
Abstract
Background and purpose
Parathyroid carcinoma is the rarest endocrine neoplasm with very few published data discussing its imaging appearance with primary focus on ultrasound imaging features. We present our 23 years institutional experience to highlight multimodality imaging evaluation at presentation and at recurrence.
Material and Methods
Retrospective chart review of clinical and pathological diagnosis of parathyroid carcinoma patients presented for initial or recurrent disease management at M.D. Anderson Cancer Center between the period of January 2000 and February 2023 was performed. Imaging findings on US, CT, PET/CT, and technetium-99m sestamibi were analyzed for initial and local recurrent parathyroid carcinoma. We further assess patterns of distant recurrence and its location.
Results
Twenty three patients with pathological and clinical diagnosis of initial (14 patients) or recurrent parathyroid carcinoma (14 patients) were included in this study. US findings of parathyroid carcinoma were larger lesions, increased/irregular vascularity, and non-circumscribed margins. Multiphasic CT findings of parathyroid carcinoma included an arterially enhancing lesion that is hypoenhancing relative to the thyroid and demonstrates no washout on delayed imaging. Highly suggestive findings for recurrent disease included a hypoechoic solid nodule (91.67%) with increased vascularity on ultrasound (81.8%) with corresponding enhancement on CT.
Conclusion
Parathyroid carcinoma is a rare malignancy often diagnosed after surgical resection. We provided CT and US imaging features that are helpful in suggesting the diagnosis of parathyroid carcinoma and detection of early local recurrence.
Keywords
Introduction
Parathyroid carcinoma is the rarest endocrine neoplasm and one of the rarest reported malignancies in the US with a reported prevalence of 0.005% of all malignancies with an estimated incidence of 0.015.1–3 Most cases present as hyperparathyroidism, with approximately 90% of parathyroid carcinomas being hormonally functional. 4 However, parathyroid carcinomas account for less than 1% of all hyperparathyroidism cases.1,5,6 Parathyroid carcinomas mostly occur sporadically but are associated with other syndromes such as hyperparathyroidism-jaw tumor syndrome (HPT-JT) and endocrine disease such as familial isolated hyperparathyroidism and multiple endocrine neoplasia type 1 (MEN1).7–9
Diagnosis and staging of parathyroid carcinomas remain significantly challenging. The eighth edition, most recent, of The American Joint Committee on Cancer staging manual was the first to put forward a proposed staging of the disease. 10 However, clinical diagnosis remains significantly challenging due to the significant overlap of clinical, laboratory, and imaging features of the diseases with the much more common parathyroid adenoma/hyperplasia with diagnosis usually achieved only after pathological sample assessment.6,11–13
Significant advancement in imaging of primary hyperparathyroidism and availability of multiple modalities including ultrasound (US) with doppler imaging, technetium-99m sestamibi (⁹⁹ᵐTc-MIBI), and multiphasic (4D-CT) have allowed for excellent localization of parathyroid lesions with reported sensitivity and specificity of 4D-CT of 90.4% and 100% in some studies. 14 However, despite this excellent imaging localization of parathyroid lesions, discrimination of parathyroid adenoma/hyperplasia and parathyroid carcinoma remains challenging and is limited.3,6
Few case reports and case series have assessed the imaging appearance of parathyroid carcinomas and these have primarily focused on US with the majority comparing adenomas to carcinomas.15–18 However, there remains lack of data on CT imaging of parathyroid carcinoma despite recent data suggesting its superior sensitivity and specificity to US and ⁹⁹ᵐTc-MIBI. 14 Furthermore, there is significantly limited data in the radiology literature addressing the imaging appearance of local recurrence and distant metastasis patterns.
We present our institution experience with this rare disease over 23 years with an emphasis on the multimodality imaging appearance of initial and recurrent disease.
Methods
This retrospective study was approved by the institutional board review at MD Anderson Cancer Center (MDACC).
Patient Selection and Clinical Data
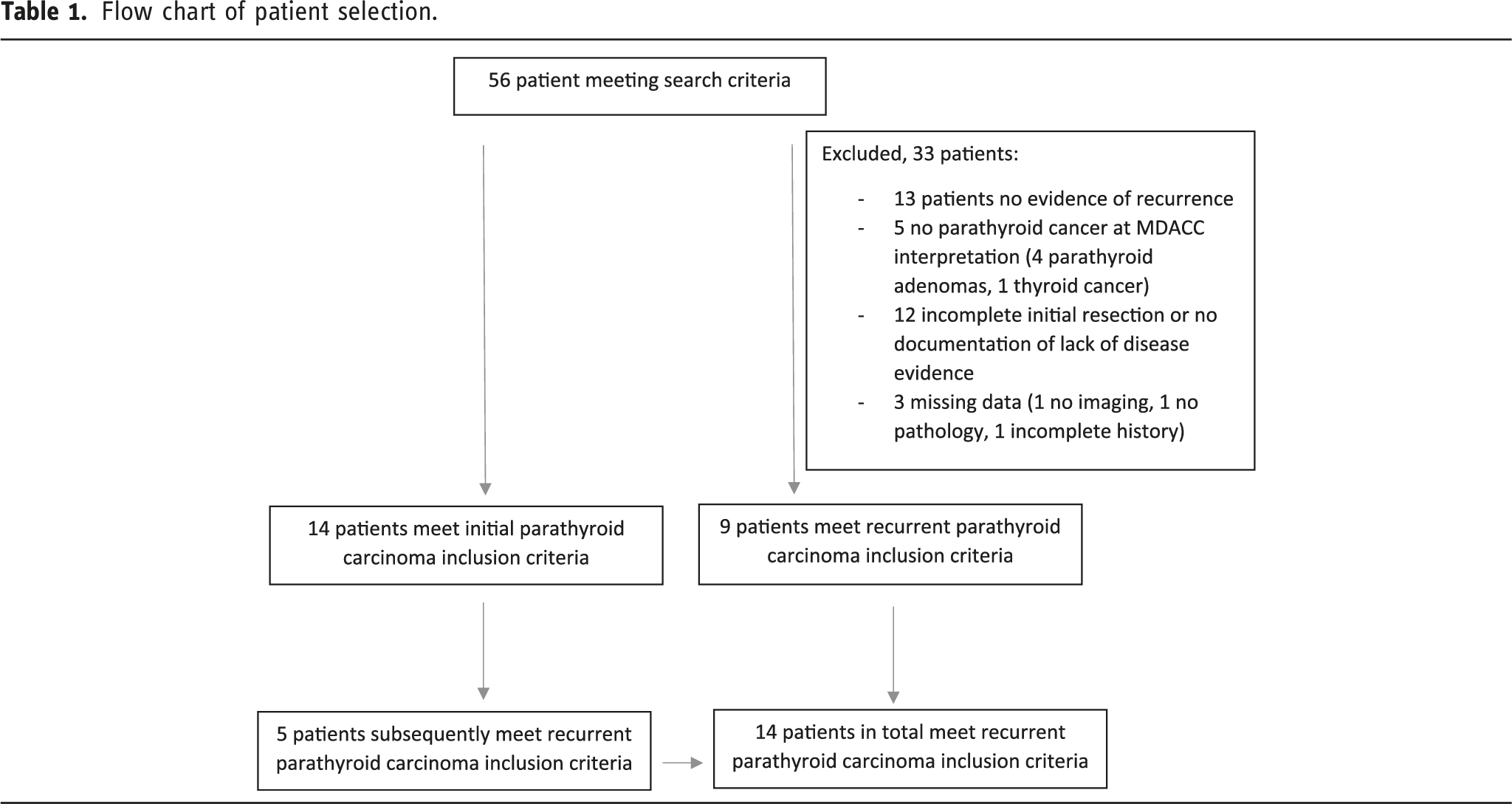
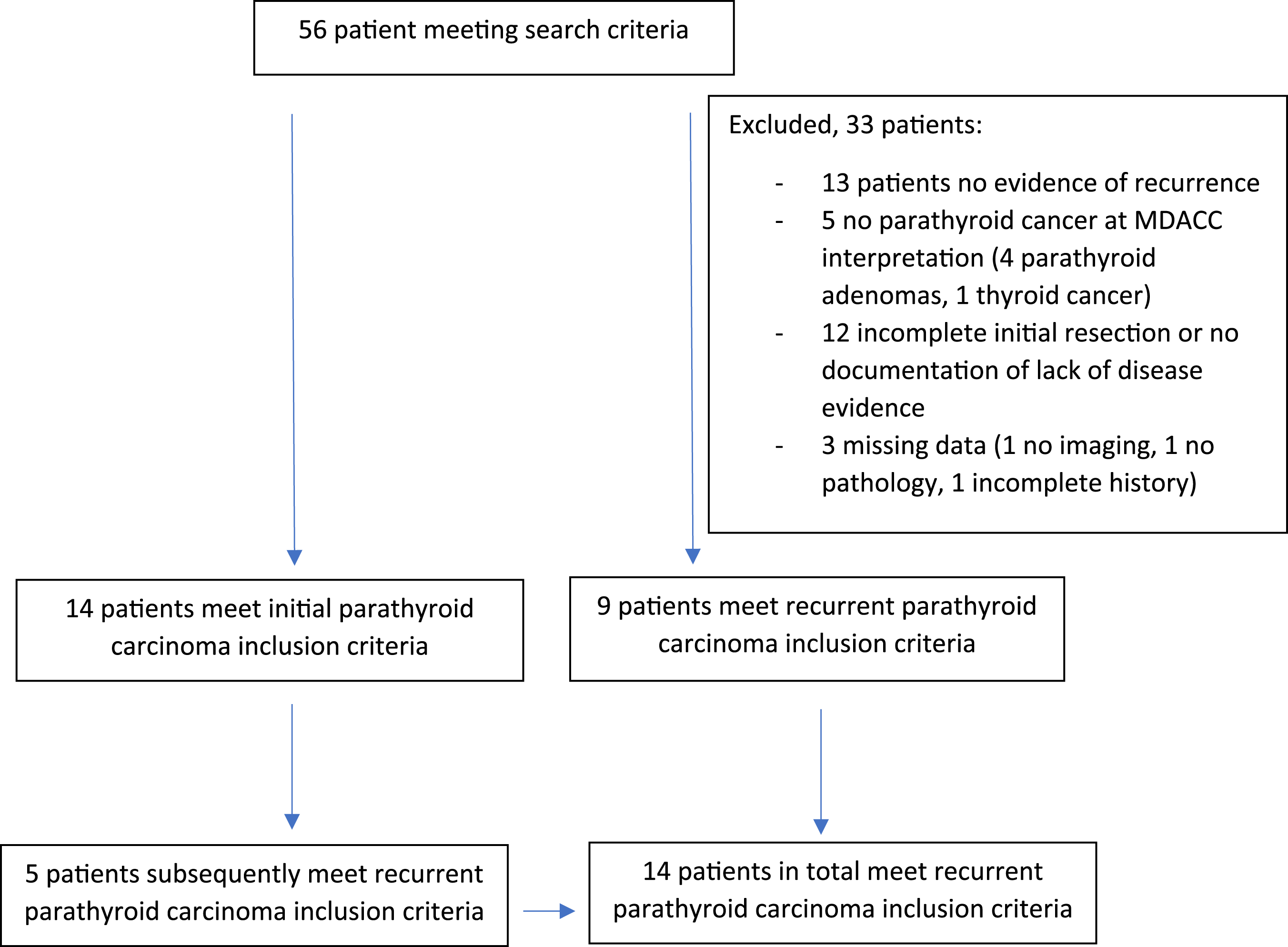
Flow chart of patient selection.
Careful review of the data to ensure clinical documentation of lack of residual disease after initial surgical resection was performed and only such patients were included in the recurrence subset. Similarly, only patients with clinical and radiographical diagnosis of remission after treatment were included.
