
Abstract
Unilateral sinonasal mass presenting as nasal block is a common presentation but poses a diagnostic challenge. The differential diagnosis includes inflammatory polyps, benign and malignant sinonasal neoplasm. Fibrolipoma presenting in the sinonasal area is an uncommon pathology. As it is uncommon, there is potential for a misdiagnosis, unnecessary investigation and delay in the definitive treatment. We report a patient with a fibrolipoma originating from the posterior nasal septum. The diagnostic and surgical features of this unique case are discussed.
Introduction
Lipomas are benign mesenchymal neoplasms consisting of mature adipocytes, generally enclosed by a thin fibrous capsule, and are classified as classic lipoma, fibrolipoma, angiolipoma, lipomatosis of nerve and lipoblastoma. 1 Histological variant is very rare as compared to classic lipoma. Fibrolipoma is an extremely rare subtype which accounts for 1.6% of all head and neck lipomas. 2 Most common sites of occurrence for head and neck fibrolipomas are the posterior subcutaneous neck, while a few cases have been reported in the oral cavity.3,4 To date, only two cases have been reported on fibrolipoma of the nasal septum (Table 1).5,6 Both of these were found at the anterior septum. We report the case of a patient who had a fibrolipoma of the posterior nasal septum.
Clinical features, imaging findings and treatment of reported cases of nasal septal fibrolipoma.

CT: computed tomography scan; MRI: magnetic resonance imaging.
Case report
A 42-year-old man presented with a unilateral right nasal block for 7 years. He claimed the nasal block was initially intermittent, but later became persistent. No history of frequent rhinorrhea, nasal itchiness, facial pain and epistaxis was noted. He had no family history of malignancy. A rigid nasoendoscopy revealed a solid reddish multilobulated mass at the right posterior choana which occupied the whole nasopharynx (Figure 1). The mass was non-pulsatile and not friable without any secretion or mucopus in the nasal cavity. The site of origin of the mass was not visualised due to the size of the mass which occupied the whole posterior choana. Intraoral examination showed a lobulated mass at the right side of the oropharynx which was an extension from the nasopharyngeal mass. Biopsy was taken from the nasal mass and the histopathological analysis demonstrated an inflammatory polyp. An intravenous contrast enhanced computed tomography (CT) scan of the paranasal sinuses demonstrated a lobulated peripheral enhancing attenuated mass measuring approximately 5.3 cm × 3.6 cm × 4.8 cm at the posterior choana (Figure 2).

