
Abstract
Introduction:
This paper compares the usage of inhaled methoxyflurane versus traditional procedural sedation and analgesia for manipulation and reduction of acute shoulder dislocation and acute elbow dislocation in the emergency department.
Methods:
This was a retrospective observational study of patients who presented with either acute shoulder dislocation or acute elbow dislocation to an adult tertiary emergency department between 1 April 2018 and 30 September 2019 and underwent manipulation and reduction with either methoxyflurane or procedural sedation and analgesia. Primary outcomes of patients’ length of stay in the emergency department and secondary outcomes of duration of procedure and success of reduction on first attempt for inhaled methoxyflurane were compared against those of procedural sedation and analgesia.
Results:
A total of 192 patients were included in this study; 74 patients underwent reduction with methoxyflurane while 118 patients (85 acute shoulder dislocation and 33 acute elbow dislocation) underwent reduction with procedural sedation and analgesia. The median length of stay in the emergency department was significantly shorter (P<0.001) for the methoxyflurane group (99 minutes, interquartile range (IQR) 136.8 minutes) versus the procedural sedation and analgesia group (246.5 minutes, IQR 163 minutes). The median duration of procedure in the emergency department was also significantly shorter (P<0.001) for the methoxyflurane group (16 minutes, IQR 17 minutes) versus the procedural sedation and analgesia group (32 minutes, IQR 40.3 minutes). There was no significant difference in reduction on first attempt between the two groups.
Conclusion:
The use of inhaled methoxyflurane in the manipulation and reduction of acute shoulder dislocation and acute elbow dislocation was associated with a shorter patient length of stay and a shorter duration of procedure, while no significant difference was observed in the success of reduction on first attempt when compared to procedural sedation and analgesia.
Keywords
Introduction
Manipulation and reduction (M&R) of joint dislocations are common procedures in the emergency department (ED). They are often painful and are usually performed under procedural sedation and analgesia (PSA). PSA often involves observing the patient post-procedure for recovery and complications that may take hours. Moreover, PSA carries non-negligible cardiovascular risks and is resource consuming. 1
Methoxyflurane belongs to the fluorinated hydrocarbon group of volatile anaesthetic agents. At low concentrations, it can be used as an analgesic in haemodynamically stable and conscious patients. 2 It is inhaled by way of the pre-designed Penthrox inhaler and its use has been studied in Singapore’s pre-hospital setting. 3 Methoxyflurane has been recommended by the emergency medical services (EMS) medical advisory committee as a first line analgesic in the pre-hospital setting.
Methoxyflurane has been used extensively, primarily in Australia but more recently in Europe, as a self-administered, rapidly acting inhaled analgesic agent.4,5 It has been shown in multiple studies rapidly to provide effective analgesia and potentially reduce patient length of stay (LOS).5,6 Methoxyflurane has been shown to reduce anxiety during colonoscopies and its main side effect has been drowsiness which resolves within 30 minutes. 7 As such, this is a drug which needs minimal further monitoring after administration and concerns about airway compromise, as compared to PSA, are negligible. 8 This may contribute to reduced manpower and resource utilisation (e.g. resuscitation bay usage), and better patient flow within the ED.
The aim of this study was to assess whether M&R of acute shoulder or elbow dislocations with inhaled methoxyflurane would reduce ED LOS when compared to traditional PSA. The secondary outcomes studied were the duration of procedure (DOP) and first-time success rate (FSR) in reduction of the acute dislocations.
Methods
Study design and setting
This was a retrospective observational study involving all patients presenting with either acute shoulder dislocation (ASD) or acute elbow dislocation (AED) between 1 April 2018 and 30 September 2019. The ED belongs to a tertiary hospital with an annual ED attendance of 140,000 patients. Based on institutional guidelines, this study was exempted from review by the centralised institutional review board (CIRB).
Study population
All adult patients (>16 years), who underwent reduction of shoulder or elbow dislocation with either inhaled methoxyflurane or PSA in the ED were included. Patients with reduction prior to arrival in the ED, in whom no medications or only intravenous analgesia were used, and in whom M&R was not attempted were excluded.
Data collection
SNOMED clinical terms were used to shortlist patients with ED discharge diagnosis of shoulder or elbow dislocation (Supplementary Annex A) within the study period. Two researchers then reviewed the electronic medical records and extracted relevant data using a standardised form.
