA, USA).
Results
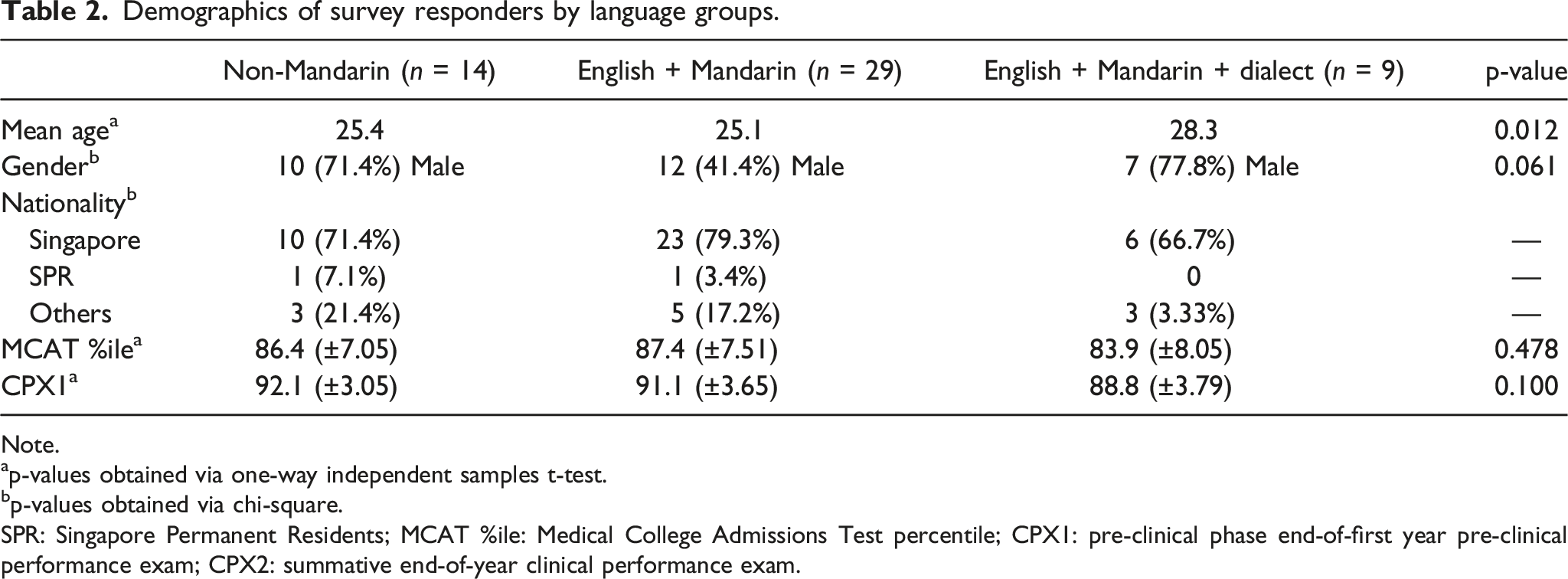
Demographics of survey responders.

Note.
ap-values obtained via one-way independent samples t-test.
bp-values obtained via chi-square.
SPR: Singapore Permanent Residents; MCAT %ile: Medical College Admissions Test percentile; CPX1: pre-clinical phase end-of-first year pre-clinical performance exam; CPX2: summative end-of-year clinical performance exam.
Based on the survey data of self-reported language skills, we coded each student into one of three groups: Respondents who were speakers of Mandarin and either of the Chinese dialects were grouped into the “English + Mandarin +Dialect” or Dialect group. Respondents who were speakers of Mandarin but neither one of the Chinese dialects were grouped into “English + Mandarin” or Mandarin. The rest of the respondents were grouped into “Non-Mandarin” group. There was no respondent who were speakers of a Chinese dialect but not a speaker of Mandarin. With regards to language proficiency, respondents who rated themselves as Advanced or Native Speakers of a language were coded as speakers and those who rated themselves as Intermediate or Beginner or None were coded as non-speakers. The percentage of languages spoken among respondents almost mirrored that of the Singapore population as mentioned above. We found that the languages with the most speakers among our respondents, aside from English, were (in descending order) as follows: Mandarin Chinese, Teochew/Hokkien, Cantonese, Tamil, and Malay (Figure 1). The three groups (Non-Mandarin, Mandarin, and Dialect) did not differ by gender, nationality, or academic performance as measured by pre-matriculation MCAT scores and Year 1 (pre-clinical) summative clinical examinations (CPX1) when compared to each other (Table 2), thus making adjusted analyses for these factors unnecessary. Language Proficiency of Respondents Demographics of survey responders by language groups. Note. ap-values obtained via one-way independent samples t-test. bp-values obtained via chi-square. SPR: Singapore Permanent Residents; MCAT %ile: Medical College Admissions Test percentile; CPX1: pre-clinical phase end-of-first year pre-clinical performance exam; CPX2: summative end-of-year clinical performance exam.
