
Abstract
Background
Paediatric neuro-interventional (PNI) procedures are markedly different to adult procedures and are more likely to be complicated by vasospasm. Traversing the complex tortuous anatomy in these fragile vessels requires both torque control and distal tip softness of the microwire. The Aristotle wires (Scientia Vascular Inc) are a new family of wires with design features offering both torque control and distal tip softness. We sought to assess the ability of these wires to achieve successful target vessel cannulation in paediatric patients.
Methods
The study design was a single-centre case-control study. We compared a case cohort of PNI procedures performed using the Aristotle wires (2023–24) with a control cohort using other wires (2022–23). The primary study outcome was successful cannulation of the target vessel (Yes/No) with a microcatheter.
Results
The Aristotle wires cohort consisted of 44 targeted vessels across 40 procedures in 20 patients (F = 8; mean age 6.9, SD 6.53 years). The other wires cohort consisted of 41 targeted vessels across 41 procedures in 19 patients (F = 6; mean age 4.3, SD 4.98 years). Successful cannulation of the target vessel was achieved in 43 of 44 target vessels (97.7%) in the Aristotle wires cohort and 34 of 41 target vessels (82.9%) in the other wires cohort (p = .020). The rate of wire-related complications was significantly lower in the Aristotle wires cohort (0 of 44 vs 6 of 41 target vessels, p = .008).
Conclusion
Aristotle wires were associated with significantly better target vessel cannulation and lower wire-related complications than other wires in PNI procedures.
Introduction
Paediatric neuro-interventional (PNI) procedures are markedly different to adult procedures. 1 Differing factors include patient size, vessel size, 2 and tortuosity, underlying pathology,1,3 and the propensity towards vasospasm,4–6 thrombosis, 7 and dissection. 8 Such factors can limit accessibility to the target vessel for treatment. Super-selective manipulation of microcatheters within the intracranial circulation of children may trigger iatrogenic vasospasm, 6 further limiting the ability to reach the target vessel.
Paediatric-specific devices
A major challenge in undertaking PNI procedures is the relative absence of paediatric-specific devices on the market. 3 For this reason, PNI practitioners frequently adapt the use of devices designed for adults into the paediatric setting.1,3,9 Such adaptation requires careful selection based on the physical properties of the device, access sheath and guide catheter diameter, size, and tortuosity of the target vessel, and the pathology being treated. Virtually all such adaptation results in ‘off-label’ use of the stated device due to the relative absence of device-specific clinical studies in children.
Microwires in PNI procedures
PNI procedures include vein of Galen Malformation (VoGM) embolization, arterio-venous malformation (AVM) embolization, and intra-arterial chemotherapy (IAC) for retinoblastoma, all of which require successful microcatheterization of small arteries in infants and young children.
