
Abstract
Background
Inequitable distribution of human resources in healthcare is one of the main obstacles to improve any health system. This study aimed to evaluate inequalities in the distribution of human resources in healthcare in South Khorasan Province, Iran.
Methods
We have investigated three types of health staff (i.e. nurses, general practitioners, and specialists) from 2013 to 2018. Data were collected from the annual reports of the Statistical Centre of Iran. The Gini coefficient and time trend regression were applied to measure the inequality.
Results
The distribution of specialists and general practitioners were the highest and lowest inequality, respectively. Inequalities in the distribution of nurses and specialists have decreased from 2013 to 2018, while the Gini coefficients of the general practitioners have increased from 0.31 to 0.38. According to the regression analysis, inequality in the distribution of nurses and specialists was decreasing over the time; however, the decline was only significant for specialists. While the coefficient B for general practitioners is positive, this indicates raised inequality, but the observed increase was not significant.
Conclusions
This study revealed that Iran, similar to several other low- and middle-income countries, is with faced the challenge of inequitable distribution of human resources in healthcare, which in turn indicates the necessity of reforms at national and regional levels to address inequalities in the distribution of healthcare human resources, particularly in South Khorasan Province. Hence, the main policy recommendation is to focus on continuous monitoring and evaluation of resource allocation in South Khorasan Province to reduce inequalities.
Introduction
Provision of healthcare services reflects a balance between several factors including ability to pay, availability, accessibility, acceptability, and compliance with needs. 1 Hence, we might claim that access to health services can be deemed as one of the main pillars of equity in any society. 2 To make the health system efficient, health staff is expected to be capable, motivated, and empowered. 3 In recent years, policymakers, managers, and health researchers have paid special attention to issues related to the distribution of human resources worldwide. 4 In the new era, the Sustainable Development Goals (SDG) have been launched seeking a universal health coverage (UHC) and access to appropriate, affordable, and high-quality health services.5,6 In the present time, many countries are on their way to achieve UHC; for that, these countries and several international developmental agencies have shown their commitment to fully support achieving UHC by 2030, this has been expressed especially in SDG 3.8. 6
In the endeavor toward UHC, many issues emerged which were related to the distribution of human resources. 7 In other words, one of the main pillars of health service provision is the equitable distribution of resources, particularly human resources.8,9 Some previous studies have investigated the accessibility and availability of healthcare services at national and international levels and concluded that there were substantial differences among regions, considerable inequalities in provision and/or access to healthcare services, prioritization of central provinces in resource allocation, and lack of appropriate access to health services.10–18
In Iran, several studies have examined the distribution of resources and reported serious inequalities.11,13–16,19–21 According to Article 29 in the Iranian Constitution, all society’s population should enjoy the right to social security and get benefits with respect to retirement, unemployment, old age, workers’ compensation, lack of guardianship, destitution, accidents, and demand to healthcare services (either for insured or uninsured). 22 All of these privileges should be governmentally provided using public income and society’s contributions. Therefore, it is a governmental responsibility to ensure equitable distribution of resources, which in turn facilitates achieving better and more equitable health among the community.
The importance of this issue arises from the fact that equitable distribution of and access to resources are crucial in accomplishing UHC goals. 23 For this reason, it is necessary to evaluate the access and distribution of health services as well as the human resources in order to develop and implement comprehensive programs aimed at addressing the identified problems. 16
On one hand, several studies24–26 emphasized the distribution of resources within the same province rather than between various provinces, and this was due to the negative impact of inequality on efficiency and public health indicators. On the other hand, some other studies highlighted the attractiveness of industrial areas and tourist destinations for healthcare professionals, as mentioned in Kazemi et al. 27 Hence, particular attention should be paid to the intra-provincial distribution of human resources in health care, especially in border provinces such as South Khorasan, mainly because of their limited population and paucity of resources, which in turn adversely affects their appeal to healthcare professionals. To the best of authors’ knowledge, no study has investigated the distribution of human resources in South Khorasan Province, Iran. Therefore, the current study aimed to evaluate inequalities in the distribution of human resources in healthcare in South Khorasan Province which is located in east Iran.