The electronic medical records of patients were accessed and demographic and clinical data for each patient were collected, including age at diagnosis, gender, tumor location, and presenting symptoms, available imaging and pertinent laboratory data (intact PTH, calcium, and renal function). Patient risk factors and presence of syndromes such as MEN1 were recorded when present.
Imaging Review
All neck US and CT imaging characteristics were reviewed by two fellowship trained neuroradiologists with 4 years’ (R.E.) and 5 years’ experience (S.C). Both readers were blinded to the radiology reports and to each other’s interpretation.
Imaging was assessed for initial tumor detection and surveillance by either US and/or CT neck and ⁹⁹ᵐTc-MIBI and staging studies using CT chest, abdomen, and pelvis, and PET/CT.
US Imaging Review
All gray scale and color doppler ultrasound images of the neck were assessed for echogenicity (hypoechoic, isoechoic, and heterogenous relative to the thyroid), margin (smooth, micro lobulated, or irregular), tumor size (measured in three orthogonal planes, anteroposterior, transverse, and craniocaudal dimensions), and vascularity (absent or present). Margins were defined as smooth versus non-smooth (irregular and micro lobulated); if a lesion had more than 1 margin, appearance of the most worrisome margin was considered. Pattern of vascularity was reported as polar/feeding vessel or irregular/increased. US composition as solid, cystic, mostly solid (>90% solid), mixed cystic, and solid (<90% solid) was also assessed. If present, calcifications were recorded as micro or macro calcifications.
For assessment of local recurrence, margins of the lesions were not assessed given surrounding scarring/irregular appearance of the resection bed and small size of the recurrent lesions making it challenging to assess margins.
CT Neck Imaging Review
CT neck was noted if the exam was single phase routine contrast-enhanced or multiphasic 4D CT. CT images were assessed for enhancement, tumor size (measured in three orthogonal planes), appearance (solid/mostly solid, cystic, or mixed), and calcification (present or absent). Enhancement was assessed as a 2-step approach. First, lesions were visually inspected as demonstrating enhancement, defined as increased visual density relative to lymph nodes. Second, for multiphasic CT in subset 1, Hounsfield unit measurements were performed on all phases for the thyroid and parathyroid carcinoma. Hounsfield units mean values were recorded, and assessment for enhancement and washout of parathyroid was performed using an unpaired t test exam. The Hounsfield Unit was measured on all phases of the mass and the adjacent thyroid. Region of interest measurements were performed on solid homogenous enhancing components of at least 1 cm in size, where there were no or minimal streak artifact on all phases for both the thyroid and the lesion with similar size region of interest for both. These values were recorded for each phase and compared. Both readers measured the region of interest within the parathyroid carcinoma, and a mean value was generated for statistical analysis.
For detection of local recurrence, the enhancement of the lesion was reported as present or absent relative to adjacent cervical lymph nodes and CT ability to detect lesions relative to US.
Technetium-99m sestamibi Review
Acquisition of technetium-99m sestamibi study (with or without single photon emission computed tomography, SPECT) was assessed for identification of initial tumor localization and for detection of metastasis.
PET/CT Imaging Review
[1⁸F]FDG/PET and 68Ga-DOTATATE PET/CT were assessed in recurrent disease only for the successful detection of local disease and distant metastasis. PET/CT was not assessed in initial presenting disease as most cases did not have PET/CT prior to resection and none had distant metastasis at initial staging. Both tracers were assessed for ability to demonstrate local recurrence and distant recurrence. This was assessed as overall visualization of the lesion and the presence of avidity, defined per initial report. When both studies were present, comparison between both for detection and avidity was performed.
Statistical Analysis
The mean and standard deviations of pertinent data was calculated and reported in the result section. An interobserver agreement, Cohen Kappa, was calculated for each US and CT imaging characteristics. Disagreements were resolved by consensus agreement. An unpaired two sample t test assuming unequal variances was utilized to determine the p-value and assess for significant difference between the thyroid and parathyroid carcinoma Hounsfield Units values on precontrast, arterial, and delayed 4D-CT phases.