3
The choice of microwire is dependent on the distal inner diameter of the desired microcatheter and the tortuosity of the planned navigation path. Successfully catheterizing the target vessel in PNI procedures typically requires a balance of both enhanced torque control and minimal vessel wall trauma in a frequently tortuous and fragile arterial circulation (see Figure 1). Digital subtraction angiography images of three patients demonstrating the tortuous arterial anatomy and fragile vasculature frequently encountered in paediatric neuro-interventional practise. Aristotle wires were successfully utilized in these patients during their course of treatment to traverse this complex anatomy. A – Lateral right ICA projection in a neonate with vein of Galen malformation, via a 4Fr catheter in the proximal right cervical ICA. Note the tortuous cervical ICA tonsillar loop and posterior choroidal artery that must be traversed to approach the AV junction. B – Lateral left ICA projection in a neonate with a para-cerebellar AV malformation draining into a dural sinus malformation, via a 4Fr catheter in left CCA. Note the extensive tortuosity of the cervical ICA and the left PCA that must be traversed. C – Lateral left ICA projection in a child with connective tissue disease and a giant petro-cavernous aneurysm prior to placement of a flow-diverter construct. Note the complex course that the 0.027in microcatheter must traverse to reach the supraclinoid ICA. ABBREVIATIONS: AV – arterio-venous, CCA – common carotid artery, in - inches, Fr - French, ICA – internal carotid artery, PCA – posterior cerebral artery.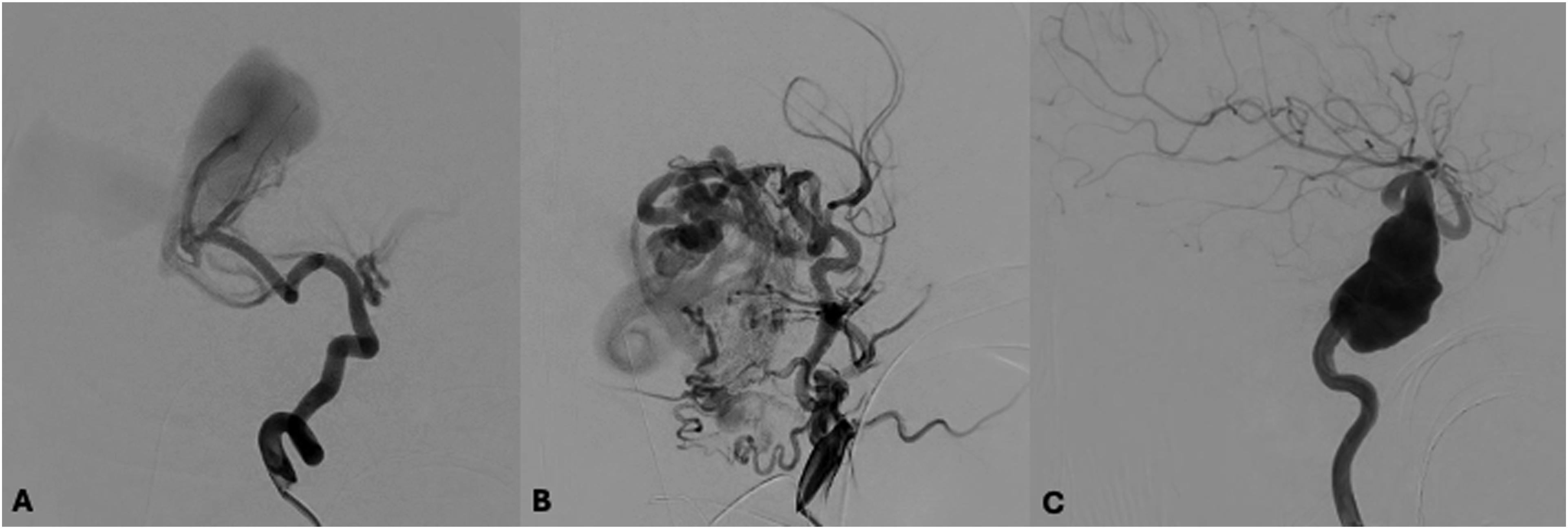
The Aristotle guidewires (Aristotle-14, -18, and -24; Soft and Standard; Scientia Vascular Inc, Utah, USA) are a new family of guidewires with design characteristics that would theoretically enhance torque control and distal tip softness. Our primary objective was to assess the rate of successful target vessel cannulation in PNI procedures using Aristotle wires via a case-control study.
Methods
Ethics approval was granted by our institutional human research ethics committee.
Study design, setting, and cohort characteristics
The study design was a single-centre case-control study utilizing retrospective analysis of a prospectively maintained procedural and complication database. Our centre is a quaternary paediatric referral centre with an established PNI service including endovascular treatment of VoGM, non-Galenic AVMs, and IAC for retinoblastoma. The procedures were undertaken by three interventionists, often in combination. Eligible patients were of age <19 years at the time of their first included procedure and of age <16 years at the time of first clinical contact with our centre, consistent with the admission criteria to our paediatric hospital. Patient age was reported at the time of each procedure.