Patient demographics, site of dislocation, history of prior dislocation, triage category, drugs utilised for procedure, experience of procedure doctor, success at first attempt, DOP (start of procedure to the X-ray confirmation of successful reduction) and total LOS in the ED (time from triage to discharge or admission) were derived from patients’ electronic medical records.
Institutional practice
In this institution, the decision regarding the need for sedation, the method used for M&R and the drugs used are left to the treating physician’s discretion. A shared decision is usually made with the patient on the need for sedation, options and risks.
There are two broad categories of short-acting sedative agents (SSAs) available in the department: (a) sedative agents with duration of action up to 1–2 hours (i.e. midazolam at 0.1–0.2 mg/kg); and (b) sedative agents with duration of action up to 30 minutes (i.e. etomidate at 0.2–0.3 mg/kg, propofol at 1–2 mg/kg and ketamine at 1–2 mg/kg). Sedative agents are given in small intravenous boluses and titrated according to the Ramsay sedation scale (RAS) or Richmond agitation–sedation scale (RASS) corresponding to light sedation. For the administration of methoxyflurane, it is a self-administered analgesia by patients with instructions and guidance from the nurses. Patients are instructed to inhale and exhale to reduce their pain to a manageable level, usually achieved in six to 10 breaths. Doctors will then assess if the level of pain relief provided is enough for the patient to proceed with the M&R or instead to choose PSA for the patient.
Department protocol mandates a maximum of two attempts at reduction by the ED team, before a referral to the orthopaedics team is made, for assistance. All M&Rs that require sedation are performed in a monitored area in the resuscitation bay in the presence of at least three staff members (charting nurse, doctor performing the PSA and the doctor performing the M&R). Post M&R, an X-ray is performed to confirm reduction of the dislocated joint.
Thereafter, the patient is placed in an observation area for monitoring. The patient is discharged to the care of a responsible adult only when fully conscious with a Glasgow coma scale score of 15 and stable vital signs. Otherwise, the patient is admitted to the ward for longer monitoring.
Outcome measure and statistical analysis
The primary outcome was the ED LOS and the secondary outcomes were DOP and FSR in reduction of the acute dislocations. Comparison was made between two groups – methoxyflurane versus PSA. IBM SPSS was used for statistical analysis. The Mann–Whitney U-test, t-test and chi-square test were used to assess for significant differences among groups for continuous variables with non-parametric and categorical variables, respectively. P values of less than 0.05 were taken as significant. No a priori sample size calculation was done in this study.
Results
Baseline characteristics
A total of 279 patients (231 ASD and 48 AED) presented to the ED during the study period. One hundred and ninety-two patients fulfilled our inclusion criteria (Figure 1). There were no patients who had concomitant ASD and AED. The patient characteristics and associated variables for the three groups are shown in Table 1. There were more patients in the PSA group (n=118) than the methoxyflurane group (n=74). There was also a greater proportion of patients with elbow dislocation in the PSA group (28%) than the methoxyflurane group (8.1%). This suggested a preference by the department physicians for PSA in general. Under our PSA group (n=118), 39 patients received midazolam and 79 patients received other SSAs such as ketamine, propofol or a combination of both (ketofol).

Study flowchart.
Baseline characteristics of patients.