Respondents in all three groups similarly reported encountering a patient who did not speak English often, defined in the survey as once a day. Furthermore, they reported that aside from English, Mandarin was the language they most commonly have to use to speak to patients during their Year 2 clerkships, as compared to the other four local languages (Figure 2, Supplementary Table 1). This supports the Ministry of Health record of public hospital admission that shows an increase in hospitalization of older Singaporeans, who tend to be non-English speakers.
10
Non-Mandarin speakers reported that learning medicine in a multilingual environment negatively impacts clinical learning due to significantly more frequent challenges to clerking patients and feeling hindered from learning from doctors due to language barriers (Figure 3 and Figure 4, Supplementary Table 1). However, there was no statistically significant difference in the performance on the end-of-clinical year summative exam (CPX2) of the three groups. The non-Mandarin speaking group, however, did display higher ratings in the history-taking section of their work-based assessments as compared to the other two groups (p = 0.009). The non-mandarin group had lower ratings in the professionalism (p = 0.032) but received similar ratings for the remaining component of their CA, such as physical examination skills, communication skills, and medical knowledge (Table 3). Frequency of encounters with non-English speaking patients. Note: As measured on the following scale: 1 “Never”; 2 “Rarely (a few times a month)”; 3 “Occasionally (a few times per week)”; 4 “Often (once a day)”; 5 “Very Often (many times per day)”. p-values obtained via non-parametric Kruskal–Wallis test. Respondents were asked regarding their experiences with patients during their Year 2 clerkships. In particular, they were asked about the frequencies in which they encounter (a) non-English speaking patients, and of which predominantly spoke in (b) Mandarin Chinese, (c) Hokkien/Teochew, (d) Cantonese, (e) Malay, and (f) Tamil. Respondents’ experience with patients. Note: As measured on the following scale: 1 “Never”; 2 “Rarely (a few times a month)”; 3 “Occasionally (a few times per week)”; 4 “Often (once a day)”; 5 “Very Often (many times per day)”. p-values obtained via non-parametric Kruskal–Wallis test. Respondents were asked regarding their experiences with patients during their Year 2 clerkships. In particular, they were asked frequently they (a) were unable to clerk and learn from a patient due to language barriers, (b) were asked to interpret for patients, (c) actively avoided patients with whom they did not speak the same language with, and (d) felt hindered from learning from doctors during rounds/bedside tutorials due to language barriers. Respondents’ perception of impact of SPLD on their clinical education. Note: As measured on the following scale: 1 “Not at all”; 2 “Very Little”; 3 “Somewhat”; 4 “Very Much”; 5 “Extremely”. p-values obtained via non-parametric Kruskal–Wallis test. Respondents were asked regarding their perception of impact of SPLD on their clinical education in Year 2. In particular, they were asked how strongly they agreed with the following statements: (a) had less opportunities to learn from patients because of the languages they do not speak, (b) their lack of language skills negatively impacted the amount they learned in Year 2, (c) learning medicine in a multicultural environment negatively impacts clinical learning, and (d) often feel lost in rounds/clinics because of the languages they do not speak. Year 2 clinical performance grades. Note: To aid in interpretation, all data are displayed as means (+/-sd), although p-values were obtained via non-parametric Kruskal–Wallis test. aAs measured on the following scale: 1 “Does not meet basic expectations,” 2 “Occasionally Meets Basic Expectations,” 3 “Consistently Meets Basic Expectations,” 4 “Occasionally Exceeds Basic Expectations,” and 5 “Consistently Exceeds Basic Expectations”. bAs measured on the following scale: 1 “Did not meet expectations,” 2 “Met Expectations,” and 3 “Exceeded Expectations”. cAs measured on the following scale: 1 “Have reservations,” 2 “Recommend,” and 3 “Highly Recommend”.