Nasal endoscopic view. (a) The right posterior choana mass (black asterisk, *) attached at the upper part of the posterior septum (black arrow). (b) The whole nasopharynx is occupied by the mass. (c) Intraoral examination depicting the extension of the mass into the oropharynx from the nasopharyx.
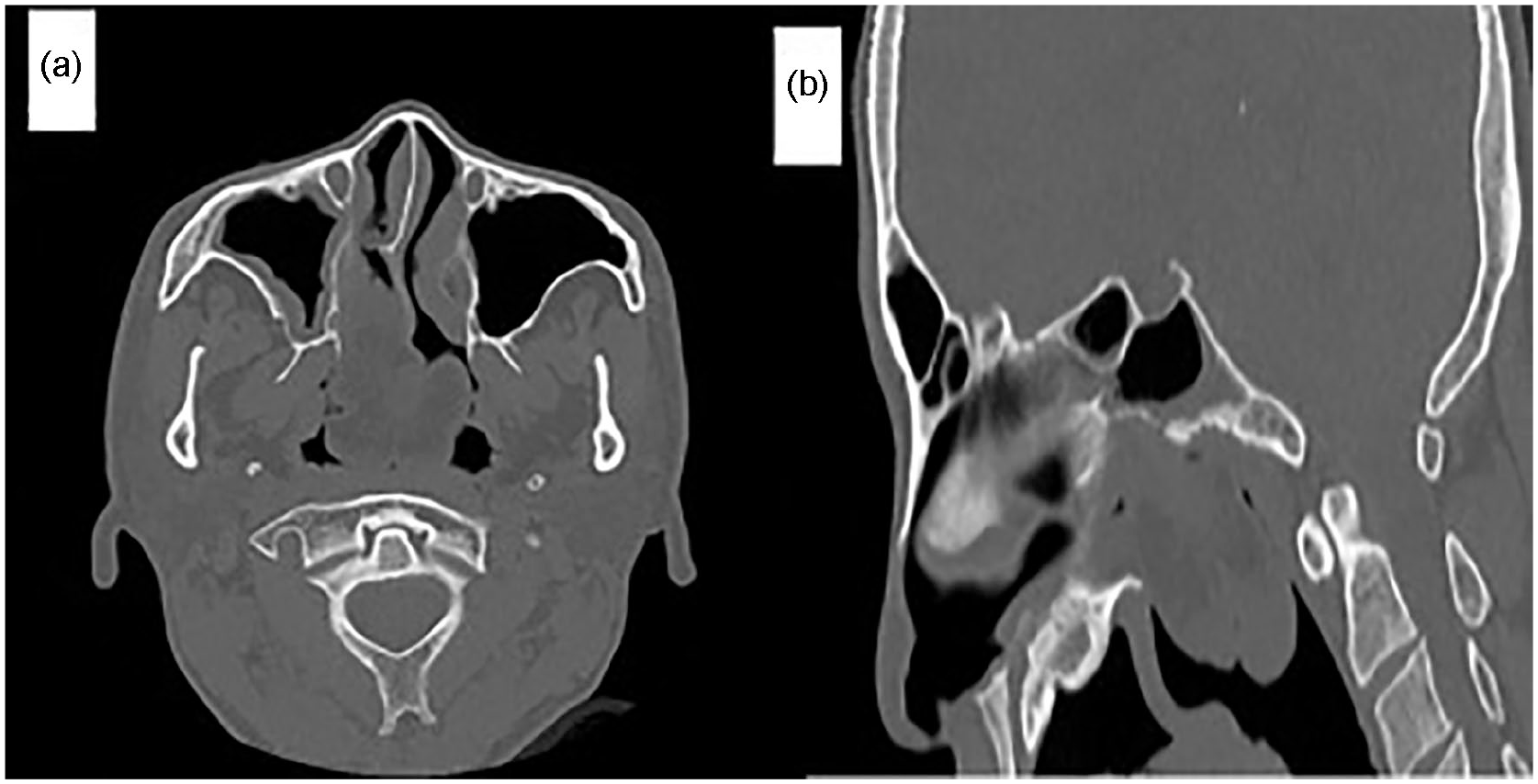
Computer tomography of paranasal sinuses. (a) and (b) Axial and sagittal section, demonstrating lobulated mass at the right posterior choana, occupying the whole nasopharynx with inferior extension to the superior aspect of the oropharynx. (b) The sagittal section demonstrating a fat attenuating mass at the right posterior choana, just inferior to the floor of the sphenoid sinus.
Anteriorly it extended into the nasal cavity with displacement of the middle turbinate superiorly and inferior turbinate laterally. Posteriorly it occupied the nasopharynx with inferior extension to the superior aspect of the oropharynx. Superiorly the mass caused scalloping, irregularities, erosion and sclerosis of the sphenoid sinus floor. However, there was no obvious extension into the sphenoid sinus. Medially, the mass caused thinning and bowing of the vomer bone on the left nasal cavity. Based on the histopathological analysis and imaging, a sphenochoanal polyp was initially suspected. An endoscopic surgical excision was performed under general anesthesia. Endoscopic examination showed the mass was attached to the posterior part of the right nasal septum by a thin stalk, indicating that this was the site of origin. The right sphenoid sinus was otherwise clear. The mass appeared very fibrotic which required the use of several instruments such as a microdebrider, sickle knife and microscissor. The thin stalk was carefully identified and excised using a microscissor. Grossly, the mass was well circumscribed, multilobulated, whitish, smooth-surfaced and firm measuring 45 mm × 35 mm × 28 mm. Microscopically the tumor was well circumscribed, covered by respiratory-type epithelium with areas of squamous metaplasia. The subepithelial stroma was moderately infiltrated by lymphoplasmacytic cells and the stroma was composed of mature adipocytes separated by incomplete fibrocollagenous septa (Figure 3). There were scattered benign seromucinous glands in the septa and no evidence of malignancy seen. The adipocytes were positive for S100 while negative for HMB-45 and smooth muscle actin (SMA) stains which weres in favor of fibrolipoma. Postoperative follow- up of the patient after 3 months showed no signs of recurrence and the patient remained asymptomatic.