The case cohort consisted of all supra-aortic endovascular PNI procedures undertaken utilizing Aristotle wires (Aristotle-14, -18, and -24; Soft or Standard) beginning at first uptake of the wires in our centre and over a subsequent 12-month period, extending from August 2023 to July 2024. The control cohort consisted of consecutive supra-aortic endovascular PNI procedures only utilizing other (non-Aristotle) wires between November 2022 and November 2023. The latter was the timepoint after which Aristotle wires became the most used primary wire for PNI procedures in our centre. Diagnostic cerebral angiography procedures were only included if they utilized wires smaller than 0.035in diameter for super-selective angiography.
The overlapping period across these two cohorts (August–November 2023) included some cases in which other wires were primarily used and then were switched to Aristotle wires during the same procedure (included in the Aristotle case cohort). Consistent with international PNI practise, paediatric patients frequently underwent multiple procedures for treatment of the same condition (e.g. IAC for retinoblastoma) including a subset of patients that underwent procedures in both cohorts.
Primary and secondary outcomes
The primary study outcome was successful cannulation of the target vessel (Yes/No) with a catheter or microcatheter when utilizing Aristotle wires vs other wires for guidance.
Secondary outcomes included
i) Prior failure to cannulate the target vessel with another wire during the same procedure, ii) Occurrence of intra-procedural iatrogenic vasospasm requiring the use of intra-arterial spasmolytics, iii) Other wire-related complications (include wire-related vessel perforation), iv) All wire-related complications (including vasospasm and other wire-related), and v) Non-wire-related intra-procedural complications.
Statistical analysis