Methods
Using the concept of the Gini coefficient (GC), the current study aimed to measure the inequality associated with the distribution of human resources on healthcare in South Khorasan Province. This province, located to the east of Iran, was established in 2003 after the division of the Khorasan province into three provinces. South Khorasan is regarded as the third largest province according to its area, 151,193 K2; meanwhile, it is ranked 28th concerning the number of population, and its capital is Birjand city.
In this study, data were collected from the annual reports of the Statistical Centre of Iran (SCI) which issued in the period from 2013 to 2018. It is noteworthy that the distribution of human resources in healthcare has a major impact on the prevention of disease and improvement of the overall health of society.
28
Consequently, the distribution of three types of health staff were investigated, including nurses, general practitioners (GP), and specialists. Specialists embraced all specialty fields such as cardiology; infectious diseases; pediatrics; neurology; psychiatry; dermatology; general surgery; urology; orthopedics; neurology; ear, nose, and throat; optometry; gynecology; anesthesia; radiography; pathology; and laboratory. Several indicators have been developed to measure the inequality in the distribution such as the Theil Index, Herfindahl–Hirschman Index, Hoover Index-Robin Hood Index, and GC. The Theil Index is defined as the difference between distribution disorder index in the actual income and the income distribution disorder.
29
The Herfindahl–Hirschman Index is employed to measure the share and concentration of companies in the related industries, and it is defined as the sum of the second power of each company’s share of the total industry output, considering that the information of all companies are used and each company is equal in its share. This index has also been used to examine the concentration of various health-related parameters.30,31 The Hoover Index-Robin Hood Index represents a share of income that should be transferred from middle-income to upper-income people to achieve a perfectly equal income distribution.
32
The GC is widely used in studies performed in the field of health, particularly to measure income inequality.33,34 In this study, GC was applied to investigate the distribution of human resources in healthcare. The GC, as the relative contribution of population health, is also a measure of health inequality between individuals or social groups. For instance, inequality in the distribution of health or access to health services. The formula to calculate GC is as follows


The Gini index is in the range of 0 to 1, where 0 indicates the maximum equality, and 1 represents the maximum inequality. A GC of < 0.2 indicates maximum equality in the distribution. A coefficient between 0.2 and 0.3 denotes that equality in the distribution has been met to a large extent. A value between 0.3 and 0.4 indicates inequality in the distribution, values between 0.4 and 0.6 represent high inequality in the distribution, and finally, values higher than 0.6 indicate maximum inequality. 35 As aforementioned, the most widely used measure of inequality in distribution is GC. The Gini index or the coefficient of inequality, which is derived from the Lorenz curve, is the most widely applied index to measure equity in access to resources. The Lorenz curve also compares the distribution of a particular variable with the same distribution (of the same variable) that represents equality.
In the present study, the DASP 2.3 plugin was used to calculate the GC using STATA version 12. In addition, time trend regression was administered to investigate the trend of inequality from 2013 to 2018, according to the following equation

Results
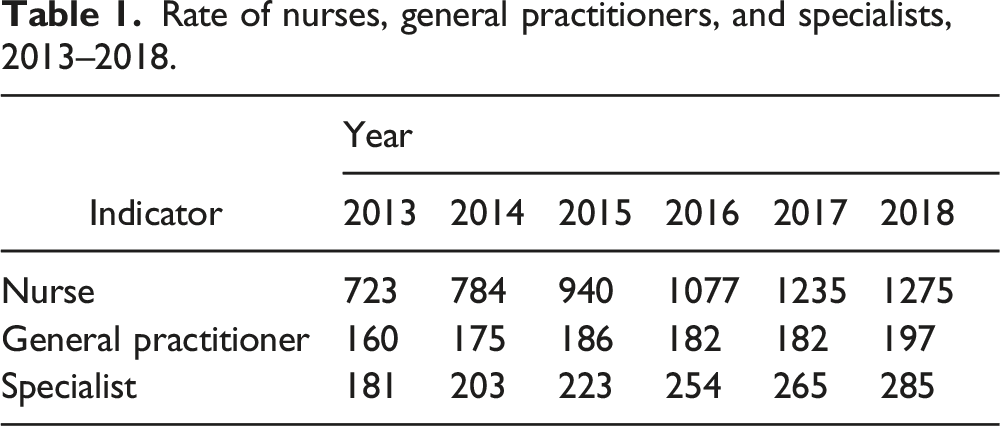
Rate of nurses, general practitioners, and specialists, 2013–2018.