Results
A total of 23 patients are included in this study (Table 1). Subset 1 has 14 patients presenting with initial imaging of the parathyroid carcinoma. Subset 2 has 14 patients presenting with recurrent disease.
Patients’ Characteristics
18 of 23 patients (78.26%) had left-sided parathyroid carcinoma, four of 23 (17.39%) had right-sided parathyroid carcinoma, and 1/23 (4.35%) had a paratracheal/upper mediastinal midline parathyroid carcinoma.
Subset 1, initial tumor
Patients’ Characteristics
Demographic and clinical characteristic of patients with available initial Imaging.
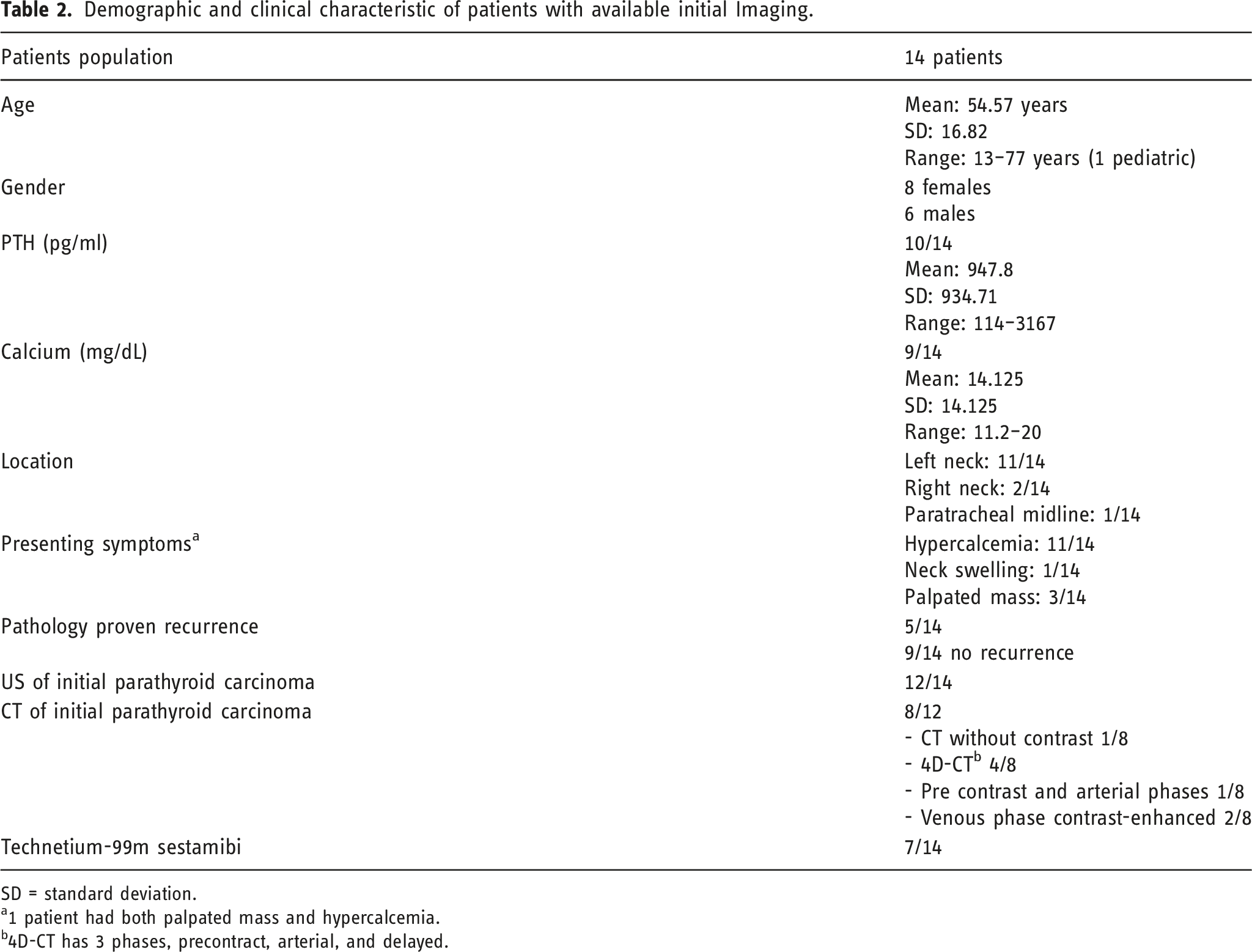
SD = standard deviation.
a1 patient had both palpated mass and hypercalcemia.
b4D-CT has 3 phases, precontract, arterial, and delayed.
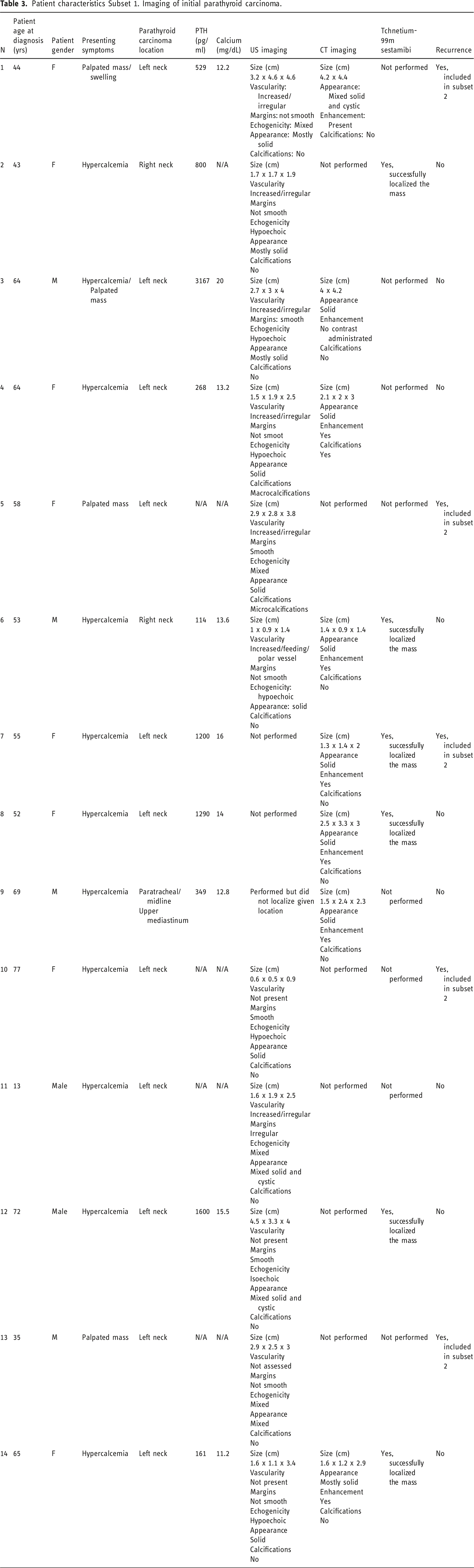
Patient characteristics Subset 1. Imaging of initial parathyroid carcinoma.
