
Abstract
This report documents a rare case of delayed-onset multiple acute dystonias after treatment with low dose intramuscular (IM) haloperidol lactate injection in a setting of non-neuroleptic drug overdose. The drug–drug interactions between haloperidol and high levels of paracetamol and naproxen are deliberated upon. A 25-year-old Asian female was admitted after an intentional overdose of medications (paracetamol, naproxen and pregabalin). She received 5 mg of IM haloperidol injection for agitation. 21 hours later she experienced mild intermittent ocular deviation in an upward and outward direction and generalised stiffness, which were self-resolving. An hour later, she required another 2.5 mg of IM haloperidol injection for further agitation. In the 35 hours following her first IM haloperidol (13 hours after the second IM haloperidol), she developed a total of three episodes of oculogyric crisis (OGC) with torticollis. Each episode was treated promptly with IM diphenhydramine 25 mg, and there was remission of symptoms within 15 minutes of treatment. An objective causality assessment revealed a definite relationship between the episodes of acute dystonia with IM haloperidol therapy. Where oral alternatives and IM atypical antipsychotics/benzodiazepines are unavailable, rapid tranquillisation with a high-potency typical antipsychotic is a possibility. However, consideration should be made to combine haloperidol with an anticholinergic agent as prophylaxis against acute dystonia, especially in the setting of drug overdose, even if it is that of a non-neuroleptic drug (in this case, paracetamol and naproxen).
Keywords
Introduction
Acute dystonias are involuntary sustained contractions of major muscle groups, producing painful muscular spasms, abnormal posturing and repetitive twisting movements. Symptoms of acute dystonia include torticollis, OGC and opisthotonos. These typically occur within 1 week of commencing or rapidly increasing the dose of the antipsychotic medication, or of reducing the anticholinergic medication prescribed to treat them. 50% of cases occur within 48 hours, rising to 90% within 5 days of exposure. 1
Haloperidol is a commonly used high-potency typical antipsychotic, effective in the management of acute behavioural disturbance 2 but poorly tolerated with a high risk of acute dystonia. These adverse effects are likely due to an increase in striatal cholinergic activity as a compensatory response to dopamine receptor blockade, which affects the dopaminergic–cholinergic balance. In an acute psychiatric setting, high‐dose parenteral sedation is defined as more than 10 mg of haloperidol 3 . Here, we report a case of delayed-onset multiple OGC and torticollis episodes after treatment with relatively low doses of IM haloperidol, occurring in the setting of non-neuroleptic drug overdose.
Case Report
A 25-year-old Asian female, referred here as patient X, was admitted after an overdose. She has a background of major depressive disorder, with no other significant medical illnesses. She is 158 cm, weighs 53.5 kg, with a BMI of 21.4 kg/m2. Past treatments include olanzapine 2.5 mg nocte and fluoxetine 20 mg omni mane for a 1-month duration before defaulting on treatment. She is not on any regular psychotropics for the past 6 months prior to admission.
She had overdosed on 20 tablets of paracetamol 500 mg (10,000 mg), 20 tablets of naproxen 275 mg (5,500 mg) and 14 capsules of pregabalin 25 mg (350 mg) with water. She denied any recent intake of tobacco, alcohol nor other illicit substances. Approximately 12 hours after her overdose, patient X reached the emergency department in a slightly drowsy state but her vital signs and physical examination were otherwise unremarkable. All investigations (renal panel, liver panel, full blood count, coagulation panel, paracetamol levels, salicylate levels and a toxicology screen) were also unremarkable except for raised paracetamol levels (59.0 mmol/L).
Patient X was oriented to time, place and person and did not display any features of overt psychosis. However, she refused the involuntary admission and attempted to abscond from the ward repeatedly, requiring restraints and 5 mg of IM haloperidol lactate injection for rapid tranquillisation. 21 hours later, she reported mild intermittent ocular deviation in an upward and outward direction with generalised stiffness throughout her entire body lasting for minutes. Symptoms were self-resolving and there were no torticollis nor other extrapyramidal side effects noted then. 22 hours after the first 5 mg IM haloperidol dose, she again attempted to abscond (mental state similar to earlier) and required a further 2.5 mg of IM haloperidol injection. 20 minutes after the second IM haloperidol injection, she developed her first episode of acute dystonic reaction with OGC and torticollis. Her eyes were fixed in a painful upward gaze and head was tilted to the back and side. Haloperidol was suspended and she was given IM diphenhydramine 25 mg. The symptoms resolved within 15 minutes of treatment.