All primary and secondary outcomes were dichotomous in nature and were compared between the case and control cohorts using the χ2 test (α = 0.05). Demographic continuous variables such as age were compared between cohorts using the t test. Sensitivity analysis of potential confounder variables was undertaken using multivariable logistic regression. All statistical analyses were completed using MiniTab statistical software (Version 22.1.0).
Results
Comparison of Aristotle versus other wires: Demographics, procedures, and outcomes.
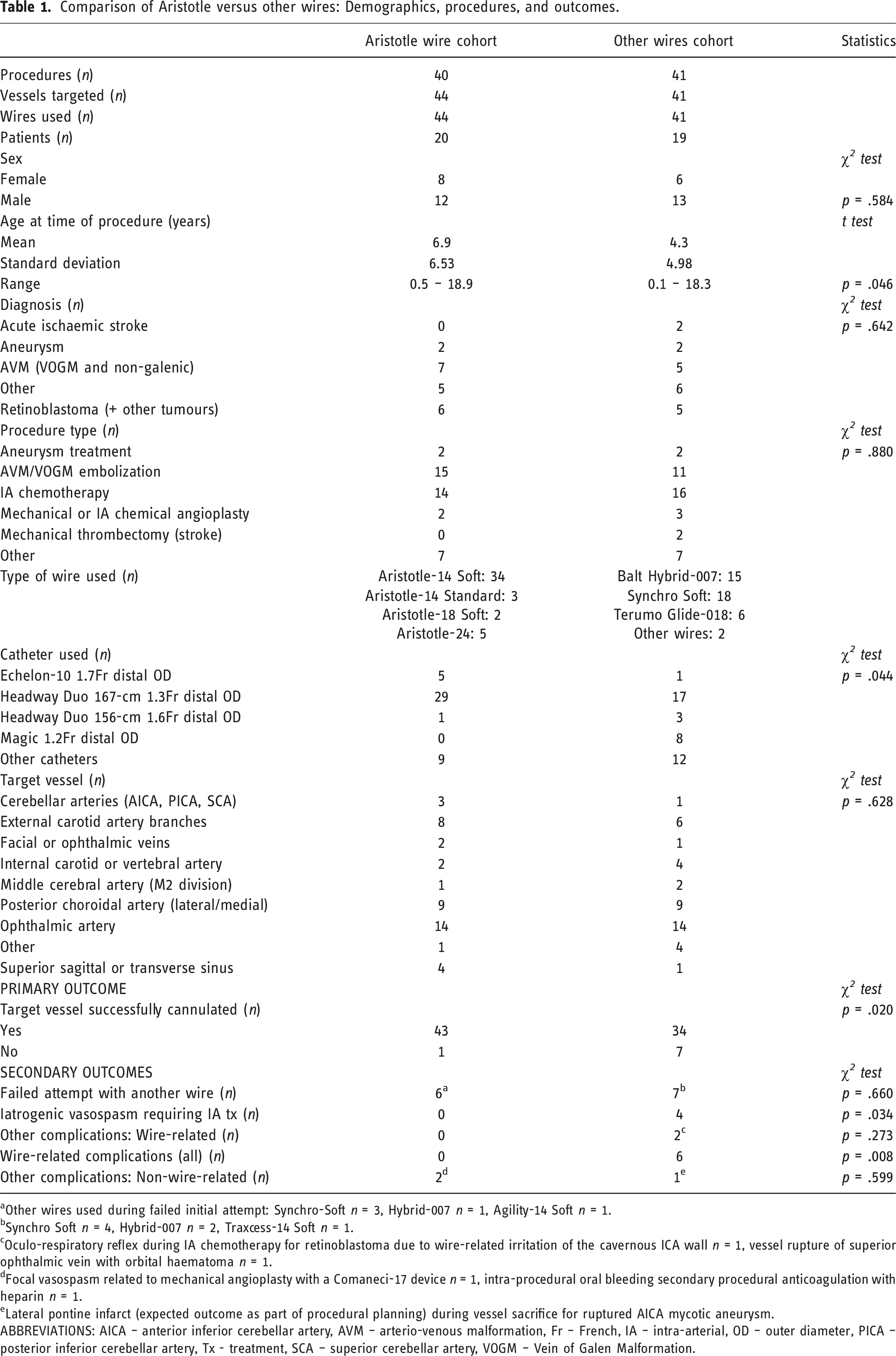
aOther wires used during failed initial attempt: Synchro-Soft n = 3, Hybrid-007 n = 1, Agility-14 Soft n = 1.
bSynchro Soft n = 4, Hybrid-007 n = 2, Traxcess-14 Soft n = 1.
cOculo-respiratory reflex during IA chemotherapy for retinoblastoma due to wire-related irritation of the cavernous ICA wall n = 1, vessel rupture of superior ophthalmic vein with orbital haematoma n = 1.
dFocal vasospasm related to mechanical angioplasty with a Comaneci-17 device n = 1, intra-procedural oral bleeding secondary procedural anticoagulation with heparin n = 1.
eLateral pontine infarct (expected outcome as part of procedural planning) during vessel sacrifice for ruptured AICA mycotic aneurysm.
ABBREVIATIONS: AICA – anterior inferior cerebellar artery, AVM – arterio-venous malformation, Fr – French, IA – intra-arterial, OD – outer diameter, PICA – posterior inferior cerebellar artery, Tx - treatment, SCA – superior cerebellar artery, VOGM – Vein of Galen Malformation.
Cohort characteristics
The Aristotle wires cohort consisted of 44 targeted vessels across 40 procedures in 20 patients (female n = 8; mean age 6.9, SD 6.53 years). The other wires cohort consisted of 41 targeted vessels across 41 procedures in 19 patients (female n = 6; mean age 4.3, SD 4.98 years). There was no significant difference in the sex distribution between cohorts (p = .584) but the control cohort was significantly younger (p = .046) due to the inclusion of multiple embolization procedures within 1 week in the same neonate in this cohort. The most common procedures undertaken were IAC for retinoblastoma (case cohort n = 14, control cohort n = 16) and AVM/VoGM embolization (case cohort n = 15, control cohort n = 11).