Ultrasound imaging findings
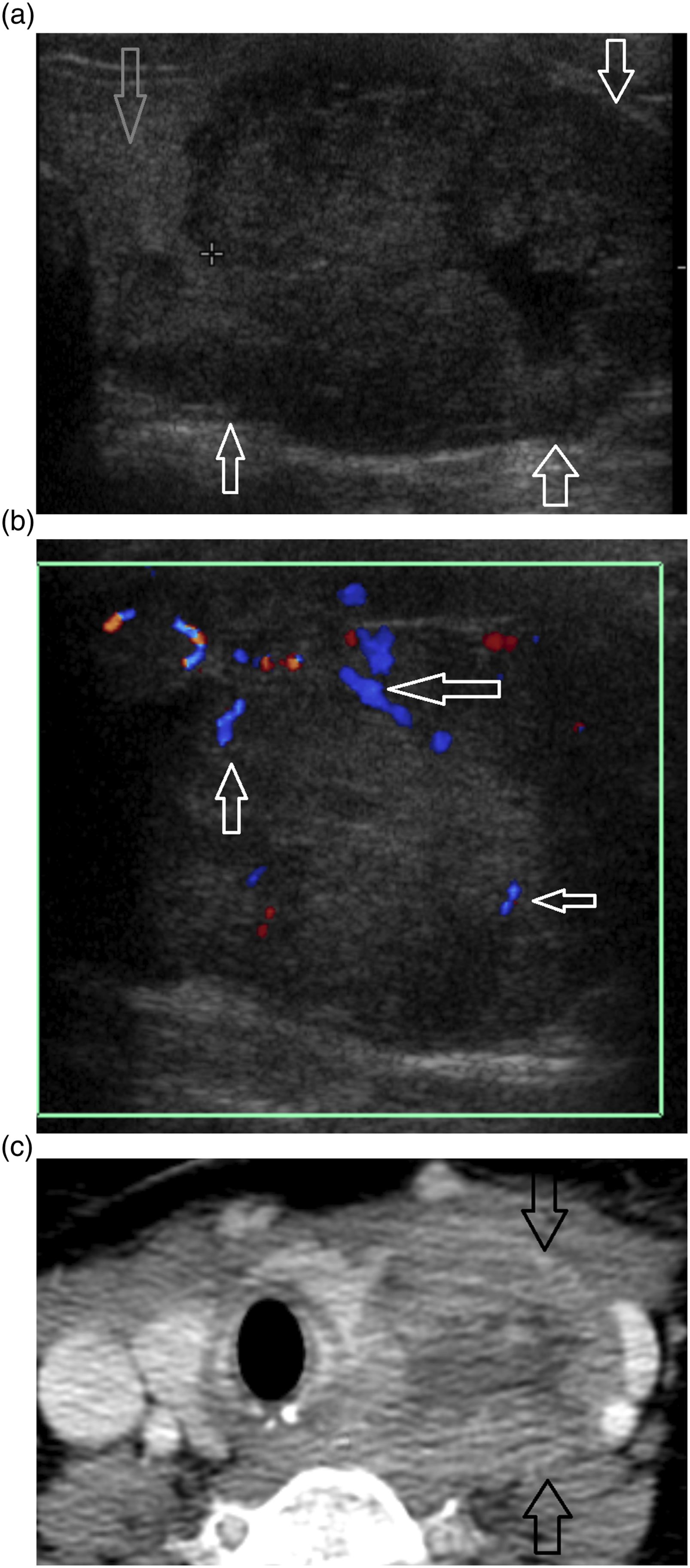
Ultrasound was performed in 12 of 14 patients (Table 3). Ultrasound was successful in localizing 11 of 12 parathyroid carcinomas. One patient had a paratracheal/upper mediastinal parathyroid carcinoma that was too inferior and deep to be visualized by the ultrasound (Figures 1 and 2). CT and US imaging of initial parathyroid carcinoma. Patient 6. Right-sided parathyroid carcinoma. (a) Gray scale US in long plane demonstrates isoechoic non-smooth lesion (arrow). (b) Doppler US shows increase vascularity with a polar/feeding vessel (arrow). US imaging appearance overlaps parathyroid adenoma. (c-e) CT demonstrates a pattern of enhancement atypical to that of parathyroid adenoma with precontrast lesion hypoattenuating relative to the thyroid (c), demonstrating arterial enhancement that is hypoenhancing relative to the thyroid (d), with no significant washout on delayed images (e) (black arrows parathyroid carcinoma, gray arrows right thyroid lobe). CT and US imaging of initial parathyroid carcinoma. Patient 1. (a). Gray scale US demonstrates hypoechoic mostly solid parathyroid carcinoma (black arrows) posterior and lateral to the left thyroid lobe (gray arrow). (b) Doppler US demonstrates increase in irregular vascularity of the lesion (arrows). (c) Postcontrast venous phase CT images demonstrate a mixed solid and cystic enhancing lesion (arrows) displacing the left thyroid lobe.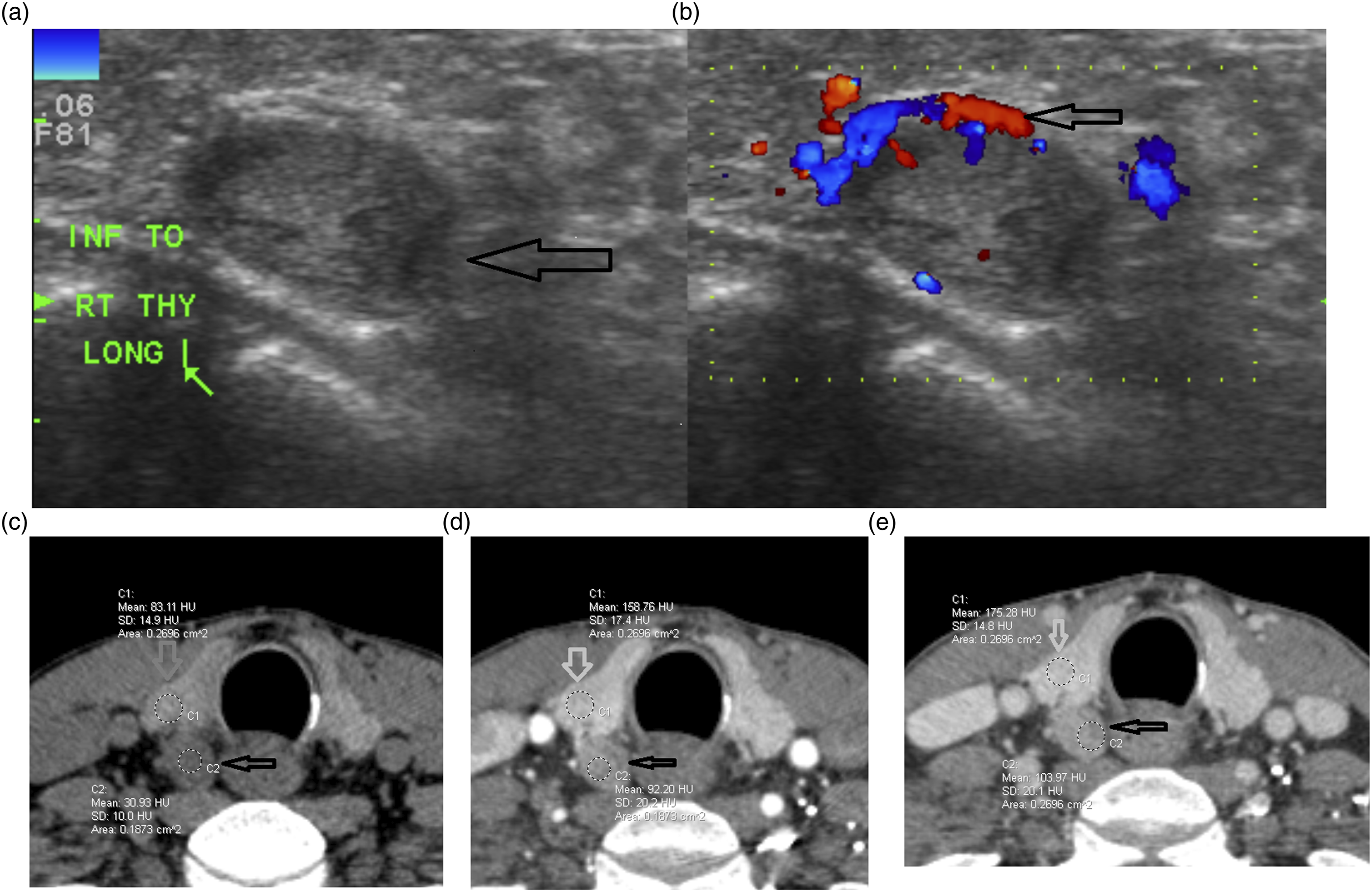
Size
The mean transverse size was 2.2 cm (SD 1.14), long short axis 2.2 cm (SD 1.19), and long long axis 2.91 cm (SD 1.18).