Gini index of health human resources in South Khorasan Province, 2013–2018.

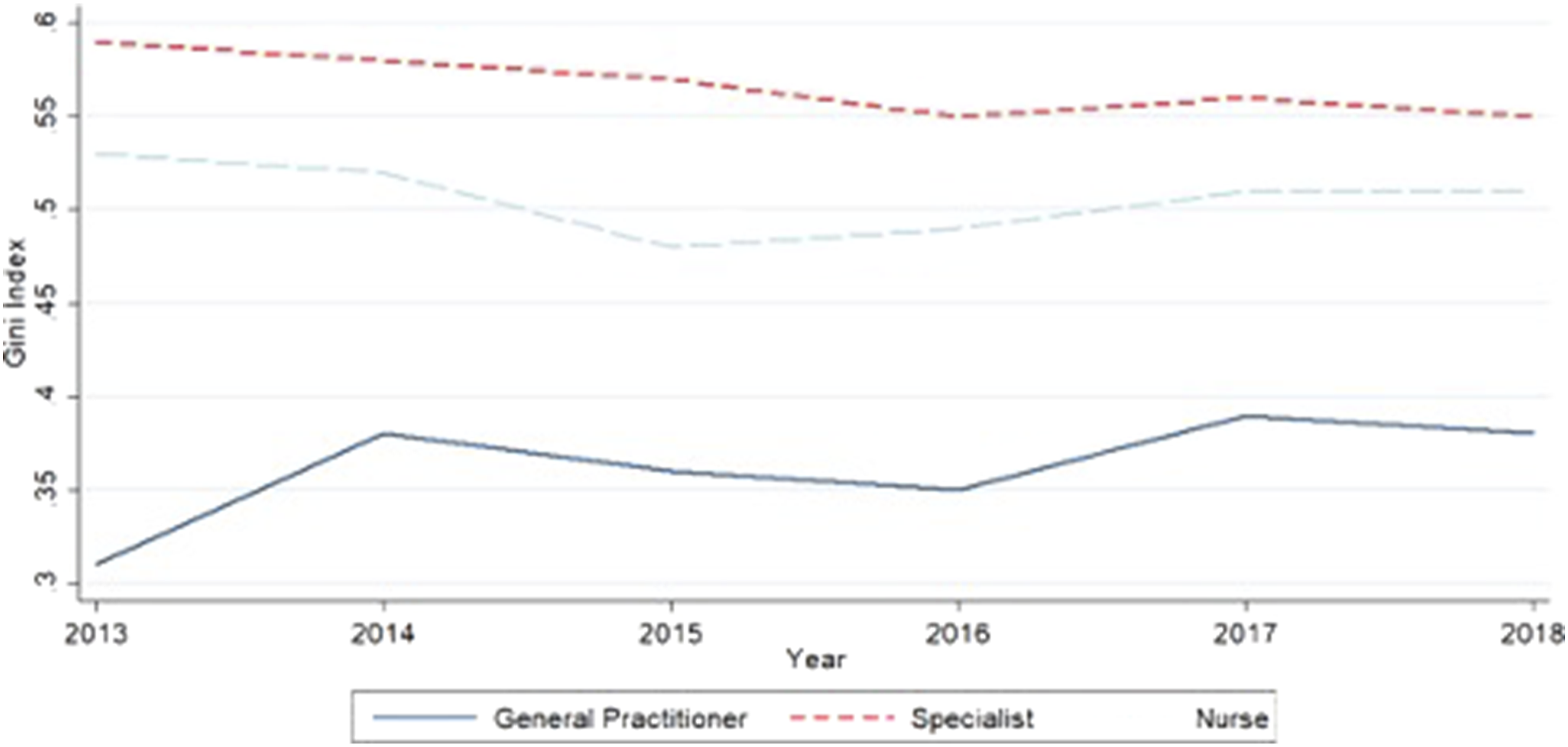
Time trend of Gini index of variables.