Our survey showed that respondents in the Non-Mandarin group reported that learning medicine in a multilingual environment negatively impacts clinical learning due to significantly more frequent challenges to clerking patients and feeling hindered from learning from doctors due to language barriers. Nonetheless, there was no substantive evidence of clinical performance that substantiated this notion. Exceptionally, contrary to this study’s hypothesis, non-Mandarin speaking students received better ratings for their history-taking skills in their work-based assessments than compared to those who do speak Mandarin.
Thus, to further explore this unexpected result, we followed-up with a qualitative study so that we may attempt to fulfill the study’s objective to examine the role of student–patient language discordance on students’ clinical education experience.
“if you can only speak one language, then you cannot interview patients who speak other languages, yeah so therefore you get you don’t get exposed to the presentation that these patients come with” [P1].
The confounding results perhaps indicate that students perceive the assessments are not an accurate portrayal of real-life and that day-to-day fluency in a particular language does not equal to fluency in medical terms in that language. For example, exams are almost always conducted in English and employ standardized patients who are prompted to respond a certain way, as described: “CPX2 is very structured, is very organized and it’s very different from the wards, because patients present very non-complicated, the patients are not complicated in CPX2, they are very straightforward patients” [P8].
Despite the difference perceived, some students still see ward experience as beneficial preparation for school assessment; “(Clerking patients in the wards) helps (students) prepare (for CPX2) however, I mean definitely CPX2 is er exam is a exam setting, it is different from being in the wards, err yeah so given that although it is helpful it is not is not foolproof, I mean, we still need practice in exam settings” [P3].
This dichotomy may force students to choose between practicing for real life or practicing for the school’s exam. Instead of preparing for the exam in the wards, non-Mandarin speakers may instead practice with fellow classmates, resulting in their higher performance at school assessments, as described: “could be because, erm, a lack of skill of languages that (non-Mandarin speakers) spend less time in the wards possibly, and that they spend more time practicing with their peers” [P8].
Although non-Mandarin speakers may have “hacked” the school’s examination, participants of that group shared their worry on how they will perform as a doctor when they graduate. As students, they still have the luxury of picking, to a certain extent, which patients to clerk and not to clerk. House Officers (HOs), however, do not because “often times (HO) the first kind of erm you know point of call when patients come in and get admitted, (they) have to take a history and (they) have to rely on a translator or (they) have to rely on someone else to come help (them) out” [P5].
Furthermore, HOs no longer have the luxury of time and availability of classmates to help translate, as described: “once you’re a HO you’re dealing with efficiency and you know there are shortages of staff all the time, so I think perhaps it’s a little bit more erm difficult to find someone to help you out” [P5].
Almost all of the interview participants prefer to use English as the primary language to communicate with patients, when given the choice, because their medical education was in English. This is true even for those who claim to be fluent in other languages, including Mandarin Chinese. “Mandarin or Cantonese is like, are my first languages, and if you ask me to talk to a patient like in the ward right now, you ask me if I prefer English or Mandarin, I would say I prefer English, because that was, that’s how I, I was taught in Year 1 and so if you ask me to to clerk a patient in Mandarin, I think it would be worse, in, I mean like, than than if I clerk yeah I clerk in English, yeah” [P6].
This response was shared across participants regardless of which additional local language they were fluent in. When probed further, they explained that “knowing the accurate medical terms in another language,” was the main challenge [P4].
“definitely better than not being able to talk to the patient at all” [P7]. “the presence of the interpreter actually gives (students) that opportunity to learn from the patients” [P9].
“If (they) didn’t have that person to help (them) translate, then that’s a like a completely loss opportunity” [P5].
This is particularly essential when encountering a rare condition, where the student otherwise would not be able to speak with without a translator. Even for seemingly common conditions, one participant noted the importance of having access to as many patients as possible since: “every patient presents differently, so every patient becomes a learning opportunity. I could’ve found easily found another case with a similar disease profile, but sometimes you wanna learn a story from that patient’s perspective” [P8].
Thus, although language discordance can be mitigated by the presence of translators, it comes at a cost of the quality of information.
All nine participants had used translators at least once during Year 2. Most often, participants had nurses or other medical students to act as translators. Less frequently, participants had doctors or the patients’ family members to translate. None of the participants had engaged the services of a professional translator. As a result, participants note that some information is missed or lost in translation, as described: “whether the person who is translating actually conveys the actual meaning of what (participants) want to bring across” [P3]. “(students) still are not very sure of whether what (they) say to the interpreter is it exactly the same as what the interpreter talk to the patient” [P6].