Vascularity
Available Doppler US of 10 patients showed increased irregular vascularity of parathyroid carcinoma in seven patients, with one patient also demonstrated a feeding/polar vessel. The remainder three patients had no increased vascularity.
Margins
In total, all 11 lesions were assessed, and four lesions had smooth margins and seven had non-smooth margins.
Echogenicity
No lesion was hyperechoic relative to the thyroid. Six lesions were hypoechoic, one was isoechoic, and four were mixed.
Appearance
US appearance was assessed in all 11 patients. Five patients had a solid lesion, three patients had mostly solid pattern, and three had mixed appearance.
Calcification
In total, two patients had calcifications. One patient had macro calcifications and one patient had micro calcifications.
Interobserver Agreement
Interobserver agreement and percent agreement was assessed for all imaging characteristics. Interobserver agreement was substantial for vascularity (0.79%, 90.9% agreement), echogenicity (0.63%, 81.8%), and appearance (0.79%, 90.9%). Interobserver agreement was perfect for calcifications (1%, 100%). Interobserver agreement for margins was slight for US margins (0.03%, 55.54%). This is explained by the challenging interpretation of lobulated margins as micro (not smooth) and macro (smooth).
CT imaging findings
In total, eight of 14 patients had CT imaging of the initial parathyroid carcinoma. Seven patients had contrast administered of which five had multiphasic CT. The five multiphasic CT exams included one patient that had precontrast and arterial exam and four patients that had 4D-CT (precontrast, arterial, and delayed (Figures 1 and 2).
Size
Anterioposterior mean size was 2.33 cm (SD 1.17), transverse mean size was 2.48 cm (SD 1.36), and craniocaudal mean size was 2.43 cm (SD 0.65).
Appearance
seven lesions demonstrated a solid/mostly solid appearance and one was mixed solid and cystic.
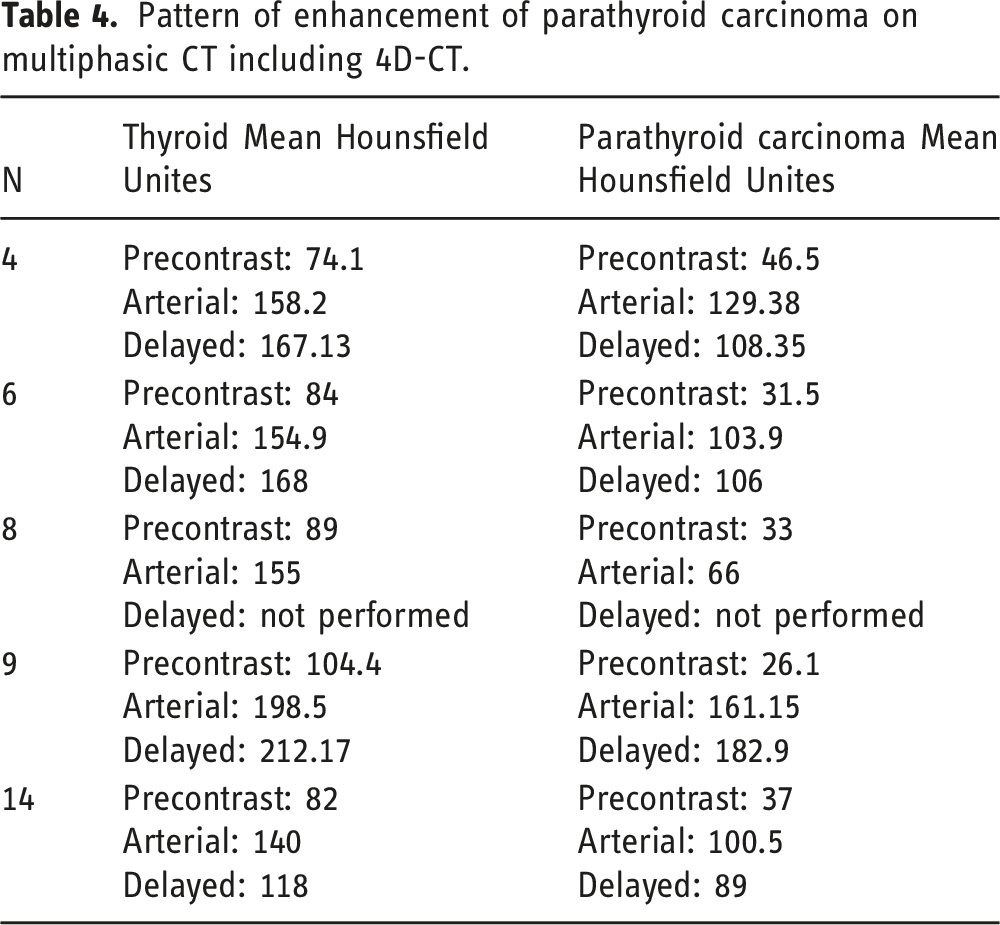
Pattern of enhancement of parathyroid carcinoma on multiphasic CT including 4D-CT.
Statistical significance in Mean Hounsfield Unit differences in parathyroid carcinoma based on contrast phase. p value < .05.
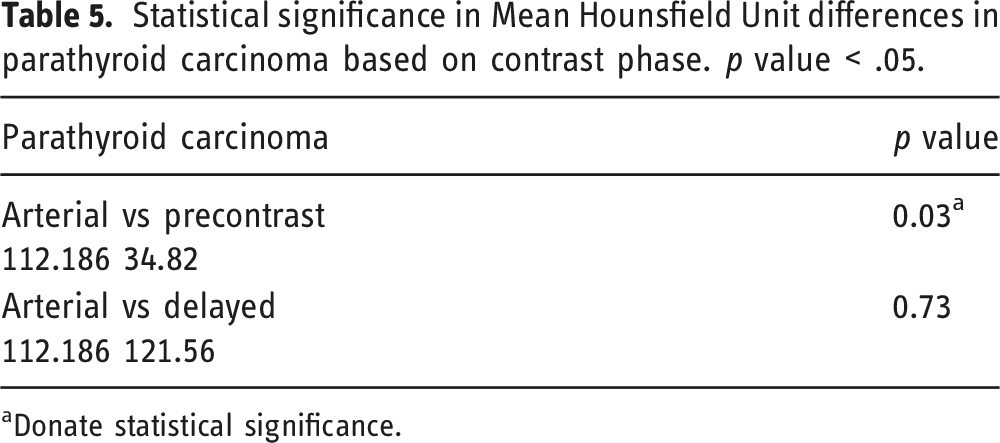
aDonate statistical significance.
Statistical significance in Mean Hounsfield Unit differences between thyroid gland and parathyroid carcinoma based on contrast phase. p value < .05
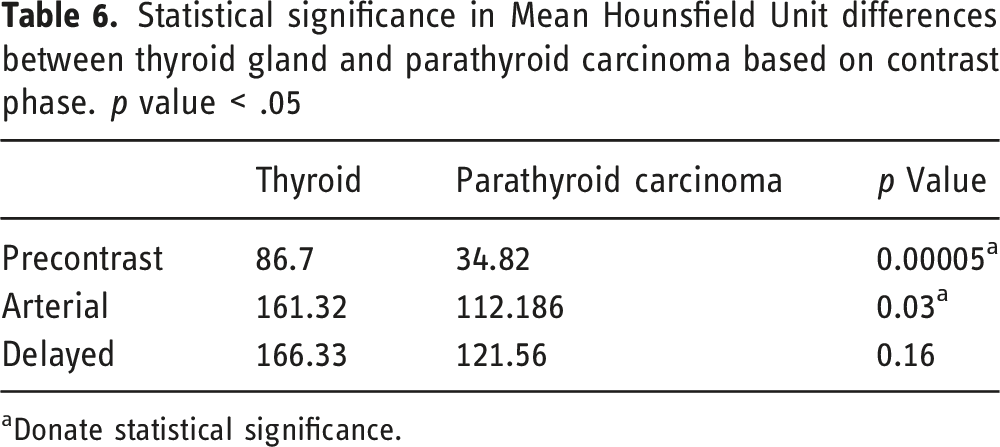
aDonate statistical significance.