She had a second (29 hours after the first IM haloperidol, 7 hours after the second IM haloperidol) and third episode (34 hours after the first IM haloperidol, 12 hours after the second IM haloperidol) of acute onset OGC and torticollis. Each episode was treated with IM diphenhydramine 25 mg with similar resolution observed. Additionally, a prophylactic dose of 2 mg oral benzhexol was given after the second episode. During each of these acute dystonic episodes, consciousness was maintained throughout, with no signs of seizures nor features of neuroleptic malignant syndrome.
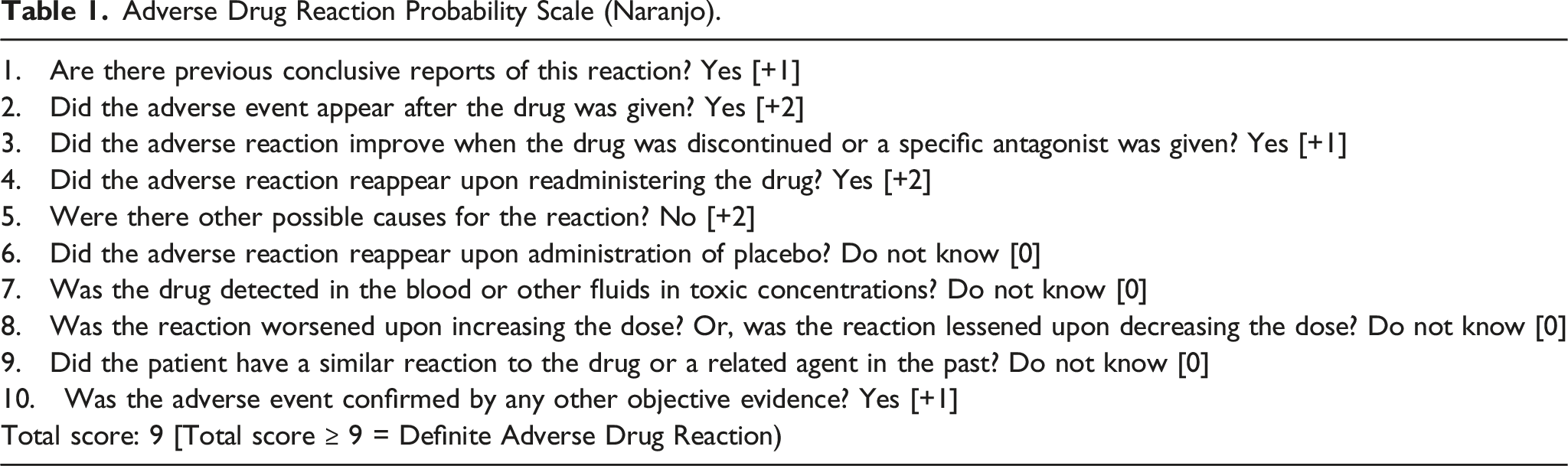
Adverse Drug Reaction Probability Scale (Naranjo).
Discussion
Early recognition and prompt treatment of acute dystonias are essential. Risk factors for acute dystonia include IM administration (in the case for haloperidol), young age (<45 years old), male sex, liver failure, hypocalcaemia, recent cocaine misuse and a personal/family history of acute dystonic reactions 5 . The risk of acute dystonia also correlates with drug dosage, potency and the rate of titration. Patient X has but a few of the above risk factors, and received only a total of 7.5 mg of IM haloperidol, with a significant interval (22 hours) between the first and second dose administration. This led the authors to review the relationship between the concomitant non-neuroleptic drug overdose and the development of multiple acute dystonias.