Hematoxylin and eosin (H&E) stained sections depicting the microscopic features of the case presented. (a) Low power image showing the stroma of the lesion composed of groups of mature adipocytes separated by thick fibrous septa (H&E, ×4 magnification). (b) The septa composed of fibro-collagenous tissue (H&E, ×40 magnification). (c) Mature adipocytes that formed the lesion (H&E, ×40 magnification).
Discussion
Lipoma is a well-encapsulated mass of mature adipocytes benign tumor of fat, which usually arises in the subcutis of proximal extremities and trunk, most frequently during middle adulthood. These tumors are subclassified according to morphologial and/or characteristic molecular features as conventional lipoma, fibrolipoma, angiolipoma, spindle cell lipoma and myelolipoma. 7 Fibrolipoma is a rare microscopic variant of lipoma, characterized by mature adipose tissue interspersed by dense fibrous connective tissue. Congenital disorder, endocrine imbalances, degeneration of fibromatous tumor, or from the maturation of lipoblastomatosis are thought to be the etiological factors. The growth rate of fibrolipomas is faster than the classic variants. 8 The occurrence of fibrolipomas in the nasal cavity and paranasal sinus is rare and probably reflects the paucity of normal adipose tissue in this area. To our knowledge, there have been only two cases in the literature reported on fibrolipoma arising from the nasal septum.5,6 Nonetheless, these tumors were found at the anterior nasal septum as compared to our case which was at the posterior nasal septum. Pleomorphic adenoma commonly arises from the posterior nasal septum and is one of the most common differential diagnoses considered for a mass found at this area. 9 Fibrolipoma is the other differential diagnosis that should be considered for a posterior nasal septal mass, especially when the histopathological analysis is inconclusive.
Patients with unilateral nasal mass present with varied nasal symptoms such as nasal obstruction, nasal discharge, epistaxis, hyposmia and headache. The extranasal symptoms are commonly facial pain, dental and orbital symptoms. 10 In our case, the patient mainly presented with chronic unilateral nasal blockage without typical symptoms of chronic rhinosinusitis, which indicates a neoplastic pathology and precludes an inflammatory condition. The differential diagnosis for benign tumor at the sinonasal area generally includes inverted papilloma, pleomorphic adenoma, osteoma, angiofibroma, glioma, dermoid cyst, schwannoma, leiomyoma, paraganglioma and solitary neurofibroma. Ozturk et al. who reported the first case of nasal septum fibrolipoma, described the presence of accompanying intracranial lipoma in nasal septum fibrolipoma. 6 Hence, a preoperative radiological assessment to identify the primary and accompanying lesion is a useful investigation.
Magnetic resonance imaging (MRI) is the modality of choice for the evaluation of lipomatous tumor. It is not only used to confirm the diagnosis, but also for a better assessment of atypical features suggesting liposarcoma and the surrounding anatomy. In classic lipomas, they have generally been described as homogenous intensity identical to subcutaneous fat in all MRI pulse sequences, with complete loss of signal after fat suppression and no enhancement with contrast. However, MRI features for fibrolipoma may mimic well-differentiated liposarcoma in which areas of non-adipose (fibrous) show a mild inhomogeneous enhancement with gadolinium. 11 Meanwhile, in CT images, it is important to identify the presence of bony erosion which may indicate more sinister pathologies such as liposarcoma. Immunohistochemistry may distinguish fibrolipoma from liposarcoma as it is negative for murine double minute-2 (MDM2), cyclin-dependent kinase-4 (CDK4) and p16. 11
Malignant transformations in the oral and maxillofacial regions are rare. 12 The recommended treatment for fibrolipoma is surgical excision with capsular dissection which is associated with rare recurrence.6,12 In nasal septal fibrolipoma, there is an involvement of the submucosal tissue of the nasal septum where it adheres, and this area should be resected together with the whole mass. In our patient, tumour excision was performed at its attachment around the posterior nasal septum to ensure complete removal.
Conclusion
Even though fibrolipoma arising from the nasal septum is uncommon, such a pathology must be considered to avoid misdiagnosis, unnecessary investigation, and delay in the definitive treatment.
Footnotes
Acknowledgements
None.
Authors’ contributions
All author(s) performed a literature review, provided the attached images, conceived the case report, reviewed, and edited the manuscript.
Availability of data and materials
Data and materials are available from the corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Universiti Sains Malaysia does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for his anonymized data to be published in this article.