Calcifications
Only one of eight patients had calcifications detected on CT and this corresponded to the macrocalcification noted on ultrasound.
Interobserver Agreement
Interobserver agreement and percent agreement was assessed for all imaging characteristics. Interobserver agreement was perfect for CT enhancement (1%, 100% agreement) and calcifications (1%, 100%). Interobserver agreement was moderate for CT appearance (0.6%, 87.5%)
⁹⁹ᵐTc-MIBI findings
⁹⁹ᵐTc-MIBI was performed in seven patients presenting with parathyroid carcinoma and was successful in localizing the parathyroid carcinoma in all 7 cases.
Subset 2, recurrent tumor
Patients’ Characteristics
Demographic and clinical characteristics of patients presenting with recurrence.
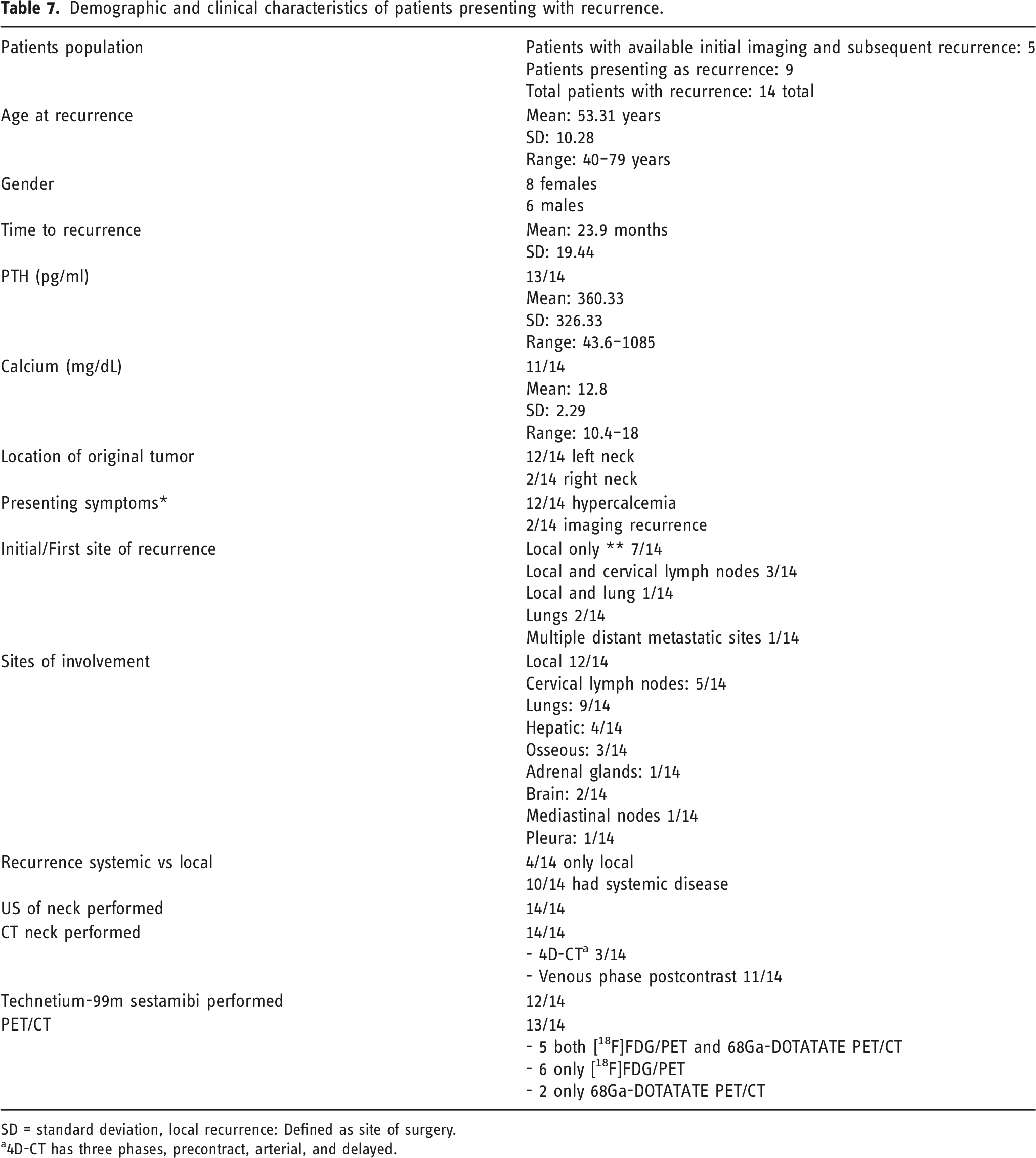
SD = standard deviation, local recurrence: Defined as site of surgery.
a4D-CT has three phases, precontract, arterial, and delayed.
Patient characteristics Subset 2. Imaging of recurrent parathyroid carcinoma.
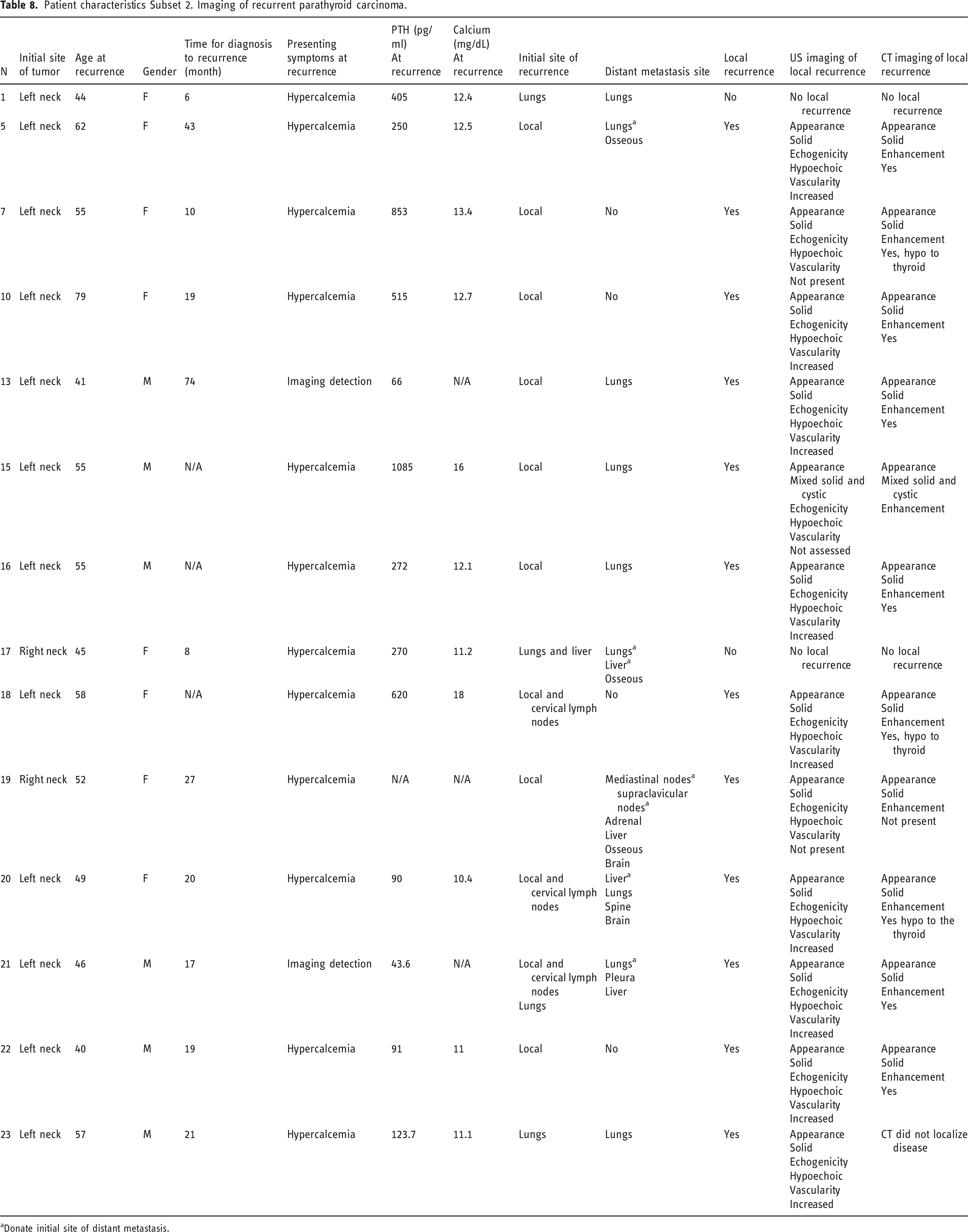
aDonate initial site of distant metastasis.