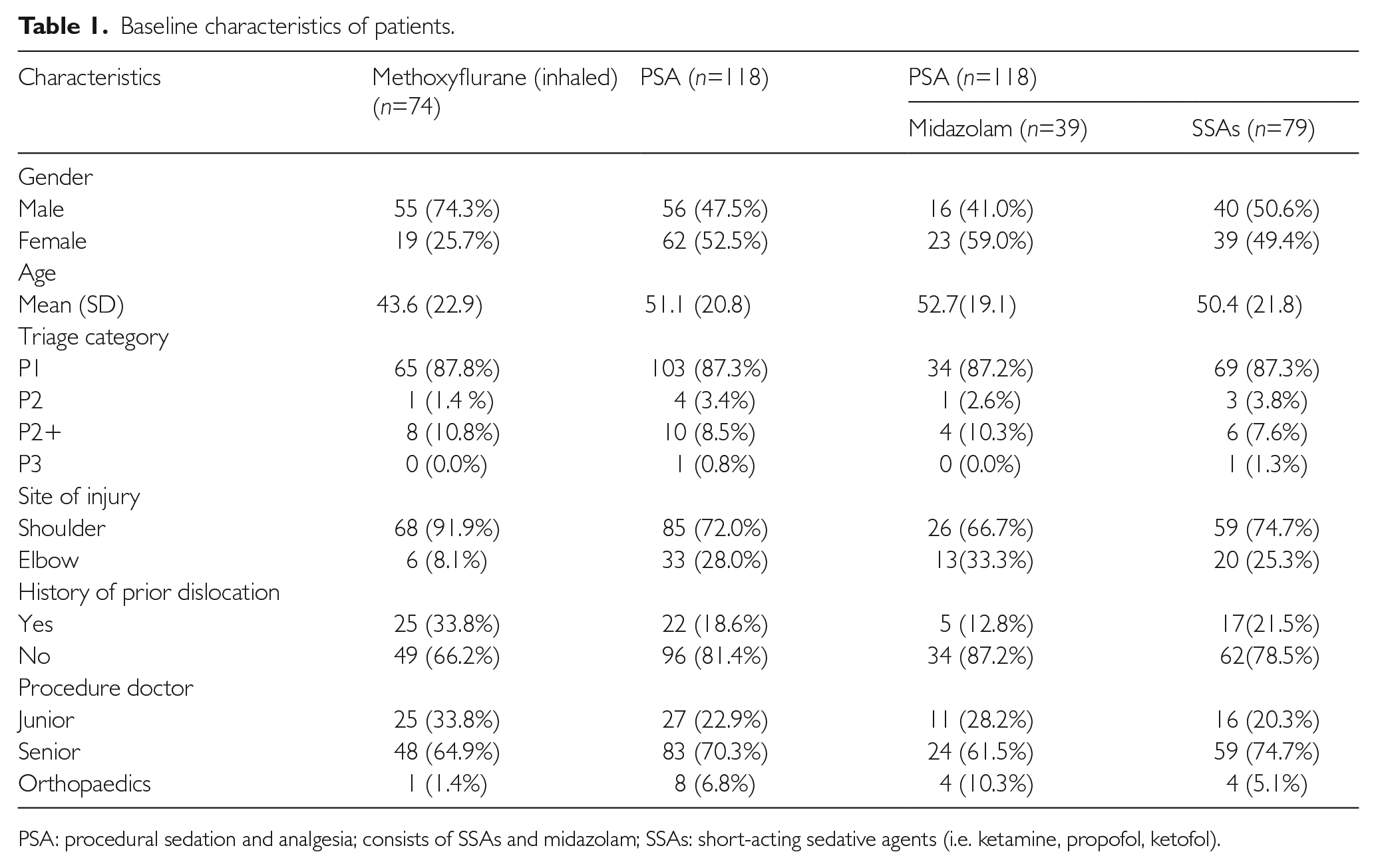
PSA: procedural sedation and analgesia; consists of SSAs and midazolam; SSAs: short-acting sedative agents (i.e. ketamine, propofol, ketofol).
The procedure doctors for both groups were mostly senior doctors (methoxyflurane 65% vs. PSA 71%). Senior doctors included fourth or fifth-year emergency medicine trainees or emergency physicians. Junior doctors were non-trainees or trainees in their first 3 years of training.
Study outcomes (methoxyflurane vs. PSA)
Seventy-four patients underwent reduction with methoxyflurane while 118 patients underwent reduction with PSA. The results of our primary analysis are displayed in Table 2. The median LOS in the ED was significantly shorter (P<0.001) for the methoxyflurane group (99 minutes, interquartile range (IQR) 136.8 minutes) than the PSA group (246.5 minutes, IQR 163 minutes). The median DOP in the ED was also significantly shorter (P<0.001) for the methoxyflurane group (16 minutes, IQR 17 minutes) than the PSA group (32 minutes, IQR 40.3 minutes). Finally, there was no significant difference in first success reduction between the two groups.
Comparison of primary and secondary outcomes between methoxyflurane and PSA.

ED: emergency department; IQR: interquartile range; LOS: length of stay; PSA: procedural sedation and analgesia; consists of other short-acting sedative agents (i.e. ketamine, propofol, ketofol) and midazolam.