Primary outcomes
The primary outcome of successful cannulation of the target vessel was achieved in 43 of 44 target vessels (97.7%) in the Aristotle wires cohort and 34 of 41 target vessels (82.9%) in the other wires cohort. The rate of successful cannulation of the target vessel was significantly higher in the Aristotle wires cohort (p = .020).
Secondary outcomes
Prior failed attempts at cannulation of the target vessel during the same procedure using a different wire occurred in 6 of 44 target vessels (13.6%) in the Aristotle wire cohort and 7 of 41 target vessels (17.1%) in the other wires cohort (p = .660). The were no instances of iatrogenic vasospasm requiring intra-arterial spasmolytics in the Aristotle wire cohort compared with four instances in the other wires cohort (p = .034). The rate of all wire-related complications was also significantly lower in the Aristotle wires cohort (0 of 44 target vessels vs 6 of 41 target vessels, p = .008). Two patients with wire-related complications in the other wires cohort, both undergoing embolization for VoGM, required abandonment and rebooking of their procedures due to iatrogenic vasospasm (n = 1) and periorbital haematoma from superior ophthalmic vein rupture (n = 1). There were no deaths or wire-related long-term neurological sequelae in either group.
Sensitivity analysis for potential confounders
Due to the significant difference in age between groups (p = .046) and the heterogeneity of wire types utilized in the other wires cohort, age, and wire type were identified as potential confounders for inclusion in the sensitivity analysis. Multivariable logistic regression was performed with the dependent variable of successful cannulation of the target vessel (Yes/No) and predictors of age and wire type. This analysis demonstrated that age was not a significant predictor of successful cannulation (p = .433; OR 1.09, 95%CI 0.88–1.35; b = 0.09). Use of an Aristotle wire was a significant predictor of successful cannulation (p = .042; OR 10.84, 95%CI 1.09–107.6; b = 2.38), however, none of the other wires used were significant predictors of successful cannulation (p = .405–1).
Discussion
Aristotle wires were associated with a significantly higher rate of successful target vessel cannulation compared with other wires in our study of PNI procedures. The Aristotle wires cohort also had significantly lower rates of intra-procedural vasospasm and all wire-related complications. These results suggest that Aristotle wires provide advantages over other wires in paediatric patients that may stem from design characteristics such as torque control, trackability, and distal tip softness.