This uncertainty of lost in translation is compounded with another downfall of using untrained translators. Since most of the translators recruited by participants are medical professional (nurses, other medical students, or on the rare occasion doctors), participants noted that most of the translators may indirectly, or directly, apply a “medical filter” on the patient information and translate what they deem is important. Participants who have acted as translators admit that they too are guilty of applying their own “medical filter” when translating. When asked about one of the challenges of acting as a translator, a participant shared: “challenge one is should you interpret word for word or should you do the interpretation for the person that you are translating for. The risk is that if you do word for word everyone will get confused, I would to, versus if I do the thinking for the person and interpret it for the person that what information is there missing in the translation” [P2].
Thus, students employing non-professional translators may not get to hone their history-taking skill and instead receive information that has been prepacked to fit into certain diagnoses.
In addition, students would need to go over the first hurdle of finding a translator, as described: “I think, actually the main challenge is finding an interpreter, because, erm mainly when I need an interpreter is when I clerk the patient on my own in the morning, so I won’t have any, like classmates around, and the doctors are all busy with their own work, and the nurses are busy also” [P9].
Another drawback how using translators is time consuming, as described: “It takes a lot longer to get a history […] if you have to rely on a translator, who is like you know clarifying every other second, it just takes way longer, at least double the time, to get a good history” [P5].
Some participants shared that they were more enthusiastic about using translators earlier in their clinical education but later adapted to avoiding SPLD. One participant shared that they “consciously avoid the language barrier” [P9] as “the whole trouble of taking time out to find the interpreter and then, erm, having to prolong the whole history taking process because you have to talk to, speak to the interpreter, who then speak to the patient, and also, perhaps even like deterring from taking history from the patient because the patient doesn’t speak your language, so you’re just like, ‘ok never mind, I will just give up on this patent, I will just find another patient’” [P9].
When students encounter SPLD, they have a choice to make—to find a translator and take more time to learn from that patient whilst potentially receiving an incomplete picture or to miss out on the learning opportunity that patient provides.
At the same time, should they decide not to use translators because of the various drawbacks mentioned above, students find themselves “segregate(ing) patients by people (students) can clerk and cannot clerk” [P7] based on language discordance. In doing so, students may find themselves to a biased group of patients, specifically clerking English-speaking patients. Participants note that patients who do not speak English tend to be older and less educated, affirming the demographics from Singapore Household Survey. With a bias toward younger patients, non-Mandarin speaking students miss out on an entire patient population since “older patients (who) tend to be sicker and because they are sicker they tend to have more signs, clinical signs, so if you wanted to you know observe a patient who has really really you know informative clinical signs and or like really really good history of natural course of disease” [P5].
This may also lead to the loss of some of the nuances of the socio-economical and sometime psychological background and the “big picture” of the patient. Communication is key in the medical field, and although socio-economic and psychological information can seem trivial, they can paint a better picture of the patient and can sometime provide important factors to the patient’s condition.
“the art side of medicine, when they know that they are being listened to and someone actually cares enough to try and make an effort to connect” [P7].
Having empathy toward patients benefits both patient and medical student. When the patient feels attended and cared for, they are more likely elaborate more on their medical history or be more willing to let students examine them, as described: “being able to communicate with the patient one-to-one is the best because you can form a rapport, the patient will be more than happy to share or divulge little details, they will also be more likely to humor you when you (ask them to do certain maneuvers for physical examination)” [P5] “having that familiarity of language facilitates (the patients) to expound on their history, tell you a little bit more about history, because they’re just more comfortable using certain language, figures of speech, to get the message across” [P8].
Using a translator affects rapport building because as one student shared: “talking to (patients) indirectly through a mediator, erm you definitely lose that connection that you’d get when you speak to someone heart to heart, when you have like a one-to-one, so not being able to perform that bond or like that sort of connection with the patients is I think in of itself you’re basically creating a barrier” [P5].
After all, patients do not want a robotic doctor with whom they do not feel can empathize or “share a common ground” with [P5]. The number of local languages a medical student can speak therefore affects both quantity and quality of patient interaction. While this may not impact students’ medical knowledge as much, it does impede medical students’ professional identity formation, specifically as a member of a caring profession, as recounted: “I think the most impact it would have would be to understand more the not, less so the biomedical factors of a patient but more so the social and psychological factors of a patient” [P4].
Another aspect of the formation of a medical student’s professional identity is for them to feel like a member of the healthcare team. One way is for medical students to help the team by clerking less complicated patients to alleviate their busy workload. One participant reported: “(Medical students) want to feel like (they’re) contributing to the team rather than being an additional like burden or whatever” [P7].