Time trend regression of inequality in distribution health human resources in South Khorasan Province, 2013–2018.

Discussion
Equitable distribution of human resources is not only emphasized by Article 29 of the constitution, but it is also of crucial importance for ensuring access to healthcare services and improving their quality and effectiveness. Therefore, the present study aimed to investigate the distribution of human resources (i.e., GPs and specialists and nurses) in South Khorasan Province for the period 2013–2018.
According to the findings, similar to other developing countries, Iran also encountered the challenge of inequitable distribution of human resources in healthcare. Nevertheless, this challenge is not limited to developing countries, so low- and middle-income countries like China and India, which have one of the largest and most diversified health labor markets, are faced with such problems despite major healthcare reforms and experiencing great progress. 36
The findings also revealed that the distribution of nurses was highly inequitable in all study years. Theoretically, the GC possibly ranges from 0 (maximum equality) to 1 (maximum inequality). A GC below 0.35 indicates equitable distribution; 0.35–0.5, relatively inequitable; and 0.5–0.7, complete inequitable distribution. 37 The findings of the present study are in line with some of the previous studies.38–40
We also found that the unequal distribution of nurses did not considerably change during the study period. This inequality can be partially attributed to the high-level policies of the Iranian healthcare system, such as the Tariffs of Nursing Services Act, which was enacted 14 years ago but still not implemented, despite the emphasis of the Supreme Leader. Because of this Act being disregarded, there are huge income inequalities between nurses and physicians, which has demotivated nurses and encouraged them to migrate to countries such as Canada, Australia, and Arab countries.41,42 As a result of these income inequalities, many nurses work in both public and private sectors to compensate their low incomes. It seems that due to the geographical location of South Khorasan Province and the small number of non-governmental hospitals (i.e., private and charitable) in this province, nurses do not possess many opportunities to work extra shifts. Therefore, most nurses are reluctant to work in this province and tend to do so in other provinces and major cities. The findings of the present study were consistent with the results of the Nishiura study. This study stated that many physicians and nurses are concentrated in the center of Bangkok. However, our findings were inconsistent with results reported in countries such as Mongolia. 43 According to the GC of GPs, the distribution of GPs has been relatively good during the study period. In contrast to nurses and specialists, GPs' distribution was less inequitable in South Khorasan Province, which is consistent with some previous studies.44,45 This relatively equitable trend can be due to the recently implemented macro policies such as increasing the capacities of medical schools and the local and targeted hiring policies.
The findings also showed that, despite some fluctuations, the inequality in the distribution of GPs has increased. The observed inequalities in the distribution of GPs can be referenced to the wide gap in annual incomes of GPs and specialists. Hence, GPs are inclined to work in populated cities. The findings of the present study are in line with the study conducted by Nishiura et al. 46 However, our findings are inconsistent with studies performed in Mongolia, Saudi Arabia, and Fiji.43,47,48 Considering that the distribution of GPs was more equitable than that of nurses and specialists, further studies are highly recommended to investigate the GC of physicians’ distribution between various cities in the province. Also, our findings were consistent with some other studies49,50 conducted in Iran. Nevertheless, a study 25 carried out in Iran showed that the distribution of GPs in Sistan and Baluchestan Province was better off than that of our estimate for South Khorasan Province.
Regarding the distribution of specialists, analyzing the GC trend during the study period revealed that the distribution of specialists has been completely inequitable. However, the findings of this study demonstrated that the inequality in the distribution of specialists has significantly decreased during the study period, and a remarkable progress has been achieved including addressing the gap in inequality. To some extent, the inequality in the distribution of specialists is due to the high-level policies of the health sector encompassing the training of health staff. Nevertheless, the health transformation plan has improved this trend by reducing inequalities. Since, in the present study, we did not separate specialists in accordance to their specialty (i.e., internal medicine, surgery, obstetrics, and pediatrics), investigating the inequality in the distribution of various specialties in the cities of South Khorasan Province is suggested. Our findings are consistent with the result of a study conducted in Khorasan Razavi Province. 50
The current study showed that although there are inequalities in the distribution of human resources in South Khorasan Province, programs designed to reduce inequalities in the distribution of specialists have been relatively successful in the recent years.