Ultrasound imaging findings
US was assessed in all 12 patients. 11 patients had small (less than 2 cm) solid, hypoechoic recurrence (Figure 3). Nine patients had increased vascularity, and two patients did not demonstrate increased vascularity of the hypoechoic solid nodule. One patient had a large mixed solid and cystic recurrence. Interobserver agreement was perfect for all three assessed US characteristics (1%, 100% agreement). US and CT images of recurrent disease. Patient 5 subset 2. (a) Gray scale US in long shows a hypoechoic solid nodule within the left side surgical bed (arrow). (b) Doppler US demonstrates increase in irregular vascularity of the lesion (arrows). (c) Arterial phase CT demonstrates multiple enhancing recurrent lesions in the left surgical bed including the US nodule medial to the vessel corresponding to the lesion noted on US (arrows).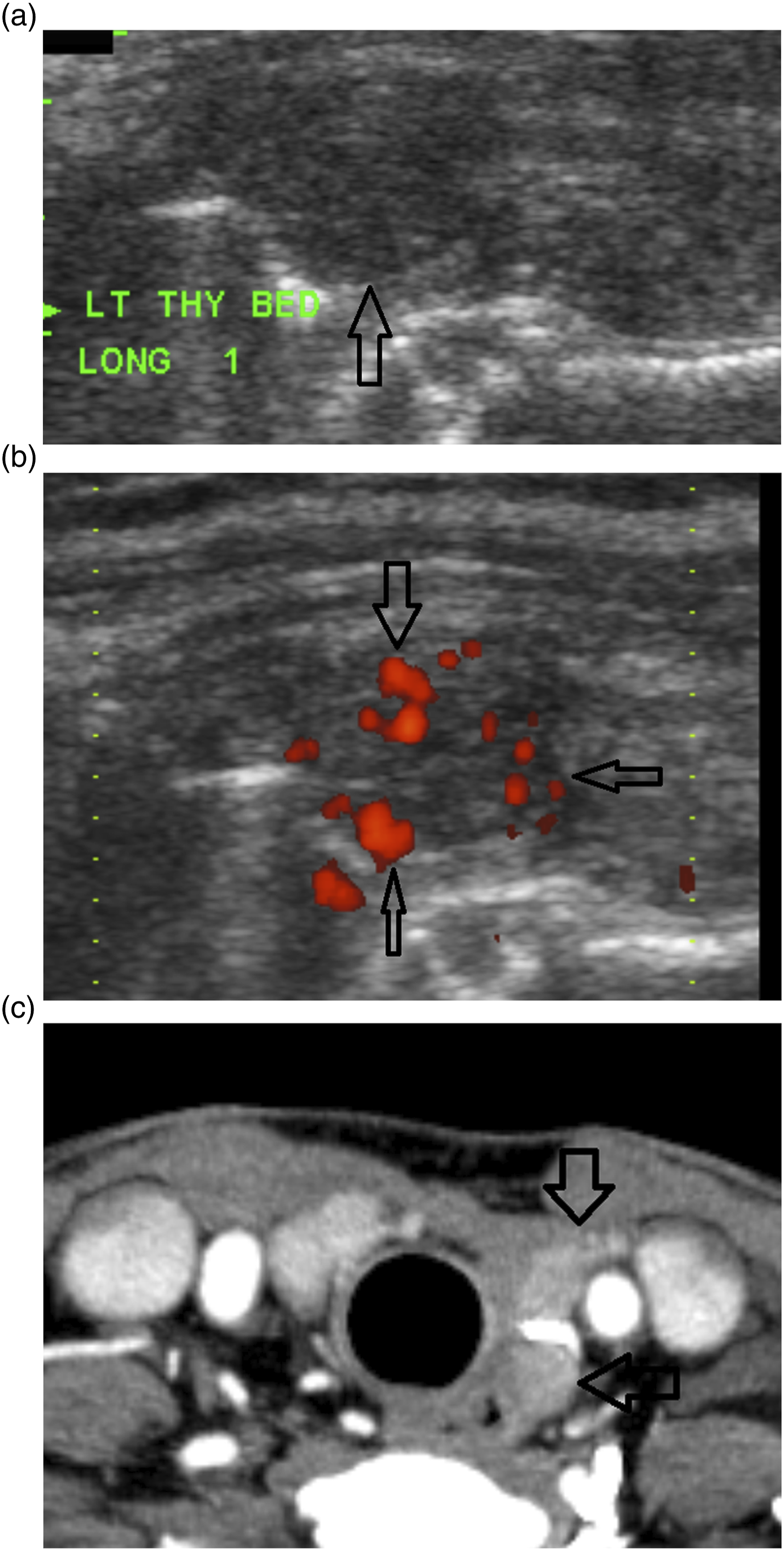
CT imaging findings
All 12 patients had CT of the neck for assessment of local recurrence. In 1 patient, enhancement was not able to be assessed. CT localized initial recurrence in 10 patients and failed to localize initial recurrence in two patients. CT subsequently visualized the lesion in one of the two patients as the lesion increased in size.
Appearance
In 11 patients, the lesion was solid and small, less than 2 cm. This includes the patient with the initial recurrence not localized on CT. In one patient, the recurrence was a large mixed solid and cystic lesion.
Enhancement
In 1 patient, assessment for enhancement was not feasible. In the remaining 11 visualized recurrences, nine demonstrated enhancement (diffuse or heterogenous) relative to the adjacent lymph nodes (Figure 3). Three patients had 4D-CT with imaging pattern like the one reported above in subset 1. However, this was not reported given that the initial lesion was either not imaged (in cases of referred recurrence) or did not have multiphasic CT of the initial lesion.
Interobserver Agreement
Interobserver agreement and percent agreement was assessed for all CT imaging characteristics. Interobserver agreement was perfect for appearance (1%, 100% agreement). Interobserver agreement for enhancement could not be calculated, but agreement was significant, 90.9%.
⁹⁹ᵐTc-MIBI findings
⁹⁹ᵐTc-MIBI was performed in 12 patients with recurrent parathyroid carcinoma. ⁹⁹ᵐTc-MIBI was successful in localizing local recurrence or distant metastases in 10 patients. ⁹⁹ᵐTc-MIBI failed to detect local recurrence in 2 cases.
PET/CT Imaging Findings
[1⁸F]FDG/PET and 68Ga-DOTATATE PET/CT Imaging Findings in Subset 2:
In total, 13 patients with recurrent disease had PET/CT imaging for staging. These were obtained at variable time in the recurrent disease course. Five patients had both [1⁸F]FDG/PET and 68Ga-DOTATATE PET/CT, six patients had only [1⁸F]FDG/PET, and two patients had 68Ga-DOTATATE PET/CT. PET/CT data was heterogenous as PET/CT was acquired at different stages of the recurrence, and in some cases, 68Ga-DOTATATE PET/CT was obtained later in the disease course relative to the [1⁸F]FDG/PET that has been utilized for longer time period.