Acute dystonia is usually rapid in onset and is related to the pharmacokinetic profile of IM haloperidol. For agitation, the initial effects of haloperidol occur within 15 minutes with a mean time to sedation of 24.8 minutes. 6 Haloperidol is extensively metabolised in the liver, and IM administeration which avoids the first-pass metabolism by the liver results in increased bioavailability compared to the oral administration. Therefore, oral haloperidol peaks in 1.7–6.1 hours while IM haloperidol peaks within 20 minutes, with a half-life of approximately 14.1–26.2 hours. 7
At therapeutic doses, there are no clear drug–drug interactions between haloperidol and, paracetamol, naproxen and pregabalin individually, however, dynamics between the drugs may differ in the setting of drug overdose. The pharmacokinetics of haloperidol might be influenced by high doses of these co-administered drugs, specifically haloperidol’s metabolic clearance and binding to plasma proteins (haloperidol is highly protein-bound at 88–93%). Haloperidol appears to be a moderately hepatically extracted drug. 7 Although hepatic cytochrome P450 (CYP) 3A4 enzyme appears to be the major isoform responsible for the metabolism of haloperidol in humans, 7 it is also a major substrate of 2D6, and minor substrate of 1A2 enzymes. 8
At therapeutic doses, 90% of paracetamol is metabolized in the liver to sulfate and glucuronide conjugates via sulfotransferase and UDP-glucuronosyl transferases. 9 The remaining paracetamol is metabolized via oxidation by the hepatic CYP2E1 enzyme. Other than 2E1, paracetamol is also a minor substrate of CYP2A6, 2C9 and more importantly, 3A4, 2D6 and 1A2 enzymes, which haloperidol is also a substrate of Ref. 8. With an overdose of paracetamol, the sulfation and glucuronidation pathways become saturated, and more paracetamol is shunted to the CYP450 enzymes. The toxic level of paracetamol then competes with haloperidol for binding to CYP3A4, 2D6 and 1A2 enzymes, hence reducing metabolic clearance of haloperidol. This increases drug exposure and hence the risk of ADR. In addition, paracetamol has a plasma protein binding of 10–25%, but at toxic doses, this increases to 8–43% 10 . Similarly, competitive binding to plasma protein may result in more free and unbound haloperidol, increasing ADR risk, especially since haloperidol is highly protein-bound.
Naproxen is a nonsteroidal anti-inflammatory drug that is extensively metabolized in the liver, and a minor substrate of CYP1A2 and 2C9 enzymes. Rarely, it can cause liver toxicity. 10 Naproxen is also highly bound to plasma protein (>99% at therapeutic doses) and may thus displace and transiently increase haloperidol exposure.11,12
Pregabalin is a potent ligand for the alpha-2-delta subunit of voltage-gated calcium channels in the central nervous system, and works as an anticonvulsant, analgesic and anxiolytic agent. 13 It is 0% protein-bound, not subjected to hepatic metabolism, and does not induce nor inhibit liver enzymes such as those in the CYP450 system. 10 It is thus unlikely to have a major role in drug interaction with haloperidol.
Therefore, the development of multiple acute dystonias at a relatively low dose of IM haloperidol could be explained by the IM administration itself, with contributions from a concomitant overdose of paracetamol and naproxen, via reduced CYP450 enzyme metabolism and altered protein-binding. Clinical implication includes consideration of combining IM haloperidol with an agent with anticholinergic properties (e.g. diphenhydramine, promethazine) for prophylactic treatment in similar future settings.
Of note, patient X experienced no extrapyramidal symptoms for the 21 hours after her first IM haloperidol dose, and only developed OGC and torticollis 20 minutes after the second smaller dose. This atypical delayed onset was similarly noted by Jhee et al. 14 whose patient received a total of 17.5 mg of IM haloperidol over two doses (7.5 mg and 10 mg), and developed OGC and torticollis only 26 hours after the first injection. However, the difference lies in the much reduced total dose of 7.5 mg of IM haloperidol administered to patient X, and the presence of multiple episodes of acute dystonia despite cessation of the offending agent.
Conclusions
This case report highlights an unexpected and delayed-onset adverse effect of haloperidol lactate. This adverse effect can occur at a low dose of IM haloperidol, and acute dystonia can present multiple times after, despite cessation of the offending agent. While the concomitant non-neuroleptic drugs typically do not have any clinically significant drug–drug interactions giving rise to dystonias, in an overdose setting, their relationship with haloperidol should be re-examined. Where oral alternatives and IM atypical antipsychotics/benzodiazepines are unavailable, rapid tranquillisation with a high-potency typical antipsychotic is a possibility. However, consideration should be made to combine IM haloperidol with an anticholinergic agent as prophylaxis against acute dystonia, especially in the setting of drug overdose, even if it is that of a non-neuroleptic drug (in this case, paracetamol and naproxen).
Footnotes
Acknowledgments
We would like to thank Dr Liew Tau Ming (Consultant Psychiatrist) for reviewing the draft copy of the manuscript.
Author contributions
Dr Cai Hao, Howard Khoe obtained consent and wrote the first draft of the manuscript. Both authors reviewed and edited the manuscript, and approved the final version.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Singapore General Hospital does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.
Data avaliabilty
Data sharing is not applicable to this article as no datasets were generated or analysed during the current study.