Therefore, when developing long-term plans, the Ministry of Health should consider the shortage of human resources, increased demand for specialists’ services, elderly, raised awareness of people, and deprivation of this province. Considering that the current ratio of medical professionals per 1000 population is 0.5 and according to the Islamic Republic of Iran’s 20-Year Vision Plan, 51 this ratio should increase to 0.9, and a major revision of the country’s education system should be made.
It is noteworthy that the programs which will be designed without taking into consideration the current human resource distribution will lack the intended effectiveness. Accordingly, interventions should be designed to maintain and promote the welfare of specialists in deprived regions. Due to the current international sanctions, the country is suffering from economic austerity measures; hence, the government needs to use the capacities of the private sector to increase access to services provided by medical specialists. Allocation of human resources based on the population is the simplest criterion, but one cannot ignore the influence of poverty on the burden of diseases and deprivation of South Khorasan Province. In the same vein, some studies reported a higher burden of diseases in deprived areas; nonetheless, less populated areas may need more health staff. 52
Since in the Iranian health system, policies on the distribution of human resources have a top-down approach, the findings of the present study represent strong evidence indicating the need for addressing the current inequalities. Due to the unsustainable financial resources of the health sector, international sanctions, and soaring costs, the need for controlling demand for healthcare services and emphasizing self-care and prevention cannot be neglected.15,20 According to the findings of the present study, despite expanding training capacities in recent decades, the problem of unequal distribution of human resources persists. Therefore, it can be argued that sole expansion of training capacities is not sufficient to improve the access to healthcare human resources or their distribution. Hence, immediate and more serious interventions are required.
The findings of this study can be used by managers and policymakers of the Iranian healthcare system to reduce inequality in the distribution of human resources in South Khorasan Province. This study demonstrated that human resources in healthcare are unequally distributed in South Khorasan Province. However, future studies are needed to investigate these inequalities within the province by using more precise indicators to provide more robust evidence for policymakers.
It is necessary to mention some limitations in our study. First, we have not investigated the distribution of all types of human resources within South Khorasan Province, which could make aspects of distribution and equity more clear. Second, the number of those professionals working in the private healthcare centers was not considered.
Conclusion
One of the major issues of health systems that currently concern policymakers is health inequalities. The equitable distribution of human resources in healthcare is an important issue that has always been considered in any health system. Also, the first step to achieving fair access to health services in all countries is the equitable distribution of human resources.
This study demonstrated the unequal distribution of human resources in healthcare, similar to other provinces of the country and other low- and middle-income countries. The results showed that inequality in the distribution of nurses and specialists has decreased, but this decline was only significant for specialists. In addition, the distribution of GPs has grown, but it was not significant. Hence, the main policy recommendation is to focus on the continuous monitoring and evaluation of resource allocation in South Khorasan Province to reduce inequalities.
Given the special geographical location of South Khorasan Province in the east of Iran and its low density of population, the equitable distribution of human resources is more challenging than other regions of the country, which indicates the need for particular programs. Thereby, in addition to continuous monitoring of resource distribution, other policy recommendations to reduce inequality in the province entail the use of intra-provincial localization methods to examine the in health-related fields related to motivation such as financial incentives and continuous education, using public–private participation model in order to use the capacities of other provinces (either public or private institutions), improving the distribution of physical resources like beds and medical equipment, and the use of per capita payment method to enhance retention of physicians in South Khorasan Province.
Footnotes
Acknowledgments
None.
Author Contributions
MD was responsible for the design, implementation, and drafting the article. SSM was involved in the conception, development, implementation, and writing the article. JE was responsible to conduct statistical analysis of the data. MHZ and ZM were responsible for the intellectual development of the article. All authors have read and approved the final article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of Data
Data are available and can be accessed by contacting with MD.
Ethical Approval
Not applicable.
Informed Consent
Not applicable.
Trial Registration
Not applicable.