In total, [1⁸F]FDG/PET was acquired in 7 cases with active local disease. [1⁸F]FDG/PET was not successful in visualizing local disease in four patients given small size. However, [1⁸F]FDG/PET was able to subsequently visualize one local disease as it got larger.
[1⁸F]FDG/PET was obtained in 10 patients with distant metastasis. [1⁸F]FDG/PET detected distant disease in nine patients with six patients demonstrating avidity of their lesions and 3 with no increase tracer avidity given small size of lesions (all lungs) but the lesions were detected on accompanying low-dose CT scans.
68Ga-DOTATATE PET/CT was obtained in seven patients. Five patients had local disease at time of 68Ga-DOTATATE PET/CT acquisition. 68Ga-DOTATATE PET/CT demonstrated increase tracer avidity in 2 cases. In the three other small local recurrences, 68Ga-DOTATATE PET/CT did not demonstrate increase tracer avidity but the accompanying low-dose CT scans detected the lesions. 68Ga-DOTATATE PET/CT was acquired in seven patients with distant metastasis at the time of scan. 68Ga-DOTATATE PET/CT demonstrated increase tracer avidity in two patients. In the remaining five patients, the accompanying low-dose CT scans visualized the lesions, lung nodules, but these were too small for PET resolution to demonstrate increase avidity.
In five patients, both [1⁸F]FDG/PET and 68Ga-DOTATATE PET/CT were acquired. Four patients have both scans acquired within the same time frame, within a month of each other, allowing for comparison. In 2 patients, both PET tracers demonstrated increase tracer avidity in distant metastatic lesions. In 1 patient, [1⁸F]FDG/PET demonstrated increase tracer avidity, while 68Ga-DOTATATE PET/CT did not demonstrate increase tracer avidity. In 1 patient, [1⁸F]FDG/PET did not see the local recurrence, while 68Ga-DOTATATE PET/CT localized the local recurrence on low-dose CT but did not demonstrate increase tracer avidity.
Discussion
Parathyroid carcinoma is one of the rarest malignancies and causes of parathyroid gland disease. 19 Although the first case was described in 1909, given its rarity, the literature remains lacking regarding this entity with less than 1000 cases reported in the literature. 20 Imaging data on parathyroid carcinoma is even less available, in particular, CT imaging of primary disease and imaging of recurrent disease.
Our case series presented multimodality imaging findings in 23 parathyroid carcinoma patients; 14 patients presenting with initial parathyroid carcinoma and 14 patients with recurrent disease. Multiple interesting observations were noted. First, most of the cases had a left-sided parathyroid carcinoma as 18 of 23 patients presented with left gland tumor. This side prevalence of parathyroid carcinoma has not been reported before, and while this is a small case series with limited patients, this observation is worth further assessment in future studies. Second, the most common presenting symptom at initial diagnosis and recurrence was hypercalcemia. However, at initial presentation, hypercalcemia was symptomatic, while at recurrence, it was mostly laboratory. This is consistent with the fact that treated parathyroid carcinoma is frequently monitored with calcium and PTH levels. Our case series demonstrates the value of imaging monitoring of treated disease as in two cases imaging detected recurrence in patients with no evidence of local or lab recurrence. Lastly, local recurrence was the most common site of initial and overall recurrence. Distant metastasis has been reported to occur via hematogenous spread in up to 25% of cases.21,22 In our case series, 71.43% developed distant metastasis with lungs being the most common site.
Ultrasound imaging of the initial parathyroid carcinoma demonstrated typically a large lesion, hypoechoic or of mixed echogenicity relative to the thyroid, increased mostly irregular vascularity, and lack of smooth margins. This is consistent with multiple previous studies that suggested larger size, irregular/increased vascularity, non-smooth margins, and calcifications as suspicious features.15–18,23 Our study did not demonstrate high number of calcified lesions on US as only two patients had calcification.
CT imaging of parathyroid carcinoma is poorly reported in the literature and to our knowledge there are no studies reporting parathyroid carcinoma enhancement pattern on multiphasic CT. Bahl et al reported three unique patterns of enhancement of parathyroid adenoma, reported as patterns A-C. 24 All three patterns demonstrated hypo enhancement to the thyroid on precontrast. Pattern A parathyroid adenomas demonstrated enhancement of the adenoma higher than the thyroid gland on arterial phase. Pattern B parathyroid adenomas did not demonstrate higher enhancement to thyroid on arterial phase but demonstrated lower attenuation on delayed phase. Lastly, pattern C did not demonstrate higher attenuation on arterial phase or lower attenuation on delayed phase to the thyroid. In this case series, parathyroid carcinoma demonstrated a pattern that is different than all patterns reported for parathyroid adenoma. Parathyroid carcinomas were hypodense to the thyroid and demonstrated arterial enhancement. However, unlike adenomas, the enhancement was lower than that of the thyroid and exhibited no significant washout relative to the thyroid gland on delayed phase. This pattern can be of great value for preoperative distinction between both adenoma and carcinoma and can help preoperative planning. 25 , 26
Local recurrent disease imaging characteristics are poorly studied and to our knowledge there is no multimodality imaging assessment of recurrent disease characteristics. In total, we present 12 cases of local recurrence in which both US and CT were acquired. US was successful in localizing all 12 recurrences, including all 11 small lesions. Our study suggests that a hypoechoic solid nodule with increased vascularity on US coupled with enhancement on CT should suggest recurrent disease until proven otherwise. An added value of our study is that the study suggests US as possibly the best initial modality for detection of small local recurrence as it was successful in localization of all local recurrences while CT was successful in 10 patients. Furthermore, increase radiotracer avidity in local recurrence was only noted in two of five patients on 68Ga-DOTATATE PET/CT and three of seven patients on [1⁸F]FDG/PET. This suggests that early recurrent disease might be challenging to detect on PET/CT given its relatively small size for the PET resolution to detect. Knowledge of the limitations and strengths of these imaging modalities and appearance of recurrence on each modality is of significance as two patients with recurrent disease had no evidence of local or lab recurrence.
Lastly, ⁹⁹ᵐTc-MIBI offers an excellent modality for localization of initial disease as it was successful in localizing initial disease in all patients it was acquired in. ⁹⁹ᵐTc-MIBI was also able to localize local or distant metastatic disease in 10 of 12 patients; it was acquired in while failing to detect local recurrence in two patients. However, one limitation of ⁹⁹ᵐTc-MIBI is its inability to distinguish adenoma from carcinoma on initial presentation (25-26).
Limitations of our study include the retrospective nature of this study. Another limitation is the relatively small size sample of the study. However, relative to other imaging studies, this is one of the larger data set. Also, given the rarity of parathyroid carcinoma, a large data set is hard to achieve. Another limitation is lack of complete data in all patients. This was partially offset by robust inclusion and exclusion criteria. Furthermore, the data set lacked complete genetic information on mutations and assessment for familial syndromes. This is in part due to a subset of older diagnosis. However, multiple endocrine neoplasia type 1 was diagnosed in two patients but this was not included in the analysis given lack of consistent analysis in all patients. Lastly, we did report two PET radiotracers, [1⁸F]FDG/PET and 68Ga-DOTATATE PET/CT, ability to detect local recurrence, and distant metastasis. However, this was limited by lack of consistent similar exam time frame acquisition and relatively small sample.
Conclusion
Parathyroid carcinoma is a very rare malignancy with paucity of data related to CT imaging of initial disease and overall limited imaging data of recurrent disease. This case series assess both imaging of initial and recurrent disease with suggestion of possible imaging markers that can help make the diagnosis. More collaborative studies are required to further validate these imaging markers in prospective future studies to aid the clinician with a confident preoperative diagnosis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.