Subgroup analysis (methoxyflurane vs. midazolam vs. SSAs)
We also present a three-way comparison of methoxyflurane versus midazolam versus SSAs in Table 3 to see if the choice of SSAs of different duration of action affects our study outcomes. The median LOS in the ED was also significantly shorter (P<0.001) for the methoxyflurane group (99 minutes, IQR 136.8 minutes) than the midazolam group (277 minutes IQR 137 minutes) than the SSA group (229 minutes, IQR 173 minutes). The median DOP in the ED was likewise significantly shorter (P<0.001) for the methoxyflurane group (16 minutes, IQR 17 minutes) than the midazolam group (33 minutes, IQR 55 minutes) versus the SSA group (30 minutes, IQR 35 minutes). Finally, there was no significant difference in first success reduction among the three groups.
Comparison of primary and secondary outcomes among methoxyflurane, midazolam and SSAs.
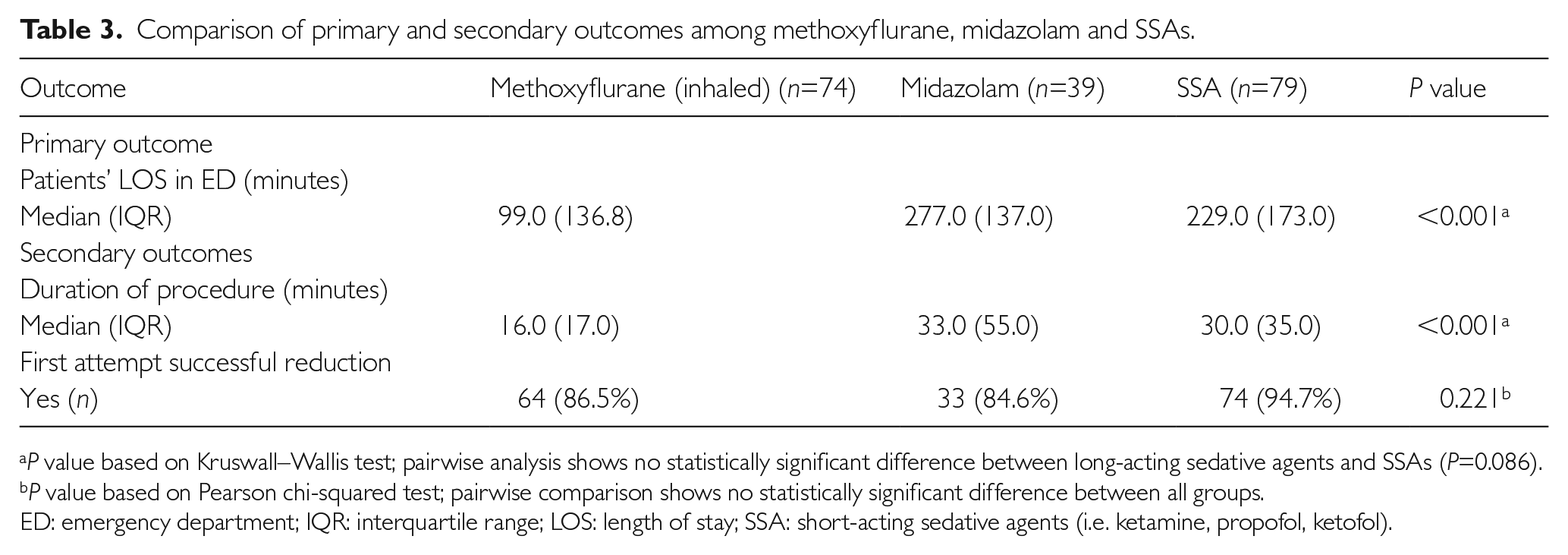
P value based on Kruswall–Wallis test; pairwise analysis shows no statistically significant difference between long-acting sedative agents and SSAs (P=0.086).
P value based on Pearson chi-squared test; pairwise comparison shows no statistically significant difference between all groups.
ED: emergency department; IQR: interquartile range; LOS: length of stay; SSA: short-acting sedative agents (i.e. ketamine, propofol, ketofol).
Discussion
Our retrospective study showed that the usage of methoxyflurane is associated with shorter ED LOS and DOP among patients with ASD and AED, while there was no significant difference in the success rate at the first attempt, with either methoxyflurane or PSA, regardless of the choice of sedative agent. Of note, further pairwise analysis also shows no statistically significant difference in the median ED LOS between midazolam and SSAs (P=0.086).