Aristotle guidewire design
The Aristotle guidewires (Aristotle-14, -18, and -24; Soft and Standard; Scientia Vascular Inc, Utah, USA) are a new family of guidewires consisting of a core wire that flattens distally, a surrounding coil wire for transmission of torque to the core wire, and a microfabricated nitinol tube externally with a hydrophilic coating (see Figure 2). The nitinol tube is the main provider of torque control, as opposed to many other wires in which torque is primarily transmitted via the core wire, consisting of numerous transitions between cut patterns from proximal to distal. The more proximal cut patterns are designed for torque transfer whilst the most distal cut patterns, where the number of cuts and transition points greatly increase in number, are designed for softness (see Figure 2). Thus, the design potentially allows for an improved balance between torque control and distal softness which may be of benefit in PNI procedures. Schematic diagram demonstrating the structure and design features of the Aristotle wires (Reproduced with permission from Scientia Vascular Inc). Note the progressive transition in the cut pattern of the exterior nitinol tube allowing for a greater balance of torque control with distal tip softness.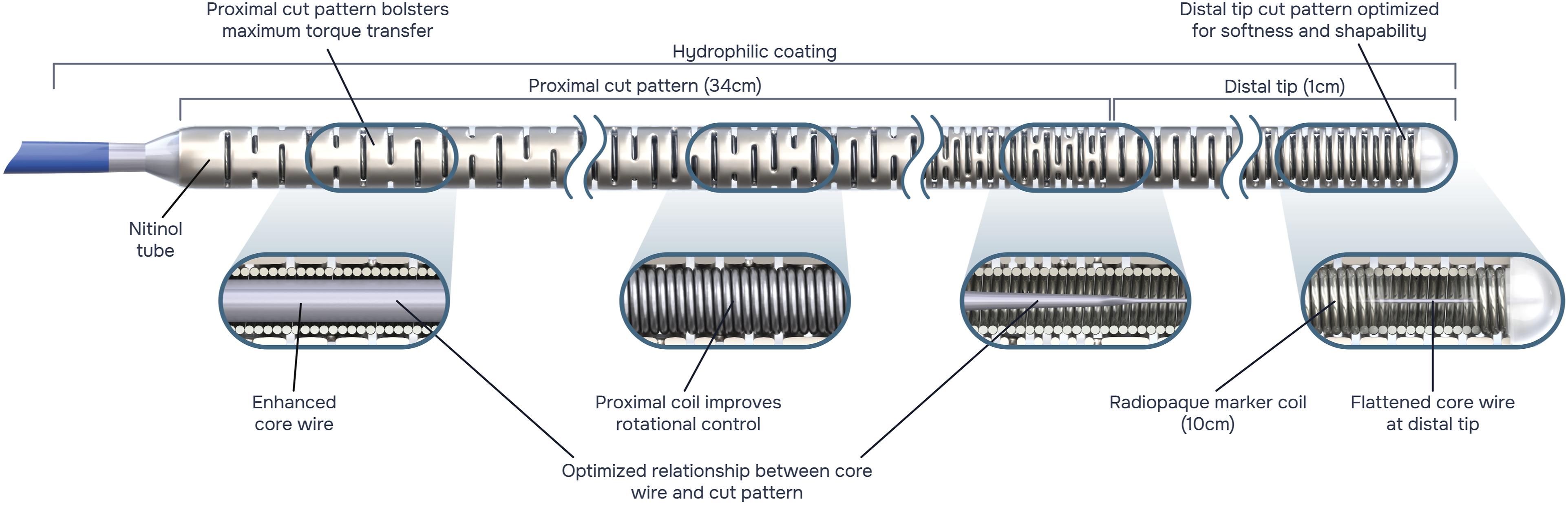
Ledge effect
A recent retrospective study in adult patients analysing Aristotle-18 and -24 wires in tracking catheters to reach a target vessel or aneurysm demonstrated a 100% cannulation success rate, 10 which was comparable to the same group’s success rate using 0.014in microwires. The authors of that study particularly noted the advantages of a reduced ‘ledge effect’ when using these 0.018in and 0.024in Aristotle wires for larger catheters during stroke thrombectomy and flow-diverter deployment procedures. 10 The reduced difference between the outer diameter of these larger wires and the inner diameter of the catheters results in reduced impaction of the catheter distal tip ledge upon a curved vessel wall (e.g. at the ophthalmic artery origin), thus improving trackability.
Reduced ledge-effect was also recently reported utilizing the newly introduced Aristotle 0.035-in macrowire to advance 0.088-in inner diameter aspiration catheters to the M1 segment of the middle cerebral artery during mechanical thrombectomy for acute ischaemic stroke. 11 These ledge-effect advantages are less relevant in PNI, where small microcatheters (<2.0 Fr distal OD) are predominantly utilized and in which stroke thrombectomy and flow-diverter deployment are relatively uncommon procedures.