However, by needing translation, low-local-language-capacity students may burden their teammates by not being able to clerk the patient or worse, taking out the team’s time to help them with translation to facilitate their learning.
Low-local-language-capacity students also reported feeling inadequate and hindered by their language limitations. They recognize as future physicians their duty is first and foremost to consider the safety of their patient; if their language limitations prevent them from thoroughly understanding their patients, or as a student recounted not “(appreciating) the nuances in the patient response” [P7], they might be unable to get a full picture or miss out on the diagnosis or complications. Thus, they acknowledge that they should let others clerk the patient because patient safety is most important: “at the crux of it, is to evaluate a patient safely and professionally” [P8].
Discussion
As William Osler famously said, “To study the phenomena of disease without books is to sail an uncharted sea, while to study books without patients is not to go to sea at all”. What differentiates clinical learning from pre-clinical learning in a medical students’ education is often the presence of a real-life patient rather than a standardized patient. This is because clinical education is not just about knowledge and skill acquisition, but also the formation of professional identity of clinicians. Interacting with real-life patients and witnessing how the medical team manages both the biomedical and psychosocial aspects each patient presents with give medical students a glimpse of their future role as a medical professional. By stepping into the wards, they step out of the controlled scientific part of medicine and into the organic humanistic part of medicine. Students are to learn how to care for the patient not just for their physical ailments but also building a therapeutic relationship with them.
Our study shows that students perceive SPLD as a hindrance toward their clinical education experience. Our qualitative study further revealed that although high-local-language-capacity students do not feel hindered by SPLD personally, they felt that their low-local-language-capacity was negatively impacted. Despite their perceptions, the first part of our study suggests that studying medicine in a multilingual environment has no apparent, measurable impact on student’s clinical performance, as shown by their clinical examinations results. However, our follow-up qualitative study suggests that this could be due to students “gaming” the examination system by spending more time studying textbooks or practicing with fellow classmates instead of learning in the wards and thus not necessarily an accurate representation of how SPLD affects their clinical learning experience. This also highlights the variability of learning clinical knowledge for students and the potential danger of having students’ ace exams but using Osler’s analogy, fail to successfully set sail at sea.
The qualitative part of our study shows that when studying medicine in a multilingual environment, students experience a quandary toward using translators. Participants understood the importance of being multilingual and some even actively seek to improve communication skills by learning new local languages. They note feeling inadequate and being a hindrance when they were not able to communicate effectively when encountered with SPLD. This is further expounded quandary toward translating as it provides them with additional patients at the cost of the quality of patient interactions, highlighting that untrained translators do not adequately bridge the communication gap between healthcare providers and their patients. This feeling of inadequacy may affect their professional identity as a future physician.
Limitations of Research and Implications for Future Research
The results of this study raise interesting and important questions for future investigations, such as: How do medical students adapt over time to student–patient language discordance? How does student–patient language discordance impact students’ professional identify formation? These topics would be especially well-suited for a longitudinal study that examines students’ performance when they graduate and enter the workforce, during which they can no longer choose to avoid certain patients or “game” the system by practicing more for exams.
While provocative, the results of this study must be viewed with full appreciation of its strengths and limitations. First, while Singapore makes for an excellent location to study this topic given its polyglot society, the study was conducted at a single institution with a small sample size and a low response rate to the survey. Despite the low response rate, our demographic analysis indicated that the respondents adequately represented the schools’ overall student population.
Supplemental Material
sj-pdf-1-psh-10.1177_20101058221077797 – Supplemental Material for Language Discordance Between Students And Patients: Impact On Clinical Learning
Supplemental Material, sj-pdf-1-psh-10.1177_20101058221077797 for Language Discordance Between Students And Patients: Impact On Clinical Learning by Felicia Rustandy, Foo Yang Yann, and Scott Compton in Journal of Proceedings of Singapore Healthcare
Footnotes
Acknowledgments
Dr Fan Qiao for statistical mentorship and Ms June Lee for her help in the administrative aspect of this research work. Finally, I wish to thank the students who participated in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Authors’ contributions
FR and SC conceived the study topic and design and analyzed and interpreted data. FYY assisted in design and analysis and interpretation of data. All authors take full responsibility for the manuscript.
Informed consent
Informed consent was obtained for the qualitative interviews
Ethical approval
This study was approved by the NUS Institutional Review Board
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.