Based on our experience, there could be multiple factors for increased ED LOS in the PSA group, with the most likely one being longer post-procedure monitoring required in the PSA group. Other factors such as the availability of drugs from the ED pharmacy and manpower for the monitoring of patients are largely similar for both groups, as this observation study was done in the same department. This is a limitation and it may be useful to include a breakdown of ED timings (e.g. overall ED LOS, time to procedure, DOP, post-procedure monitoring duration) in future studies.
The other limitation of this study lies in its retrospective nature and its reliance on documentation by doctors and nurses. Baseline characteristics were uneven between the two groups reflecting high selection bias. The varied practice of the emergency physicians may have contributed to an imbalance in the numbers in the two groups (PSA 118 vs. methoxyflurane 74), reflecting a strong preference for procedural sedation over the usage of inhaled methoxyflurane. Patients with a history of prior dislocation were also more prevalent in the methoxyflurane group (33.8% vs. 18.6%). It may be easier to reduce dislocated joints in patients with a previous history of dislocation, which may have had a positive effect on DOP in the methoxyflurane group.
There were no adverse events reported for either group of patients; however, it is well known that adverse events are under-reported. Patients’ pain score data were incomplete and hence we were unable to draw any conclusions on this aspect. There were insufficient data regarding the number of staff involved in the procedure when methoxyflurane was used, which meant that we could not actually see if the use of methoxyflurane reduced the strain on manpower.
To date, there are no studies comparing the use of methoxyflurane with PSA in the M&R of ASDs and AEDs on ED LOS as the primary outcome. Umana et al. studied the use of inhaled methoxyflurane in the ED but their main aim was to assess the success rate of reduction of only anterior shoulder dislocation when compared to propofol. 6
No power size sample calculation was done a priori for the study power. There is a chance that the study may be underpowered to detect a statistically significant difference (Type II error). However, in this study, a statistically significant difference in ED LOS was detected. Prospective research that can produce a higher quality of evidence to validate the observed beneficial association on ED LOS seen in using inhaled methoxyflurane is definitely required. We would suggest for the future study to measure methoxyflurane versus a single sedation agent to reduce the clinical heterogeneity in the sedation group. The safety profile of the two methods should also be looked into in the future study.
Supplemental Material
sj-docx-1-psh-10.1177_2010105821993493 – Supplemental material for Comparison of inhaled methoxyflurane versus procedural sedation for manipulation and reduction of acute shoulder and elbow dislocation in the emergency department
Supplemental material, sj-docx-1-psh-10.1177_2010105821993493 for Comparison of inhaled methoxyflurane versus procedural sedation for manipulation and reduction of acute shoulder and elbow dislocation in the emergency department by Shu Fang Ho, Sameera Ganti, Eunizar Omar, Sherman Wei Qiang Lian, Hui Cheng Tan, Yogeswary Pasupathy, Norizan Jaafar, Faraz Zarisfi and Marcus Eng Hock Ong in Proceedings of Singapore Healthcare
Supplemental Material
sj-docx-2-psh-10.1177_2010105821993493 – Supplemental material for Comparison of inhaled methoxyflurane versus procedural sedation for manipulation and reduction of acute shoulder and elbow dislocation in the emergency department
Supplemental material, sj-docx-2-psh-10.1177_2010105821993493 for Comparison of inhaled methoxyflurane versus procedural sedation for manipulation and reduction of acute shoulder and elbow dislocation in the emergency department by Shu Fang Ho, Sameera Ganti, Eunizar Omar, Sherman Wei Qiang Lian, Hui Cheng Tan, Yogeswary Pasupathy, Norizan Jaafar, Faraz Zarisfi and Marcus Eng Hock Ong in Proceedings of Singapore Healthcare
Footnotes
Acknowledgements
The author(s) would like to thank authors 4 to 8 for their assistance and guidance in this research.
Authors’ contributions
Authors 1 and 2 researched the literature and conceived the study. Authors 1, 2 and 4 were involved in the development of study methodology and data collection. Authors 3 and 5 were involved in the data analysis. Authors 1, 2 and 3 wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Availability of data and materials
The datasets generated and/or analysed during the current study are available from the corresponding author.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study institution does not require ethical approval for an internal audit study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent was not sought for the present study because it is an internal audit study.
Supplementary material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.