However, ledge effect is still encountered in PNI when attempting to track a DMSO (dimethyl sulfoxide) compatible microcatheter over a 0.007in wire as opposed to a 0.014in wire, requiring additional forward load when tracking the microcatheter along the wire (see Figure 3). Such additional forward load can result in intra-procedural complications (including vasospasm and perforation) or failure to successfully track the microcatheter tip to the distal wire tip. In our practice, 0.014in wires were traditionally avoided during cannulation of distal or small intracranial vessels (e.g. tortuous posterior choroidal arterial feeders in VoGM, ophthalmic arteries in infants with retinoblastoma) due to concerns over distal wire stiffness and associated risks of vasospasm or perforation. Therefore, the ability to utilize a navigable softer 0.014in wire is of potential additional benefit in children by allowing for a reduced ledge effect. Schematic diagram demonstrating the reduced ledge gap within the lumen of a 0.017in inner diameter DMSO-compatible microcatheter when utilizing a 0.014 in microwire (such as the Aristotle-14) compared with using a 0.007 in microwire (Reproduced with permission from Scientia Vascular Inc). The distal tip softness of the Aristotle-14 allows the interventionist to minimize the ledge gap effect when tracking a DMSO-compatible microcatheter distally over the wire whilst maintaining a low wire-related pressure effect.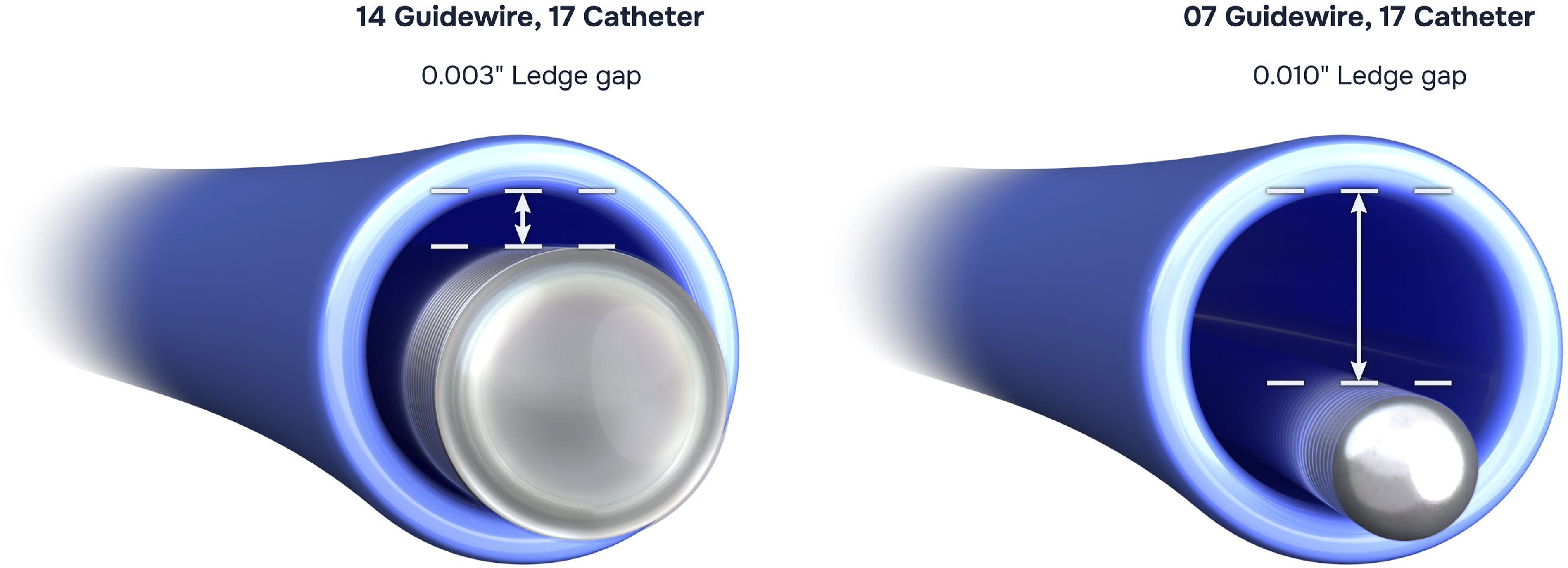
Distal tip softness
The distal tip softness in Aristotle wires is a design feature arising from the extensive transitions of the cut patterns in the distal aspect of the surrounding nitinol tube (see Figure 2). The softer tip results in reduced direct pressure upon the vessel wall compared with other wires (see Supplemental Figure 1).
In addition, cannulation of the cavernous segment of the ICA or ophthalmic artery origin in infants can trigger an autonomic reflex known as the oculo-respiratory reflex characterized by a rapid and dramatic reduction in lung ventilatory compliance (most often during IAC for retinoblastoma). 12 Whilst the aetiology of this reflex is unknown, it is likely to be triggered by the interaction of wires and catheters with sensory receptors in the vessel wall. 12 One of the wire-related complications encountered in our other wires group was an episode of the oculo-respiratory reflex during wire manipulation in the cavernous ICA (see Table 1). Thus, minimization of wire manipulation (through improved torque control) and wire pressure on the vessel wall (through distal tip softness) are potentially advantageous in this patient population.
Clinical implications of wire-related complications
Two patients undergoing embolization for VoGM in the other wires cohort required abandonment and rebooking of their procedures due to wire-related complications (vasospasm and superior ophthalmic vein rupture, respectively). Whilst no patients suffered long-term neurological sequelae from wire-related complications in either cohort, the potential for long-term disability exists both with vasospasm-related stroke and vessel rupture causing intracranial haemorrhage. Failed cannulation of target vessels may also delay or prolong necessary treatment in a vulnerable population, such as patients with VoGM who are at risk of developmental delay without appropriate intervention. As such, ongoing efforts are required in the field of PNI to improve technology and techniques that may minimize the occurrence of such complications and enhance cannulation rates.
Study limitations
This study has several limitations. The retrospective and single-centre nature of the study renders it prone to selection bias. We have attempted to limit the degree of bias by including consecutive cases utilizing the Aristotle wires and consecutive cases using other wires with an intervening crossover period across both cohorts during the transition in primary device utilization. Indeed, seven patients in the study underwent procedures across both cohorts, allowing for some degree of internal control. However, these cases that transitioned between other wires and Aristotle wires during the crossover period also introduce a degree of bias.
The binary nature of the primary outcome (successful cannulation of the target vessel – Yes/No) does not necessarily reflect the variability of factors that can impact vessel cannulation, such as partial cannulation, difficult cannulation, and vascular tortuosity. Objectively measuring the impact of such factors is difficult but the binary nature of the outcome used may overly simplify the process of cannulation.
The Aristotle wires cohort was older than the other wires cohort (p = .046). Intra-procedural complications are more common in neonates and infants than in older children which would be a potential confounding factor. However, age was not a significant predictor of successful cannulation on multivariable logistic regression analysis. Analysis of the age distributions between the two cohorts demonstrated that much of the difference resulted from the inclusion of multiple procedures within a one-week period in a neonate with life threatening high-output cardiac failure in the other wires cohort. This patient did not suffer any wire-related complications during those procedures, potentially reducing the impact of this confounder.
Whilst we have attributed the improved target vessel cannulation and reduced wire-related complication rates in the Aristotle wires cohort to design features of the wire, other factors may have also contributed to these results. These other factors would include increased procedural experience of the interventionists over time with associated improved skillsets and reduced complication rates, given that the start of the control cohort inclusion period preceded that of the case cohort, and the older mean age of the case cohort.
Conclusion
Aristotle wires were significantly more successful in achieving target vessel cannulation during paediatric neuro-interventional procedures than other wires. Intra-procedural vasospasm and other wire-related complications were also lower with Aristotle wires. These findings suggest that the design features of Aristotle wires, including improved torque control and distal tip softness, are advantageous in children. A prospective study would be useful for further assessment.
Supplemental Material
Supplemental Material - Aristotle wires for cannulating target vessels in paediatric neuro-interventional procedures: A case-control study
Supplemental Material for Aristotle wires for cannulating target vessels in paediatric neuro-interventional procedures: A case-control study by KD Bhatia, T Blane, B Giarola, J Vedamuthu, V Carraro Do Nascimento, Y-J Kim, G Olsson and M Dexter in The Neuroradiology Journal.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Supplemental Material
Supplemental Material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.